Potrebbero piacerti anche
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5795)
- Bronkografi BronkiektasisDocumento6 pagineBronkografi BronkiektasisAlvin Dzaky NurhadyNessuna valutazione finora
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- RS BireuenDocumento120 pagineRS BireuenAlvin Dzaky NurhadyNessuna valutazione finora
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
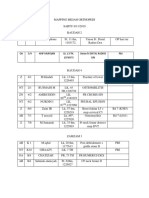
- Mapping Ortho Minggu 10Documento6 pagineMapping Ortho Minggu 10Alvin Dzaky NurhadyNessuna valutazione finora
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- Absen MR Koyan DLLDocumento2 pagineAbsen MR Koyan DLLAlvin Dzaky NurhadyNessuna valutazione finora
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- Opportunistic MycosesDocumento7 pagineOpportunistic MycosesDee GeeNessuna valutazione finora
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- Infectious Disease (Viruses)Documento4 pagineInfectious Disease (Viruses)Ahmed GaberNessuna valutazione finora
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- An Anatomical and Pathological Examination of The First Recorded Stranding of A Fraser's DolphinDocumento7 pagineAn Anatomical and Pathological Examination of The First Recorded Stranding of A Fraser's DolphinStephanie Aeriel OcampoNessuna valutazione finora
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- Corneal UlcerDocumento29 pagineCorneal UlcerdrrahulvNessuna valutazione finora
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (74)
- Study TableDocumento10 pagineStudy TableBashaer GellehNessuna valutazione finora
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (345)
- Venesection: Phlebotomy orDocumento21 pagineVenesection: Phlebotomy orLesly Marie LaxamanaNessuna valutazione finora
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Cefuroxime (Drug Study)Documento2 pagineCefuroxime (Drug Study)Rosebel LaguraNessuna valutazione finora
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Reading Karyotypes WorksheetDocumento2 pagineReading Karyotypes WorksheetSamNessuna valutazione finora
- Medicinal Study of Zingiberaceae PlantsDocumento65 pagineMedicinal Study of Zingiberaceae PlantsPravin NagoreNessuna valutazione finora
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- An Invisible World: College PhysicsDocumento39 pagineAn Invisible World: College PhysicsAngela DardonisNessuna valutazione finora
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- Tapasya Full Test-21 - BPC On 24-05-2020Documento23 pagineTapasya Full Test-21 - BPC On 24-05-2020Jagadesh nvNessuna valutazione finora
- PursueDocumento3 paginePursueBalram JiNessuna valutazione finora
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- Eye Culture 1. Principle: 3.6.11 SOP: Eye Cultures Page 1 of 2Documento2 pagineEye Culture 1. Principle: 3.6.11 SOP: Eye Cultures Page 1 of 2SemeeeJuniorNessuna valutazione finora
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1091)
- Allergic Rhinitis and RhinosinusitisDocumento53 pagineAllergic Rhinitis and RhinosinusitisSinta FiraniNessuna valutazione finora
- Grand Rounds: Roxanne Jeen L. Fornolles, M.DDocumento61 pagineGrand Rounds: Roxanne Jeen L. Fornolles, M.DRj FornollesNessuna valutazione finora
- The Secret of Kimchi's Unique TasteDocumento5 pagineThe Secret of Kimchi's Unique Tastetessar f gNessuna valutazione finora
- About Childhood Leukemia: Overview and TypesDocumento11 pagineAbout Childhood Leukemia: Overview and TypessetiawatifsNessuna valutazione finora
- Ministry Speeds Approval Process For Avigan To Treat COVID-19 - The Asahi ShimbunDocumento2 pagineMinistry Speeds Approval Process For Avigan To Treat COVID-19 - The Asahi ShimbunMustafa ShwayatNessuna valutazione finora
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- KlotoDocumento24 pagineKlotoyulian.stanevNessuna valutazione finora
- Worksheet 2 - Hematology - 2020 (11th Ed)Documento3 pagineWorksheet 2 - Hematology - 2020 (11th Ed)ahmadmahdi18mNessuna valutazione finora
- RNA VirusesDocumento56 pagineRNA VirusesJaveriaZafarNessuna valutazione finora
- Prokaryotic Gene RegulationDocumento3 pagineProkaryotic Gene RegulationRona Nur AfifahNessuna valutazione finora
- Non Blanching RashDocumento9 pagineNon Blanching RashAfnita LestaryNessuna valutazione finora
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- Importanceof CarbohydratesDocumento3 pagineImportanceof CarbohydratescraigNessuna valutazione finora
- BacteriaDocumento22 pagineBacteriajenelynNessuna valutazione finora
- PDFDocumento97 paginePDFUmeshNessuna valutazione finora
- Unit 2, Genetic Proceses, Unit Test - 2Documento5 pagineUnit 2, Genetic Proceses, Unit Test - 2hewleet100% (1)
- Antineoplastics AgentsDocumento19 pagineAntineoplastics AgentsPrincess Diannejane MurlaNessuna valutazione finora
- Medical Parasit Ology: by Anas Mahadi ElnazeerDocumento28 pagineMedical Parasit Ology: by Anas Mahadi Elnazeerardesh abdilleNessuna valutazione finora
- Anti-Infective Therapy "Antibiotics": Definitions Chemotherapeutic Agent Anti-Microbial AgentDocumento8 pagineAnti-Infective Therapy "Antibiotics": Definitions Chemotherapeutic Agent Anti-Microbial AgentMohamed EbrahimNessuna valutazione finora
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)