Potrebbero piacerti anche
- Diabetic KetoacidosisDocumento14 pagineDiabetic KetoacidosisYash RamawatNessuna valutazione finora
- DKADocumento64 pagineDKAAravindhan Gunasekaran PaediatricianNessuna valutazione finora
- Diabetic Ketoacidosis Case StudyDocumento6 pagineDiabetic Ketoacidosis Case StudyJohn AlcantaraNessuna valutazione finora
- Diabetic Ketoacidosis Case StudyDocumento5 pagineDiabetic Ketoacidosis Case Studyjc_albano29100% (7)
- Diabetic KetoacidosisDocumento16 pagineDiabetic Ketoacidosisjoyshe111100% (2)
- Diabetic Ketoacidosis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsDa EverandDiabetic Ketoacidosis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNessuna valutazione finora
- Diabetic KetoacidosisDocumento3 pagineDiabetic KetoacidosisJanna FavilaNessuna valutazione finora
- Diabetic KetoacidosisDocumento5 pagineDiabetic Ketoacidosislpickering33Nessuna valutazione finora
- Case Study 22 Diabetes I KNH 411Documento18 pagineCase Study 22 Diabetes I KNH 411api-30189722067% (3)
- Acute Lymphocytic LeukemiaDocumento7 pagineAcute Lymphocytic Leukemiamildred alidon100% (1)
- Diabetic Ketoacidosis (Dka)Documento16 pagineDiabetic Ketoacidosis (Dka)yazid100% (5)
- Case Study: Diabetic KetoacidosisDocumento66 pagineCase Study: Diabetic Ketoacidosisllaychin100% (2)
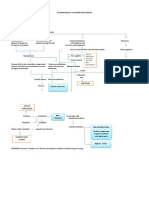
- Pathophysiology of Diabetic KetoacidosisDocumento1 paginaPathophysiology of Diabetic KetoacidosisSuzette PipoNessuna valutazione finora
- Diabetic Ketoacidosis PathwayDocumento22 pagineDiabetic Ketoacidosis PathwaySri Nath100% (1)
- DKADocumento12 pagineDKAAisha SyedNessuna valutazione finora
- Diabetic Ketoacidosis Written ReportDocumento19 pagineDiabetic Ketoacidosis Written ReportEros Victorino100% (2)
- Pathogenesis of Micro and Macrovascular Complications of DiabetesDocumento4 paginePathogenesis of Micro and Macrovascular Complications of DiabetesFrancesca LiNessuna valutazione finora
- Congestive Heart Failure 1 Concept Map !Documento1 paginaCongestive Heart Failure 1 Concept Map !Franklin A. Salaum IIINessuna valutazione finora
- ABC: Sickle-Cell Anemia, Shock, PoisoningDocumento46 pagineABC: Sickle-Cell Anemia, Shock, Poisoningroneln100% (1)
- Diabetic Ketoacidosis (Dka)Documento18 pagineDiabetic Ketoacidosis (Dka)dr.Bobi Ahmad Sahid, S.Kep100% (2)
- Electrolytes & FluidimbalancesDocumento80 pagineElectrolytes & FluidimbalancesDennis Nyambane MomanyiNessuna valutazione finora
- Chronic Kidney DiseaseDocumento49 pagineChronic Kidney Diseasesarguss1483% (6)
- DKA (Diabetic Ketoacidosis)Documento3 pagineDKA (Diabetic Ketoacidosis)Hassan.shehri83% (6)
- Diabetic KetoacidosisDocumento76 pagineDiabetic Ketoacidosisniyigok100% (1)
- Management of Diabetic Ketoacidosis in AdultsDocumento4 pagineManagement of Diabetic Ketoacidosis in AdultsRusida LiyaniNessuna valutazione finora
- Diabetic KetoacidosisDocumento12 pagineDiabetic Ketoacidosispolaris_027Nessuna valutazione finora
- Drug Overdose and ManagementDocumento9 pagineDrug Overdose and ManagementKoRnflakes100% (1)
- Diabetic Ketoacidosis PDFDocumento11 pagineDiabetic Ketoacidosis PDFCsr ArsNessuna valutazione finora
- CVD Case StudyDocumento9 pagineCVD Case Studyapi-346620455100% (3)
- Diabetic KetoacidosisDocumento21 pagineDiabetic KetoacidosisDrishti ShresthaNessuna valutazione finora
- DkaDocumento29 pagineDkaShadowSpectre0Nessuna valutazione finora
- Diabetis MellitusDocumento25 pagineDiabetis Mellituscdamasco18Nessuna valutazione finora
- DkaDocumento83 pagineDkaRajaKumar Ponnana100% (1)
- Type 2 Diabetes MellitusDocumento7 pagineType 2 Diabetes MellitusCadiz Etrama Di RaizelNessuna valutazione finora
- Clinical Manifestations and Treatment of HypokalemiaDocumento16 pagineClinical Manifestations and Treatment of Hypokalemiagerontogeria100% (2)
- Type 1 Diabetes: Diabetic Ketoacidos ISDocumento16 pagineType 1 Diabetes: Diabetic Ketoacidos ISapi-551073862Nessuna valutazione finora
- Heart FailureDocumento13 pagineHeart Failuremildred alidon100% (2)
- CHFDocumento61 pagineCHFAngeline Lareza-Reyna VillasorNessuna valutazione finora
- Pathophysiology of ArrhythmiasDocumento15 paginePathophysiology of ArrhythmiasJonathan MontecilloNessuna valutazione finora
- Pathophysiology of Diabetic KetoacidosisDocumento2 paginePathophysiology of Diabetic KetoacidosisGeevine CansinoNessuna valutazione finora
- Uremic EncephalopathyDocumento12 pagineUremic EncephalopathyRAechelle_Marc_4102Nessuna valutazione finora
- Cardiogenic ShockDocumento2 pagineCardiogenic ShockChristine QuironaNessuna valutazione finora
- Addison's DiseaseDocumento14 pagineAddison's Diseasedivya4nirmalaNessuna valutazione finora
- Diabetic KetoacidosisDocumento16 pagineDiabetic Ketoacidosisdrtpk100% (2)
- Pathophysiology of Diabetic KetoacidosisDocumento2 paginePathophysiology of Diabetic KetoacidosisHelcon John Dela TorreNessuna valutazione finora
- Insulin AdministrationDocumento8 pagineInsulin AdministrationskybluealiNessuna valutazione finora
- HypertensionDocumento8 pagineHypertensiongilma100% (3)
- Clinical features, evaluation, and diagnosis of diabetic ketoacidosis and hyperosmolar hyperglycemic stateDocumento17 pagineClinical features, evaluation, and diagnosis of diabetic ketoacidosis and hyperosmolar hyperglycemic statejoseaugustorojas9414Nessuna valutazione finora
- Congestive Heart FailureDocumento14 pagineCongestive Heart FailureBella Trix PagdangananNessuna valutazione finora
- Diabetes Mellitus Concept MapDocumento2 pagineDiabetes Mellitus Concept MapIzhra Margate100% (5)
- Chronic Renal FailureDocumento37 pagineChronic Renal Failuredorkiebaby100% (10)
- Lanjutan NCP DMDocumento14 pagineLanjutan NCP DMVera Andri YaniNessuna valutazione finora
- Acute Myocardial InfarctionDocumento32 pagineAcute Myocardial InfarctionListya Normalita100% (1)
- Sodium, and 350-500 Meq/L of Chloride. The Combined Effects of Serum Hyperosmolarity, Dehydration, and Acidosis Result in Increased Osmolarity in Brain Cells That ClinicallyDocumento5 pagineSodium, and 350-500 Meq/L of Chloride. The Combined Effects of Serum Hyperosmolarity, Dehydration, and Acidosis Result in Increased Osmolarity in Brain Cells That ClinicallyMorgan Mitchell100% (10)
- Community Acquired Pneumonia, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsDa EverandCommunity Acquired Pneumonia, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNessuna valutazione finora
- Gastrointestinal Bleeding, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsDa EverandGastrointestinal Bleeding, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNessuna valutazione finora
- Respiratory Alkalosis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsDa EverandRespiratory Alkalosis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNessuna valutazione finora
- A Simple Guide to Abdominal Aortic Aneurysm, Diagnosis, Treatment and Related ConditionsDa EverandA Simple Guide to Abdominal Aortic Aneurysm, Diagnosis, Treatment and Related ConditionsNessuna valutazione finora
- Disseminated Intravascular Coagulation, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsDa EverandDisseminated Intravascular Coagulation, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNessuna valutazione finora
- Exploring Perfect PostureDocumento8 pagineExploring Perfect Posturesquishyware100% (1)
- Dulce GomezDocumento7 pagineDulce Gomezapi-431029836Nessuna valutazione finora
- What Are Anxiety Disorder/depression?Documento4 pagineWhat Are Anxiety Disorder/depression?Joanna Mæ Nuñez SaysønNessuna valutazione finora
- A Y U S H: KeralamDocumento22 pagineA Y U S H: KeralamdrrejikumarNessuna valutazione finora
- An A Boli ZantesDocumento3 pagineAn A Boli Zantesvinigoncalves275Nessuna valutazione finora
- The Assurance KeyDocumento2 pagineThe Assurance KeySpeech & Language Therapy in PracticeNessuna valutazione finora
- Arie Bachtiar Dwitaryo Bagian Kardiologi Dan Kedokteran Vaskular FK. UNDIP / RS. Dr. Kariadi SemarangDocumento34 pagineArie Bachtiar Dwitaryo Bagian Kardiologi Dan Kedokteran Vaskular FK. UNDIP / RS. Dr. Kariadi SemarangSebastiana Ratih LefebvreNessuna valutazione finora
- Complementary and Alternative Medicines Among ResiDocumento10 pagineComplementary and Alternative Medicines Among ResiKaye Reyes-HapinNessuna valutazione finora
- Phenergan (Promethazine)Documento1 paginaPhenergan (Promethazine)E100% (1)
- PCAP - SummaryDocumento4 paginePCAP - SummaryNani TumlosNessuna valutazione finora
- Final Coaching CardioDocumento70 pagineFinal Coaching CardiomarykristiroseNessuna valutazione finora
- Wilderness Remote First Aid ManualDocumento128 pagineWilderness Remote First Aid Manualcr4zyvi3t100% (3)
- Nursing 215 Care Plan 2 FinalDocumento7 pagineNursing 215 Care Plan 2 Finalapi-283303129Nessuna valutazione finora
- Ched Memorandum OrderDocumento4 pagineChed Memorandum OrderEhlla Llausas AhmeeNessuna valutazione finora
- Paediatric Cleaning Toys Games and Play Equipment On The Paediatric WardDocumento8 paginePaediatric Cleaning Toys Games and Play Equipment On The Paediatric WarddidikNessuna valutazione finora
- Farmakopunktur Pada KankerDocumento15 pagineFarmakopunktur Pada KankerYoshua ViventiusNessuna valutazione finora
- 20.lymphatic DisordersDocumento16 pagine20.lymphatic DisordersShrestha Anjiv100% (2)
- Paduata Ortho ContractDocumento2 paginePaduata Ortho ContractAguila JairusNessuna valutazione finora
- Insulin Degludec PDFDocumento19 pagineInsulin Degludec PDFLilisNessuna valutazione finora
- Heti 2021 IPPE POSTER VOLTEIODocumento1 paginaHeti 2021 IPPE POSTER VOLTEIOAline SartiNessuna valutazione finora
- Terra Rosa Emagazine Issue 1Documento45 pagineTerra Rosa Emagazine Issue 1Terra RosaNessuna valutazione finora
- Administration Unit AccommodationDocumento134 pagineAdministration Unit AccommodationAdil AbdoNessuna valutazione finora
- Wa0010.Documento9 pagineWa0010.WaseemNessuna valutazione finora
- Higgins 2005Documento14 pagineHiggins 2005Maria Nuñez NevarezNessuna valutazione finora
- Ectopic PregDocumento6 pagineEctopic PregYwagar Ywagar0% (1)
- NCP Nutrition Assesment MatrixDocumento22 pagineNCP Nutrition Assesment MatrixPoschita100% (1)
- UTIDocumento4 pagineUTIVagabond RabbyNessuna valutazione finora
- RCT LectureDocumento64 pagineRCT LectureAKNTAI002Nessuna valutazione finora
- Nur 332 Ebp PosterDocumento1 paginaNur 332 Ebp Posterapi-419091662Nessuna valutazione finora
- Bobath Concept Effectiveness in Stroke RehabDocumento15 pagineBobath Concept Effectiveness in Stroke RehabAfrizal BintangNessuna valutazione finora