Potrebbero piacerti anche
- Research SyllabusDocumento2 pagineResearch SyllabusdvenumohanNessuna valutazione finora
- Google Classroom PPT For TeachersDocumento39 pagineGoogle Classroom PPT For TeachersMartin FranciscoNessuna valutazione finora
- Scope of Physiotherapy in Government and Non Government Scheme S and New Trends in Private SectorDocumento24 pagineScope of Physiotherapy in Government and Non Government Scheme S and New Trends in Private SectordvenumohanNessuna valutazione finora
- 1000 MCQs For DentistryDocumento161 pagine1000 MCQs For DentistryMuhsen Muneer89% (9)
- Scope of Research in Physiotherapy by DR - Ajay Midde of Kims HospitalDocumento33 pagineScope of Research in Physiotherapy by DR - Ajay Midde of Kims HospitaldvenumohanNessuna valutazione finora
- #KCRInsults ConstitutionDocumento4 pagine#KCRInsults ConstitutiondvenumohanNessuna valutazione finora
- Sigma Medicare Systems: Quotation / Proforma InvoiceDocumento17 pagineSigma Medicare Systems: Quotation / Proforma InvoicedvenumohanNessuna valutazione finora
- Institute of Medical Education Technology and Teachers' TrainingDocumento1 paginaInstitute of Medical Education Technology and Teachers' TrainingdvenumohanNessuna valutazione finora
- Rehabilitation Guidelines For Total Hip (Anterior) ArthroplastyDocumento4 pagineRehabilitation Guidelines For Total Hip (Anterior) ArthroplastydvenumohanNessuna valutazione finora
- Institute of Medical Education Technology and Teachers' TrainingDocumento1 paginaInstitute of Medical Education Technology and Teachers' TrainingdvenumohanNessuna valutazione finora
- ICF-Ankle Trimalleolar FractureDocumento18 pagineICF-Ankle Trimalleolar FracturedvenumohanNessuna valutazione finora
- NDS Workshop OctDocumento23 pagineNDS Workshop OctdvenumohanNessuna valutazione finora
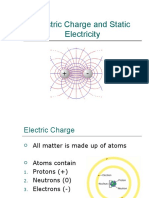
- 1 Electric Force and Electric FieldDocumento52 pagine1 Electric Force and Electric FieldKhalid mohammed khalil KhabourNessuna valutazione finora
- Course Duration: Diploma in Beauty Culture: 4 Months (288 HRS)Documento3 pagineCourse Duration: Diploma in Beauty Culture: 4 Months (288 HRS)dvenumohanNessuna valutazione finora
- Mechanical MCQDocumento2 pagineMechanical MCQKavin BalasubramaniamNessuna valutazione finora
- Diwali PowerPointDocumento30 pagineDiwali PowerPointakash baviskarNessuna valutazione finora
- Clinical Reasoning and Neurodynamic Testing and Treatment-ShacklockDocumento67 pagineClinical Reasoning and Neurodynamic Testing and Treatment-ShacklockSeda Joseph SaineNessuna valutazione finora
- Diwali: 28 October 2008 WALT Understand The Meaning of The Festival of DiwaliDocumento11 pagineDiwali: 28 October 2008 WALT Understand The Meaning of The Festival of DiwalidvenumohanNessuna valutazione finora
- Flexor Tendon Repairs Zones I III 05-13-2013Documento3 pagineFlexor Tendon Repairs Zones I III 05-13-2013Mihaela DoniciNessuna valutazione finora
- Shortwave Diathermy: Prof. Dr. Gehan MosaadDocumento29 pagineShortwave Diathermy: Prof. Dr. Gehan MosaaddvenumohanNessuna valutazione finora
- Diwali PowerPointDocumento30 pagineDiwali PowerPointakash baviskarNessuna valutazione finora
- Diwali the+Festival+of+LightsDocumento12 pagineDiwali the+Festival+of+LightsdvenumohanNessuna valutazione finora
- Mobile BrochureDocumento8 pagineMobile BrochuredvenumohanNessuna valutazione finora
- Diwali the+Festival+of+LightsDocumento12 pagineDiwali the+Festival+of+LightsdvenumohanNessuna valutazione finora
- Agency Energy Conservation ChecklistDocumento2 pagineAgency Energy Conservation ChecklistdvenumohanNessuna valutazione finora
- Scope of Research in Physiotherapy by DR - Ajay Midde of Kims HospitalDocumento33 pagineScope of Research in Physiotherapy by DR - Ajay Midde of Kims HospitaldvenumohanNessuna valutazione finora
- Test-Retest Reliability and Validity of Three Different Agility Tests For Various Team Sports in Young Male AthletesDocumento6 pagineTest-Retest Reliability and Validity of Three Different Agility Tests For Various Team Sports in Young Male AthletesdvenumohanNessuna valutazione finora
- PH D Circular For Title and Synopsis 270921Documento2 paginePH D Circular For Title and Synopsis 270921dvenumohanNessuna valutazione finora
- Reliability of Clinical Tests To Evaluate Nerve Function and Mechanosensitivity of The Upper Limb Peripheral Nervous SystemDocumento10 pagineReliability of Clinical Tests To Evaluate Nerve Function and Mechanosensitivity of The Upper Limb Peripheral Nervous SystemdvenumohanNessuna valutazione finora
- Intelect NMesDocumento28 pagineIntelect NMesJuan CamiloNessuna valutazione finora
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (399)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (73)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (120)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- Surgery 2 Case ReportDocumento12 pagineSurgery 2 Case ReportElvis NgNessuna valutazione finora
- The Courier - May 5 2017 PDFDocumento40 pagineThe Courier - May 5 2017 PDFBoki VaskeNessuna valutazione finora
- Path Questions (USMLE)Documento27 paginePath Questions (USMLE)Goljan UsmleNessuna valutazione finora
- Construing Benefits From AdversityDocumento5 pagineConstruing Benefits From AdversityIrina MorosanNessuna valutazione finora
- Care of Clients With Problems in Perception and CoordinationDocumento44 pagineCare of Clients With Problems in Perception and CoordinationmikErlhNessuna valutazione finora
- RN, MS, CCRN, Sheree Comer - Critical Care Nursing Care Plan (1998)Documento376 pagineRN, MS, CCRN, Sheree Comer - Critical Care Nursing Care Plan (1998)fega.satriaNessuna valutazione finora
- UntitledDocumento41 pagineUntitledvioletdeocaresNessuna valutazione finora
- Breast and Axilla Physical ExaminationDocumento48 pagineBreast and Axilla Physical ExaminationMelissa López Hernández0% (1)
- 2012 UpmcccanualreportDocumento70 pagine2012 Upmcccanualreportapi-290001443Nessuna valutazione finora
- NCM 106 Midterm 2013Documento6 pagineNCM 106 Midterm 2013Kirsten Sabanal100% (1)
- AstroDiagonosis CancerDocumento31 pagineAstroDiagonosis CancerOvn MurthyNessuna valutazione finora
- Breast Unit SOP: Checklist While Giving ROIS AppointmentDocumento7 pagineBreast Unit SOP: Checklist While Giving ROIS AppointmentAbhinav Ingle100% (1)
- MSDS Borax DecahydrateDocumento5 pagineMSDS Borax Decahydrateornette99Nessuna valutazione finora
- Systemic Inflammatory Response SyndromeDocumento43 pagineSystemic Inflammatory Response SyndromeherdikoshalatinNessuna valutazione finora
- Abonament Regina Maria Pachet Expert CompleteDocumento14 pagineAbonament Regina Maria Pachet Expert CompleteAna MariaNessuna valutazione finora
- Public Health NotesDocumento11 paginePublic Health NotesTRENDING YOUTUBERNessuna valutazione finora
- Light, Zimbrunes, & Gomez-Lobo, 2017Documento7 pagineLight, Zimbrunes, & Gomez-Lobo, 2017Anonymous 75M6uB3OwNessuna valutazione finora
- Chapter 1: An Overview of Clinical LaboratoryDocumento13 pagineChapter 1: An Overview of Clinical LaboratoryAshley Tañamor100% (2)
- 5d Islamic Medical EthicsDocumento33 pagine5d Islamic Medical Ethicsammaa_Nessuna valutazione finora
- Laura Final FinalDocumento68 pagineLaura Final Finalngalame lauraNessuna valutazione finora
- Sterile Parenteral Products: A Narrative Approach: Journal of Drug Delivery and TherapeuticsDocumento8 pagineSterile Parenteral Products: A Narrative Approach: Journal of Drug Delivery and TherapeuticsArinta Purwi SuhartiNessuna valutazione finora
- Basic ImmunologyDocumento2 pagineBasic ImmunologyadibwanNessuna valutazione finora
- FilgrastimDocumento3 pagineFilgrastimfransiscaNessuna valutazione finora
- An Introduction To Cytogenetics DR - DanaDocumento54 pagineAn Introduction To Cytogenetics DR - Danaalibayaty1Nessuna valutazione finora
- E Coli Path RHPDocumento18 pagineE Coli Path RHPOscar de la CruzNessuna valutazione finora
- 1700 Subjectwise 2017 p197 232Documento36 pagine1700 Subjectwise 2017 p197 232Pravin MaratheNessuna valutazione finora
- Gordana Pavliša, Marina Labor, Hrvoje Puretić, Ana Hećimović, Marko Jakopović, Miroslav SamaržijaDocumento12 pagineGordana Pavliša, Marina Labor, Hrvoje Puretić, Ana Hećimović, Marko Jakopović, Miroslav SamaržijaAngelo GarinoNessuna valutazione finora
- 2022 Danny Carroll Terminal Cancer Is A Misdiagnosis, Discover ADocumento79 pagine2022 Danny Carroll Terminal Cancer Is A Misdiagnosis, Discover Asevigonza59Nessuna valutazione finora
- Breast Reconstruction With SGAP and IGAP FlapsDocumento9 pagineBreast Reconstruction With SGAP and IGAP FlapsJean-Philippe BinderNessuna valutazione finora
- Immunology Final QS-Part1Documento15 pagineImmunology Final QS-Part1Abdallah Essam Al-Zireeni50% (2)