Potrebbero piacerti anche
- Persons With Disabilities (PWD) Using The Services of A ScribeDocumento3 paginePersons With Disabilities (PWD) Using The Services of A Scribevedant patil. div ANessuna valutazione finora
- Scribe Notice 23112022Documento4 pagineScribe Notice 23112022rajNessuna valutazione finora
- FINAL CAT-III ADVT (2022) Final - 43-EndDocumento4 pagineFINAL CAT-III ADVT (2022) Final - 43-EndjackNessuna valutazione finora
- SavasabaDocumento3 pagineSavasababandivandana8Nessuna valutazione finora
- Migration Certificate PDFDocumento2 pagineMigration Certificate PDFdollarNessuna valutazione finora
- Annexure-II InstructionsDocumento3 pagineAnnexure-II InstructionsMadhu Sudhan GuptaNessuna valutazione finora
- Scribe Declaration FormDocumento2 pagineScribe Declaration Formthymoti patnalaNessuna valutazione finora
- Scribe Decalration FormDocumento2 pagineScribe Decalration Formsunil601Nessuna valutazione finora
- Appendix-I Application Form Officers Training Academy, Gaya (Bihar) - 823005Documento4 pagineAppendix-I Application Form Officers Training Academy, Gaya (Bihar) - 823005SaiiNessuna valutazione finora
- Bank of Baroda Recruitment of Specialist Officers Date of Examination: 17.03.2019Documento2 pagineBank of Baroda Recruitment of Specialist Officers Date of Examination: 17.03.2019Rudhra MoorthyNessuna valutazione finora
- Page 1 of 2)Documento5 paginePage 1 of 2)Pradeep KumarNessuna valutazione finora
- IGNOU B.ed Application Form 2018Documento6 pagineIGNOU B.ed Application Form 2018Manoj kumar shuklaNessuna valutazione finora
- Scribe FormDocumento2 pagineScribe FormSubhashreeNessuna valutazione finora
- National Agri-Food Biotechnology Institute (Nabi) : Form of Application For The Positions of ScientistDocumento4 pagineNational Agri-Food Biotechnology Institute (Nabi) : Form of Application For The Positions of ScientistShashank KatiyarNessuna valutazione finora
- Certificate FormatsDocumento12 pagineCertificate FormatsrajkalamaeroNessuna valutazione finora
- Additional Instructions in View of Covid 19Documento5 pagineAdditional Instructions in View of Covid 19pinninti rameshNessuna valutazione finora
- DTMF CoreDocumento6 pagineDTMF Corevara prasadNessuna valutazione finora
- Reserve Bank of India Guidelines For Visually Impaired or Orthopeadically Challenged CandidatesDocumento3 pagineReserve Bank of India Guidelines For Visually Impaired or Orthopeadically Challenged CandidatesKunaalNessuna valutazione finora
- Application Form With Annexures For MBA Admission 2020Documento9 pagineApplication Form With Annexures For MBA Admission 2020Soumalya TalapatraNessuna valutazione finora
- Generic Sribe Declaration FormDocumento3 pagineGeneric Sribe Declaration Formstvmas21Nessuna valutazione finora
- Scribe FormDocumento2 pagineScribe FormSatish MekalaNessuna valutazione finora
- Main Exam Scribe Declartion Form PDFDocumento2 pagineMain Exam Scribe Declartion Form PDFManju KiranNessuna valutazione finora
- Migration Certificate University To UniversityDocumento2 pagineMigration Certificate University To Universitygirdhargopal87Nessuna valutazione finora
- InterviewDocumento4 pagineInterviewas9345667Nessuna valutazione finora
- TW-SH-CCIC Duplicate Certificate Proforma - 482.Documento4 pagineTW-SH-CCIC Duplicate Certificate Proforma - 482.Tirupati TirumalaNessuna valutazione finora
- PGIJBDocumento2 paginePGIJBKeerti PatelNessuna valutazione finora
- Scribe FormDocumento2 pagineScribe FormSankalp AgrawalNessuna valutazione finora
- State Bank of India Recruitment of Specialist Cadre Officer in State Bank of IndiaDocumento3 pagineState Bank of India Recruitment of Specialist Cadre Officer in State Bank of IndiaMuthukrishnanNessuna valutazione finora
- 1526463206558-Scribe FormDocumento2 pagine1526463206558-Scribe FormShub KumarNessuna valutazione finora
- Prescribed Proforma APPLICATION FOR THE POST OFDocumento3 paginePrescribed Proforma APPLICATION FOR THE POST OFBalaji Rao NNessuna valutazione finora
- National Agri-Food Biotechnology Institute (Nabi)Documento4 pagineNational Agri-Food Biotechnology Institute (Nabi)neeleshhh_pNessuna valutazione finora
- Scribe Declaration Form and GuidelineDocumento3 pagineScribe Declaration Form and GuidelineShubhanshu DwivediNessuna valutazione finora
- Scribe DeclarationDocumento2 pagineScribe DeclarationMuhammed AmeerNessuna valutazione finora
- Madurai Kamaraj University: Semester - Non SemesterDocumento3 pagineMadurai Kamaraj University: Semester - Non SemesterJones Jones Jr.Nessuna valutazione finora
- Application Forms Agniveervayu Non-Combatants 02 23Documento4 pagineApplication Forms Agniveervayu Non-Combatants 02 23sudeepchhetri41Nessuna valutazione finora
- UntitledDocumento5 pagineUntitledMuthu KumaranNessuna valutazione finora
- Application Form Photo CorrectionDocumento2 pagineApplication Form Photo CorrectionMuthu KumaranNessuna valutazione finora
- CUS Migration CertificateDocumento2 pagineCUS Migration CertificatezahidneakaNessuna valutazione finora
- Degree CertificateDocumento3 pagineDegree CertificatekarthiktkkNessuna valutazione finora
- Tripura Public Service Commission: Akhaura Road, Agartala - 799001. Application Form For RecruitmentDocumento4 pagineTripura Public Service Commission: Akhaura Road, Agartala - 799001. Application Form For RecruitmentSandip Kumar RoyNessuna valutazione finora
- Office of The Controller Examination Application Form For Obtaining Degree in AbsentiaDocumento2 pagineOffice of The Controller Examination Application Form For Obtaining Degree in AbsentiaAK KshatriyaNessuna valutazione finora
- IMA FormDocumento3 pagineIMA FormSandeep OdelaNessuna valutazione finora
- Scribe Form IIDocumento2 pagineScribe Form IILakshay KapoorNessuna valutazione finora
- Proforma of Application: For Office Use OnlyDocumento5 pagineProforma of Application: For Office Use OnlyBhim DasNessuna valutazione finora
- Proforma of Self Declaration For ScribeDocumento2 pagineProforma of Self Declaration For Scribevij2009Nessuna valutazione finora
- Irectorate of Istance Ducation: Deemed To Be University Established U/s 3 of UGC Act, 1956Documento4 pagineIrectorate of Istance Ducation: Deemed To Be University Established U/s 3 of UGC Act, 1956Rama KrishnaNessuna valutazione finora
- Application Form For MOT Course Session 2014-15Documento8 pagineApplication Form For MOT Course Session 2014-15scribidaccount1Nessuna valutazione finora
- 505 1 Medical Officer 2017Documento5 pagine505 1 Medical Officer 2017Vivek SinghNessuna valutazione finora
- Document Submission FormDocumento1 paginaDocument Submission FormChandra SinghNessuna valutazione finora
- PWWF Talent Scholarship Grant Checklist & Template FileDocumento21 paginePWWF Talent Scholarship Grant Checklist & Template Fileshahfaisal gfgNessuna valutazione finora
- Oil and Natural Gas Corporation Limited Western Onshore Basin: Vadodara Walk in Interview For Medics and Paramedics On Contractual BasisDocumento3 pagineOil and Natural Gas Corporation Limited Western Onshore Basin: Vadodara Walk in Interview For Medics and Paramedics On Contractual BasisAbhinav KumarNessuna valutazione finora
- Account Test For Headmaster and Headmistress Application FormDocumento7 pagineAccount Test For Headmaster and Headmistress Application FormNarasimha SastryNessuna valutazione finora
- Undertaking To Be Produced by The Candidates at The Time of AdmissionDocumento4 pagineUndertaking To Be Produced by The Candidates at The Time of AdmissionDida KhalingNessuna valutazione finora
- Recruitment Scribe Declaration Form Hindi Dab5724125Documento3 pagineRecruitment Scribe Declaration Form Hindi Dab5724125Eiknath ThakurNessuna valutazione finora
- Application Attestation FormDocumento1 paginaApplication Attestation FormSaravanan MRNessuna valutazione finora
- DIPLOMA Duplicate Proforma - 20.Documento3 pagineDIPLOMA Duplicate Proforma - 20.Tirupati TirumalaNessuna valutazione finora
- Foriegn National DevelopmentDocumento8 pagineForiegn National DevelopmentKirti VardhanNessuna valutazione finora
- Admit Card: Applicant's Name: Afcat No.Documento3 pagineAdmit Card: Applicant's Name: Afcat No.Srikanta NayakNessuna valutazione finora
- Insurance Broker: Passbooks Study GuideDa EverandInsurance Broker: Passbooks Study GuideNessuna valutazione finora
- The Addiction Counselor's Documentation Sourcebook: The Complete Paperwork Resource for Treating Clients with AddictionsDa EverandThe Addiction Counselor's Documentation Sourcebook: The Complete Paperwork Resource for Treating Clients with AddictionsNessuna valutazione finora
- YukonDocumento28 pagineYukonBhargav VekariaNessuna valutazione finora
- Post Office Monthly Income Scheme (POMIS) - Calculator: Interest Rate 7.70% Amount Invested (RS.) 100,000Documento3 paginePost Office Monthly Income Scheme (POMIS) - Calculator: Interest Rate 7.70% Amount Invested (RS.) 100,000Bhargav VekariaNessuna valutazione finora
- Line Plan XcracerDocumento1 paginaLine Plan XcracerBhargav VekariaNessuna valutazione finora
- Candidateapplicationform PDFDocumento2 pagineCandidateapplicationform PDFBhargav VekariaNessuna valutazione finora
- OfferTermsCondition2019 11 25 - 063147592 PDFDocumento1 paginaOfferTermsCondition2019 11 25 - 063147592 PDFBhargav VekariaNessuna valutazione finora
- Kessler 2-3may17 Workshop SSDocumento31 pagineKessler 2-3may17 Workshop SSBhargav VekariaNessuna valutazione finora
- National Rock Climbing Camp National Rock Climbing CampDocumento2 pagineNational Rock Climbing Camp National Rock Climbing CampBhargav VekariaNessuna valutazione finora
- Course Prog 2017-18Documento5 pagineCourse Prog 2017-18Bhargav VekariaNessuna valutazione finora
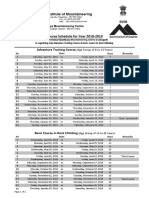
- Course Schedule For Year 2017-2018: Swami Vivekanand Institute of MountaineeringDocumento2 pagineCourse Schedule For Year 2017-2018: Swami Vivekanand Institute of MountaineeringBhargav VekariaNessuna valutazione finora
- Nehru Institute of Mountaineering Uttarkashi, Uttarakhand (India) - 249193Documento2 pagineNehru Institute of Mountaineering Uttarkashi, Uttarakhand (India) - 249193Bhargav VekariaNessuna valutazione finora
- Course Schedule For Year 2018-2019: Swami Vivekanand Institute of MountaineeringDocumento2 pagineCourse Schedule For Year 2018-2019: Swami Vivekanand Institute of MountaineeringBhargav VekariaNessuna valutazione finora
- FormDocumento2 pagineFormBhargav VekariaNessuna valutazione finora
- NIMAS Medical FormDocumento2 pagineNIMAS Medical FormBhargav VekariaNessuna valutazione finora
- Guwahati To Ahmedabad ParaglidingDocumento5 pagineGuwahati To Ahmedabad ParaglidingBhargav VekariaNessuna valutazione finora
- Sociology of Sport: Pamela SerraDocumento39 pagineSociology of Sport: Pamela SerraBhargav VekariaNessuna valutazione finora
- Swiggy Order 43333379786Documento2 pagineSwiggy Order 43333379786Bhargav VekariaNessuna valutazione finora
- Lithuania DalinaDocumento16 pagineLithuania DalinaStunt BackNessuna valutazione finora
- Duavent Drug Study - CunadoDocumento3 pagineDuavent Drug Study - CunadoLexa Moreene Cu�adoNessuna valutazione finora
- Syllabus DresserDocumento2 pagineSyllabus DresserVikash Aggarwal50% (2)
- What Is TranslationDocumento3 pagineWhat Is TranslationSanskriti MehtaNessuna valutazione finora
- Week 7 Sex Limited InfluencedDocumento19 pagineWeek 7 Sex Limited InfluencedLorelyn VillamorNessuna valutazione finora
- B122 - Tma03Documento7 pagineB122 - Tma03Martin SantambrogioNessuna valutazione finora
- Harper Independent Distributor Tri FoldDocumento2 pagineHarper Independent Distributor Tri FoldYipper ShnipperNessuna valutazione finora
- Vendor Information Sheet - LFPR-F-002b Rev. 04Documento6 pagineVendor Information Sheet - LFPR-F-002b Rev. 04Chelsea EsparagozaNessuna valutazione finora
- Companyprofil E: Erfanconstructionsolut IonDocumento14 pagineCompanyprofil E: Erfanconstructionsolut IonNurin AleesyaNessuna valutazione finora
- Snapdragon 435 Processor Product Brief PDFDocumento2 pagineSnapdragon 435 Processor Product Brief PDFrichardtao89Nessuna valutazione finora
- Functions in C++Documento23 pagineFunctions in C++Abhishek ModiNessuna valutazione finora
- 2009 2011 DS Manual - Club Car (001-061)Documento61 pagine2009 2011 DS Manual - Club Car (001-061)misaNessuna valutazione finora
- Post Appraisal InterviewDocumento3 paginePost Appraisal InterviewNidhi D100% (1)
- Stearns 87700 Series Parts ListDocumento4 pagineStearns 87700 Series Parts ListYorkistNessuna valutazione finora
- Hamstring - WikipediaDocumento21 pagineHamstring - WikipediaOmar MarwanNessuna valutazione finora
- Networker Performance Tuning PDFDocumento49 pagineNetworker Performance Tuning PDFHarry SharmaNessuna valutazione finora
- Chapter 3 - Organization Structure & CultureDocumento63 pagineChapter 3 - Organization Structure & CultureDr. Shuva GhoshNessuna valutazione finora
- 2SB817 - 2SD1047 PDFDocumento4 pagine2SB817 - 2SD1047 PDFisaiasvaNessuna valutazione finora
- Pt3 English Module 2018Documento63 paginePt3 English Module 2018Annie Abdul Rahman50% (4)
- The JHipster Mini Book 2Documento129 pagineThe JHipster Mini Book 2tyulist100% (1)
- SSGC-RSGLEG Draft Study On The Applicability of IAL To Cyber Threats Against Civil AviationDocumento41 pagineSSGC-RSGLEG Draft Study On The Applicability of IAL To Cyber Threats Against Civil AviationPrachita AgrawalNessuna valutazione finora
- SMC 2D CADLibrary English 1Documento590 pagineSMC 2D CADLibrary English 1Design IPGENessuna valutazione finora
- Heterogeneity in Macroeconomics: Macroeconomic Theory II (ECO-504) - Spring 2018Documento5 pagineHeterogeneity in Macroeconomics: Macroeconomic Theory II (ECO-504) - Spring 2018Gabriel RoblesNessuna valutazione finora
- Evaluation TemplateDocumento3 pagineEvaluation Templateapi-308795752Nessuna valutazione finora
- PSG College of Technology, Coimbatore - 641 004 Semester Examinations, SemesterDocumento3 paginePSG College of Technology, Coimbatore - 641 004 Semester Examinations, SemesterBabitha DhanaNessuna valutazione finora
- Technology Management 1Documento38 pagineTechnology Management 1Anu NileshNessuna valutazione finora
- De Thi Hoc Ki 1 Mon Tieng Anh Lop 5 Co File NgheDocumento10 pagineDe Thi Hoc Ki 1 Mon Tieng Anh Lop 5 Co File Nghetuyen truongNessuna valutazione finora
- SHCDocumento81 pagineSHCEng Mostafa ElsayedNessuna valutazione finora
- PED003Documento1 paginaPED003ely mae dag-umanNessuna valutazione finora
- B.SC BOTANY Semester 5-6 Syllabus June 2013Documento33 pagineB.SC BOTANY Semester 5-6 Syllabus June 2013Barnali DuttaNessuna valutazione finora