Potrebbero piacerti anche
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5795)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (74)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- Cayenne 5Documento17 pagineCayenne 5Marcelo AndradeNessuna valutazione finora
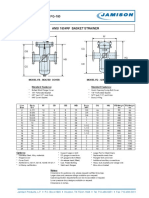
- FB-150 FQ-150 Basket StrainerDocumento1 paginaFB-150 FQ-150 Basket Strainerklich77Nessuna valutazione finora
- Modul 2 Operasi GeneratorDocumento50 pagineModul 2 Operasi Generatorika yuliyani murtiharjonoNessuna valutazione finora
- National Telecommunication Corporation (NTC)Documento40 pagineNational Telecommunication Corporation (NTC)Faheem Sajid100% (1)
- The Effect of Axial Flow Velocity On Annular Gap Windage Power LossDocumento12 pagineThe Effect of Axial Flow Velocity On Annular Gap Windage Power Losskien nguyenNessuna valutazione finora
- Astm A106-2002Documento13 pagineAstm A106-2002henryNessuna valutazione finora
- 3 Statement Model: Strictly ConfidentialDocumento13 pagine3 Statement Model: Strictly ConfidentialLalit mohan PradhanNessuna valutazione finora
- HyperMILL Readme enDocumento20 pagineHyperMILL Readme enjimNessuna valutazione finora
- Review For Final ExamDocumento29 pagineReview For Final ExamhaddanNessuna valutazione finora
- Python For Data ScienceDocumento22 paginePython For Data ScienceMohit MalghadeNessuna valutazione finora
- Lab 3 Pre LabDocumento3 pagineLab 3 Pre LabMina VoNessuna valutazione finora
- Understanding The Use of Ofdm in Ieee 802.16 (Wimax) : Roberto SacchiDocumento8 pagineUnderstanding The Use of Ofdm in Ieee 802.16 (Wimax) : Roberto SacchiHarald KerresNessuna valutazione finora
- Bluetooth PresentationDocumento18 pagineBluetooth Presentationarjun_rathore8178Nessuna valutazione finora
- Shared Memory ArchitectureDocumento2 pagineShared Memory ArchitectureNeethu RajeshNessuna valutazione finora
- Rails BasicsDocumento229 pagineRails BasicsachhuNessuna valutazione finora
- Inserting Images - ShareLaTeX, Online LaTeX EditorDocumento11 pagineInserting Images - ShareLaTeX, Online LaTeX EditorAviraj3892Nessuna valutazione finora
- Universal Law of GravitationDocumento17 pagineUniversal Law of GravitationScionNessuna valutazione finora
- (John F. Moulder) PHI Handbook of XRay Photoelectron SpectrosDocumento192 pagine(John F. Moulder) PHI Handbook of XRay Photoelectron SpectrosCamilo CorredorNessuna valutazione finora
- Compre Queation PaperDocumento6 pagineCompre Queation PaperGanesh DharmireddyNessuna valutazione finora
- MCAT Uhs Past Paper (2008-2016)Documento180 pagineMCAT Uhs Past Paper (2008-2016)Abdullah SheikhNessuna valutazione finora
- Ar 4201 PDFDocumento22 pagineAr 4201 PDFRiyanPratomuSiregarNessuna valutazione finora
- The Whys and Wherefores of Microphone Array Crosstalk in Multichannel Microphone Array DesignDocumento6 pagineThe Whys and Wherefores of Microphone Array Crosstalk in Multichannel Microphone Array DesignmewarulesNessuna valutazione finora
- Valve & Amplifier Design, Valve EquivalentsDocumento51 pagineValve & Amplifier Design, Valve EquivalentsValve Data80% (5)
- The C Puzzle BookDocumento93 pagineThe C Puzzle Bookabhijeetnayak67% (3)
- P103154 - 7.00 - Doc - Manual - 8000 WindlassDocumento43 pagineP103154 - 7.00 - Doc - Manual - 8000 WindlassDanNessuna valutazione finora
- TB-2100 Operational and Maintenance Manual Rev C OptimiseDocumento224 pagineTB-2100 Operational and Maintenance Manual Rev C OptimisearnaudmarielNessuna valutazione finora
- Manual Prevention An Control of Lost Cir PDFDocumento222 pagineManual Prevention An Control of Lost Cir PDFAna Maria TovarNessuna valutazione finora
- Packet Life BookDocumento28 paginePacket Life BookboucheravNessuna valutazione finora
- Seborg Chapter 1Documento3 pagineSeborg Chapter 1maykesguerraNessuna valutazione finora
- Rsa Netwitness Logs and Packets: Server, Dac and San HW SpecificationsDocumento10 pagineRsa Netwitness Logs and Packets: Server, Dac and San HW SpecificationsfunyiroemberNessuna valutazione finora