Potrebbero piacerti anche
- Dengue Fever 4Documento65 pagineDengue Fever 4Roshandiep GillNessuna valutazione finora
- T Cell Immunopathogenesis of Dengue Virus Infection: Lokesh Guglani and S.K. KabraDocumento12 pagineT Cell Immunopathogenesis of Dengue Virus Infection: Lokesh Guglani and S.K. KabraayushintamahaputriNessuna valutazione finora
- 17a. MIKRO Virus PenyebabDocumento153 pagine17a. MIKRO Virus PenyebabRahmawati HamudiNessuna valutazione finora
- Dengue FeverDocumento15 pagineDengue FeverNitesh GargNessuna valutazione finora
- Yang LengkapDocumento9 pagineYang LengkapauliyasaumaNessuna valutazione finora
- 8 Dengue in ChildrenDocumento61 pagine8 Dengue in Childrenastri anindyaNessuna valutazione finora
- Opportunistic Viral InfectionsDocumento40 pagineOpportunistic Viral InfectionsjohndemoNessuna valutazione finora
- Tarea de Gimena, Me Debe 10 FavoresDocumento3 pagineTarea de Gimena, Me Debe 10 FavoresGabriel FernándezNessuna valutazione finora
- 1 PDFDocumento22 pagine1 PDFnursidiq10Nessuna valutazione finora
- Presentation On DengueDocumento39 paginePresentation On DenguearmanNessuna valutazione finora
- DengueDocumento30 pagineDengueSaurav AroraNessuna valutazione finora
- Maabara Ya Kisasa: (Compiled by Prof. Eftyxia Vardas - March 2014)Documento2 pagineMaabara Ya Kisasa: (Compiled by Prof. Eftyxia Vardas - March 2014)Haki NgowiNessuna valutazione finora
- Tropical Infection DiseasesDocumento60 pagineTropical Infection DiseasesVerarisna100% (1)
- Dengue Hemorrhagic Fever With Special Emphasis On ImmunopathogenesisDocumento12 pagineDengue Hemorrhagic Fever With Special Emphasis On ImmunopathogenesisHadley AuliaNessuna valutazione finora
- Dengue-Malaria TOT For Doctors 2022 Dengue Diagnosis-Dr - A .NandyDocumento32 pagineDengue-Malaria TOT For Doctors 2022 Dengue Diagnosis-Dr - A .NandyAkshat SharmaNessuna valutazione finora
- The Association of Obesity and Severe Dengue - Possible PathophysiologicaDocumento14 pagineThe Association of Obesity and Severe Dengue - Possible PathophysiologicaTaufiqurrokhman RofiiNessuna valutazione finora
- Human Immunodeficiency Virus (HIV) and Opperortunistic InfectionDocumento54 pagineHuman Immunodeficiency Virus (HIV) and Opperortunistic InfectionBikash SahNessuna valutazione finora
- DENGUE CASE MANAGEMENT DiscussionDocumento5 pagineDENGUE CASE MANAGEMENT DiscussionHanako AranillaNessuna valutazione finora
- HHS Public Access: Plasma Leakage in Dengue Hemorrhagic FeverDocumento17 pagineHHS Public Access: Plasma Leakage in Dengue Hemorrhagic FeverZach AKNessuna valutazione finora
- DHF - Dengue Hemorrhagic FeverDocumento3 pagineDHF - Dengue Hemorrhagic FeverJellyAnnAujeroSanchezNessuna valutazione finora
- Cells in Dengue Virus InfectionDocumento16 pagineCells in Dengue Virus Infectionthyago6Nessuna valutazione finora
- Gulu Cohes Hiv Nelly MDDocumento68 pagineGulu Cohes Hiv Nelly MDYIKI ISAACNessuna valutazione finora
- Jurnal 4Documento16 pagineJurnal 4Salsa DikaNessuna valutazione finora
- Immune-Mediated Cytokine Storm and Its Role in Severe DengueDocumento12 pagineImmune-Mediated Cytokine Storm and Its Role in Severe DengueAkila SwaminathanNessuna valutazione finora
- Dengue MedscapeDocumento58 pagineDengue MedscapearuhulaminiNessuna valutazione finora
- Review Article: Pathogenesis of Dengue Haemorrhagic Fever and Its Impact On Case ManagementDocumento7 pagineReview Article: Pathogenesis of Dengue Haemorrhagic Fever and Its Impact On Case ManagementRani ChesarNessuna valutazione finora
- Pathogenesis of Vascular Leak in Dengue Virus Infection: ImmunologyDocumento9 paginePathogenesis of Vascular Leak in Dengue Virus Infection: Immunologyeuphoria8346Nessuna valutazione finora
- Part IIDocumento32 paginePart IITofikNessuna valutazione finora
- Pathogenesis of VirusesDocumento33 paginePathogenesis of VirusesFrancis ChegeNessuna valutazione finora
- Dengue Fever: By:Mehreen (09-100)Documento20 pagineDengue Fever: By:Mehreen (09-100)Arsalan NadeemNessuna valutazione finora
- Disorder of The Immune System 2Documento58 pagineDisorder of The Immune System 2Daniel OkakaNessuna valutazione finora
- Herpes VirusesDocumento26 pagineHerpes VirusesUmar'Farouq OniNessuna valutazione finora
- Disease Process HIVDocumento4 pagineDisease Process HIValeksdj1987Nessuna valutazione finora
- Il 6 New FullDocumento13 pagineIl 6 New FullAnindhiani Aparamitha SariNessuna valutazione finora
- Case ReportDocumento29 pagineCase ReportFinda RedhizaNessuna valutazione finora
- Human Immunodeficency VirusDocumento58 pagineHuman Immunodeficency VirusRandy BerryNessuna valutazione finora
- Hubungan Trombositopenia Dan Hematokrit Dengan Manifestasi Perdarahan Pada Penderita Demam Dengue Dan Demam Berdarah DengueDocumento8 pagineHubungan Trombositopenia Dan Hematokrit Dengan Manifestasi Perdarahan Pada Penderita Demam Dengue Dan Demam Berdarah DengueDea RitungNessuna valutazione finora
- Hiv/Aids and Principles of HaartDocumento88 pagineHiv/Aids and Principles of Haarthabtamu alemayehuNessuna valutazione finora
- Pathogenesis of Hemorrhagic Due To Dengue Virus: Literature ReviewDocumento5 paginePathogenesis of Hemorrhagic Due To Dengue Virus: Literature Reviewfebyan yohanesNessuna valutazione finora
- DHF With AppDocumento6 pagineDHF With AppputiridhaNessuna valutazione finora
- Dengue-Malaria TOT For Doctors 2022 District Dengue PPTDocumento88 pagineDengue-Malaria TOT For Doctors 2022 District Dengue PPTRanjeet SinghNessuna valutazione finora
- Denguefinalpdf-170803082145 2Documento74 pagineDenguefinalpdf-170803082145 2L. HusnaNessuna valutazione finora
- Sepsis and Diabetes MellitusDocumento20 pagineSepsis and Diabetes MellitusOlga GoryachevaNessuna valutazione finora
- MF3 - Herpes Simplex VirusDocumento31 pagineMF3 - Herpes Simplex VirusAnnbe BarteNessuna valutazione finora
- Dengue FeverDocumento31 pagineDengue FeverAditya Agarwal100% (1)
- Dengue Fever 2Documento5 pagineDengue Fever 2Gayitiri MenonNessuna valutazione finora
- Tuberculosis & Leprosy: Alkan Health Science Business and Technology CollegeDocumento59 pagineTuberculosis & Leprosy: Alkan Health Science Business and Technology CollegejibrailNessuna valutazione finora
- HIV Over Veiw - PPTMDocumento57 pagineHIV Over Veiw - PPTMMutegeki AdolfNessuna valutazione finora
- Epstein-Barr Virus (Infectious Mononucleosis)Documento36 pagineEpstein-Barr Virus (Infectious Mononucleosis)GîrbovanCristinaNessuna valutazione finora
- Vitamins and DengueDocumento13 pagineVitamins and DengueShuvo DasNessuna valutazione finora
- STI Slides EditedDocumento43 pagineSTI Slides Editedokureblessing33Nessuna valutazione finora
- Dengue TOT Virology, Pathogenesis Lab Diag. 2023Documento44 pagineDengue TOT Virology, Pathogenesis Lab Diag. 2023ATHIBAN VNessuna valutazione finora
- Platelets in Dengue Infection: Drug Discovery Today June 2011Documento7 paginePlatelets in Dengue Infection: Drug Discovery Today June 2011Dwi WijayantiNessuna valutazione finora
- DengueDocumento44 pagineDengueAl JihadNessuna valutazione finora
- Human Immunodeficiency VirusDocumento24 pagineHuman Immunodeficiency VirusMalueth AnguiNessuna valutazione finora
- Adenovirus Infection in Immunocompromised PatientsDocumento16 pagineAdenovirus Infection in Immunocompromised PatientsMuskan MuhemmedNessuna valutazione finora
- Menigitis EncephalitisDocumento63 pagineMenigitis EncephalitisHussain AzharNessuna valutazione finora
- HerpesvirusesDocumento25 pagineHerpesvirusesHoor Ul Ain RounaqNessuna valutazione finora
- Introduction to Respiratory Syncytial Virus InfectionDa EverandIntroduction to Respiratory Syncytial Virus InfectionNessuna valutazione finora
- Multi Organ Dysfunction SyndromeDocumento40 pagineMulti Organ Dysfunction SyndromeDr. Jayesh PatidarNessuna valutazione finora
- Cefdinir Double Dose - PIDJDocumento8 pagineCefdinir Double Dose - PIDJAhmad TharwatNessuna valutazione finora
- Elecsys Hbsag Ii: A) Tris (2,2'-Bipyridyl) Ruthenium (Ii) - Complex (Ru (Bpy) )Documento5 pagineElecsys Hbsag Ii: A) Tris (2,2'-Bipyridyl) Ruthenium (Ii) - Complex (Ru (Bpy) )Brian SamanyaNessuna valutazione finora
- RTI Online - Online RTI Information System - Vikas PatniDocumento1 paginaRTI Online - Online RTI Information System - Vikas PatniTmpNessuna valutazione finora
- Isolation 2007Documento219 pagineIsolation 2007Jorge CunhaNessuna valutazione finora
- Aso Latex Spin ReactDocumento1 paginaAso Latex Spin ReactLuis Ferdinand Dacera-Gabronino Gamponia-NonanNessuna valutazione finora
- What Is Viral Pneumonia?: 8th Leading Cause of Death Children and People Over 65Documento10 pagineWhat Is Viral Pneumonia?: 8th Leading Cause of Death Children and People Over 65Andeariesa DarmansiusNessuna valutazione finora
- Shweta PPT ThesisDocumento10 pagineShweta PPT ThesisAKSHAY WAKTENessuna valutazione finora
- PsoriasisDocumento57 paginePsoriasisapi-19916399100% (1)
- 2 MM10 CellulitisDocumento3 pagine2 MM10 CellulitisSelva VelanNessuna valutazione finora
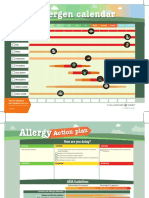
- Allergen Calendar - EnglishDocumento2 pagineAllergen Calendar - Englishpkgill15Nessuna valutazione finora
- Pathology SGD 4: Diseases-Of-The-Immune-System: Group-4Documento23 paginePathology SGD 4: Diseases-Of-The-Immune-System: Group-4Kalpana JenaNessuna valutazione finora
- Specific Host Defenses: The Immune ResponseDocumento52 pagineSpecific Host Defenses: The Immune ResponseRicardo M GomezNessuna valutazione finora
- Monocyte - WikipediaDocumento14 pagineMonocyte - WikipediaMM NabeelNessuna valutazione finora
- Blood & Tissue Protozoa-II: Prof - Dr.Shaheen Sharafat MBBS.M.Phil PH.D Dept - of Pathology LNH&MCDocumento47 pagineBlood & Tissue Protozoa-II: Prof - Dr.Shaheen Sharafat MBBS.M.Phil PH.D Dept - of Pathology LNH&MCHumna JawedNessuna valutazione finora
- Nursing Care Plan of The NewbornDocumento4 pagineNursing Care Plan of The Newbornbowki namoNessuna valutazione finora
- Novilyn C. Pataray BSN - Ii Pharyngitis: St. Paul College of Ilocos SurDocumento1 paginaNovilyn C. Pataray BSN - Ii Pharyngitis: St. Paul College of Ilocos SurCharina AubreyNessuna valutazione finora
- This Chapters 1 5Documento29 pagineThis Chapters 1 5Joanna Marie EstanislaoNessuna valutazione finora
- IntraabDocumento41 pagineIntraabDonzzkie DonNessuna valutazione finora
- Kuby5 13 ComplementDocumento20 pagineKuby5 13 ComplementASDASDDD2Nessuna valutazione finora
- History of COVID-19Documento2 pagineHistory of COVID-19Sahara SoboNessuna valutazione finora
- Necrotizing Fasciitis: David Hough MSIII Penn State College of MedicineDocumento33 pagineNecrotizing Fasciitis: David Hough MSIII Penn State College of Medicineaaz220Nessuna valutazione finora
- Type II Hypersensitivity Reaction - Abstract - Europe PMCDocumento7 pagineType II Hypersensitivity Reaction - Abstract - Europe PMCHashem Essa QatawnehNessuna valutazione finora
- Infectious Diseases: A Case of Tuberculosis Verrucosa Cutis in Brazil Undiagnosed For 15 YearsDocumento3 pagineInfectious Diseases: A Case of Tuberculosis Verrucosa Cutis in Brazil Undiagnosed For 15 YearsAnthony SetiawanNessuna valutazione finora
- Super Simplified Pathology Hematology - Dr. Priyanka SachdevDocumento500 pagineSuper Simplified Pathology Hematology - Dr. Priyanka SachdevMohd SaquibNessuna valutazione finora
- Diphtheria Guidelines FinalDocumento47 pagineDiphtheria Guidelines Finalmuhammad_ariefNessuna valutazione finora
- Cytokine Storm Response To COVID-19 VaccinationsDocumento3 pagineCytokine Storm Response To COVID-19 VaccinationsewewewNessuna valutazione finora
- Polio: Disease What It Does Why ImmunizeDocumento2 paginePolio: Disease What It Does Why ImmunizeVictor PrettiNessuna valutazione finora
- Drug Study BAIAEDocumento5 pagineDrug Study BAIAEDAOman09Nessuna valutazione finora
- Rottier & Ince, 2003Documento292 pagineRottier & Ince, 2003Yamid BarreraNessuna valutazione finora