Potrebbero piacerti anche
- Formulation of NCPDocumento8 pagineFormulation of NCPSandeep choudharyNessuna valutazione finora
- Information, Education Communication Aparna AjayDocumento70 pagineInformation, Education Communication Aparna AjayAparna Aby100% (1)
- IUCD Manual EnglishDocumento194 pagineIUCD Manual EnglishHarshaWakodkarNessuna valutazione finora
- Family Folder: 1. Identification InformationDocumento7 pagineFamily Folder: 1. Identification InformationLavie GangwarNessuna valutazione finora
- PDF Theories Applied To Midwifery CompressDocumento10 paginePDF Theories Applied To Midwifery CompressRafiqa BashirNessuna valutazione finora
- A Study To Assess The Effectiveness of VAT On Knowledge Regarding Janani Suraksha Yojana Among Mothers of Selected Rural Area at Bangalore, Karnataka, IndiaDocumento3 pagineA Study To Assess The Effectiveness of VAT On Knowledge Regarding Janani Suraksha Yojana Among Mothers of Selected Rural Area at Bangalore, Karnataka, IndiaAnonymous izrFWiQNessuna valutazione finora
- FWPDocumento37 pagineFWPhemaanandhyNessuna valutazione finora
- Health Insurance SchemeDocumento10 pagineHealth Insurance SchemeKailash NagarNessuna valutazione finora
- Likert Scale KMCDocumento1 paginaLikert Scale KMCedrinsneNessuna valutazione finora
- Antenatal CareDocumento4 pagineAntenatal Caredrfaruqui2551100% (1)
- Integrated Child Development Scheme (ICDS)Documento30 pagineIntegrated Child Development Scheme (ICDS)Geeta KumariNessuna valutazione finora
- External ExaminationDocumento16 pagineExternal Examinationrejoice international100% (1)
- The 21 Nursing Problems: Faye Glenn AbdellahDocumento44 pagineThe 21 Nursing Problems: Faye Glenn AbdellahShafiq Ur RahmanNessuna valutazione finora
- Management of Infertility: Presented By: Dr. Sheetal M Savaliya Guide: Dr. Anil P Singh Co-Guide: Dr. Shailesh MundhavaDocumento37 pagineManagement of Infertility: Presented By: Dr. Sheetal M Savaliya Guide: Dr. Anil P Singh Co-Guide: Dr. Shailesh MundhavaBhawna JoshiNessuna valutazione finora
- SYMPOSIUM On Recruitment & Disciplineof Nursing InstitutionDocumento22 pagineSYMPOSIUM On Recruitment & Disciplineof Nursing InstitutionBabita DhruwNessuna valutazione finora
- JalajaDocumento3 pagineJalajaSunija SelvamNessuna valutazione finora
- Genetic CounsellingDocumento12 pagineGenetic CounsellingPATEL NEHAKUMARI VIMALBHAINessuna valutazione finora
- NSTDocumento5 pagineNSTMarlisa YanuartiNessuna valutazione finora
- 1 WichamDocumento34 pagine1 WichamBhawna JoshiNessuna valutazione finora
- M.Sc. Nursing Syllabus and RegulationDocumento145 pagineM.Sc. Nursing Syllabus and RegulationSanthosh.S.UNessuna valutazione finora
- Current Trends Issues in Nursing Education Nursing Education ppt2 161216024141 PDFDocumento41 pagineCurrent Trends Issues in Nursing Education Nursing Education ppt2 161216024141 PDFNise Mon KuriakoseNessuna valutazione finora
- BudgetDocumento12 pagineBudgetDr. Jayesh PatidarNessuna valutazione finora
- A Study To Assess The Knowledge and Attitude of Postnatal Mother Regarding Postnatal Diet in A View of Developing Booklet at Selected Community AreaDocumento14 pagineA Study To Assess The Knowledge and Attitude of Postnatal Mother Regarding Postnatal Diet in A View of Developing Booklet at Selected Community AreaIJAR JOURNALNessuna valutazione finora
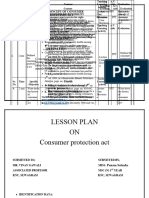
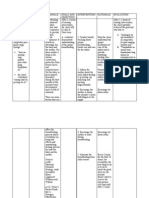
- LESSON PLAN ON Consumer Protection ActDocumento4 pagineLESSON PLAN ON Consumer Protection ActAnkush Kulat PatilNessuna valutazione finora
- Job Description of Nursing OfficerDocumento12 pagineJob Description of Nursing OfficerPunam DuwalNessuna valutazione finora
- WHO Guidelines On Acute Malnutrition, 2023Documento188 pagineWHO Guidelines On Acute Malnutrition, 2023Arafat HassanNessuna valutazione finora
- Shimla Nursing College Annadale Bai BerbaiDocumento17 pagineShimla Nursing College Annadale Bai Berbaigill priyaNessuna valutazione finora
- Health Care Deliver System AjayDocumento41 pagineHealth Care Deliver System AjayAjay DNessuna valutazione finora
- Icm Competencies en ScreensDocumento22 pagineIcm Competencies en ScreensSuci Rahmadheny100% (1)
- Nutritional Rehabilitation: Presented By: Dr. Kunal Guided By: Dr. Abhay MudeyDocumento43 pagineNutritional Rehabilitation: Presented By: Dr. Kunal Guided By: Dr. Abhay MudeyNazia Arif100% (1)
- Major Stake Holders in Health Care System-GovernmentDocumento22 pagineMajor Stake Holders in Health Care System-GovernmentTanviNessuna valutazione finora
- Lecture Notes (Genetic Counselling)Documento25 pagineLecture Notes (Genetic Counselling)Zearo GamingNessuna valutazione finora
- Fertilization & ImplantationDocumento54 pagineFertilization & ImplantationMarvelousNessuna valutazione finora
- Diagnosis of PregnancyDocumento16 pagineDiagnosis of PregnancySùjâl PätídàrNessuna valutazione finora
- List of Statistical PackagesDocumento2 pagineList of Statistical Packagestavishi dhawanNessuna valutazione finora
- Growth - Development of Fetus - NeonateDocumento40 pagineGrowth - Development of Fetus - NeonatesujidahNessuna valutazione finora
- Sba Trainers Guide For Anm LHV SNDocumento128 pagineSba Trainers Guide For Anm LHV SNnmsusarla999100% (1)
- Current Trends and Issue in NSG ManagementDocumento9 pagineCurrent Trends and Issue in NSG ManagementSimran JosanNessuna valutazione finora
- National Aids Control Programme Phase-Iv Current Status and Critical AppraisalDocumento71 pagineNational Aids Control Programme Phase-Iv Current Status and Critical AppraisalNeethu Vincent100% (1)
- National Aids Control ProgDocumento45 pagineNational Aids Control ProgGirishkumar KrishnaNessuna valutazione finora
- Effectiveness of Planned Teaching Programme On Knowledge Regarding Identification of Danger Signs in Neonates Among Post-Natal MothersDocumento4 pagineEffectiveness of Planned Teaching Programme On Knowledge Regarding Identification of Danger Signs in Neonates Among Post-Natal MothersInternational Journal of Innovative Science and Research TechnologyNessuna valutazione finora
- Twenty Point Programme by Varnit VashisthaDocumento9 pagineTwenty Point Programme by Varnit VashisthaVarnit VashishtaNessuna valutazione finora
- Evidence Based PracticeDocumento5 pagineEvidence Based PracticeDhanesh Verma100% (1)
- Congenital Syphilis SeminarDocumento32 pagineCongenital Syphilis SeminarRavi KumawatNessuna valutazione finora
- Bonding NewDocumento23 pagineBonding NewPadmaNessuna valutazione finora
- Levine Theory of NursingDocumento78 pagineLevine Theory of NursingShivangi SharmaNessuna valutazione finora
- 2017 STP Paed Neonates PDFDocumento258 pagine2017 STP Paed Neonates PDFChoden JamyangNessuna valutazione finora
- L.P of CHCDocumento18 pagineL.P of CHCKiranNessuna valutazione finora
- Tele Med and Tele NursingDocumento14 pagineTele Med and Tele NursingVineeta Jose100% (1)
- Pooja Seminar FinalDocumento13 paginePooja Seminar FinalHemantNessuna valutazione finora
- Preventive ObstetricsDocumento57 paginePreventive ObstetricsGunaNessuna valutazione finora
- Professional AdvancementDocumento51 pagineProfessional AdvancementReshma AnilkumarNessuna valutazione finora
- Performance Checklist Hand WashingDocumento4 paginePerformance Checklist Hand WashingPatrick Nava100% (1)
- AccreditationDocumento12 pagineAccreditationkiranNessuna valutazione finora
- Ministry of Health and Family Welfare Pregnancy GuidelinesDocumento173 pagineMinistry of Health and Family Welfare Pregnancy GuidelinesKhushi GuptaNessuna valutazione finora
- Healthy Newborn InfantDocumento20 pagineHealthy Newborn InfantRAMAVATH SRINUNessuna valutazione finora
- Health Promotion & PHCDocumento39 pagineHealth Promotion & PHChiral mistry100% (1)
- PDF DocumentDocumento36 paginePDF DocumentSuji MerlineNessuna valutazione finora
- Annotated BibliographyDocumento6 pagineAnnotated Bibliographyapi-268670617Nessuna valutazione finora
- The Ethic of Care: A Moral Compass for Canadian Nursing Practice - Revised EditionDa EverandThe Ethic of Care: A Moral Compass for Canadian Nursing Practice - Revised EditionNessuna valutazione finora
- 3011-Article Text-11322-2-10-20221109Documento12 pagine3011-Article Text-11322-2-10-20221109HidayahNessuna valutazione finora
- Breastfeeding Coding: For Obstetrician-Gynecologists 2016Documento1 paginaBreastfeeding Coding: For Obstetrician-Gynecologists 2016Dyah Ajeng PratiwiNessuna valutazione finora
- Ineffective Breast FeedingDocumento5 pagineIneffective Breast Feedingcamilleandaj070575% (12)
- Breast Feeding Week CelebrationDocumento24 pagineBreast Feeding Week CelebrationANSHU PANDEYNessuna valutazione finora
- Difficulties in Breastfeeding Easy Solution by OkeDocumento6 pagineDifficulties in Breastfeeding Easy Solution by OkewladjaNessuna valutazione finora
- Screenshot 2022-05-03 at 20.47.09Documento1 paginaScreenshot 2022-05-03 at 20.47.09millu 2340Nessuna valutazione finora
- Course Task #9 Pedia LecDocumento2 pagineCourse Task #9 Pedia LecMushy_ayaNessuna valutazione finora
- 1 s2.0 S0213911121001989 MainDocumento3 pagine1 s2.0 S0213911121001989 MainVinna LestaryNessuna valutazione finora
- Pijat Oksi DG Aromaterapi Kulit JerukDocumento9 paginePijat Oksi DG Aromaterapi Kulit JerukBAnfalia Dina ClaudiaNessuna valutazione finora
- Price List Spectra JUNI 2020 Update 03 Mar 2021Documento2 paginePrice List Spectra JUNI 2020 Update 03 Mar 2021Muhammad Irfan ArdiansyahNessuna valutazione finora
- FDARDocumento1 paginaFDARJohn Lloyd MontecilloNessuna valutazione finora
- The Anatomy of A Lactating BreastDocumento16 pagineThe Anatomy of A Lactating BreastJSeasharkNessuna valutazione finora
- Essential Intrapartum and Newborn CareDocumento2 pagineEssential Intrapartum and Newborn CareKharene LirazanNessuna valutazione finora
- Iloilo City Regulation Ordinance 2010-234Documento4 pagineIloilo City Regulation Ordinance 2010-234Iloilo City CouncilNessuna valutazione finora
- 'Princess Mom' - The Glinner UpdateDocumento11 pagine'Princess Mom' - The Glinner UpdatemordidacampestreNessuna valutazione finora
- ICHMSI 2020 - Luna - Personalized Human Milk Bank DevelopmentDocumento8 pagineICHMSI 2020 - Luna - Personalized Human Milk Bank DevelopmentgldsbarzolaNessuna valutazione finora
- Latest Report Template Per BrandDocumento139 pagineLatest Report Template Per BrandYamato De Jesus NakazawaNessuna valutazione finora
- How To Raise An Amazing ChildDocumento197 pagineHow To Raise An Amazing ChildMersi Ta100% (8)
- Annotated BibliographyDocumento12 pagineAnnotated Bibliographyapi-283415527Nessuna valutazione finora
- Perawatan Payudara Untuk Mencegah Bendungan Asi Pada Ibu Post Partum Ria GustiriniDocumento6 paginePerawatan Payudara Untuk Mencegah Bendungan Asi Pada Ibu Post Partum Ria GustiriniEl M RNessuna valutazione finora
- Weaning LeafletDocumento13 pagineWeaning LeafletRinio Simeonidou100% (1)
- 1341-Article Text-4651-2-10-20211223Documento7 pagine1341-Article Text-4651-2-10-20211223Alwiyah amd. kebNessuna valutazione finora
- Benefits of BreastfeedingDocumento5 pagineBenefits of BreastfeedingTaylor SwiftNessuna valutazione finora
- Breast EngorgementDocumento14 pagineBreast EngorgementSumi GNessuna valutazione finora
- Benefits of BreastfeedingDocumento2 pagineBenefits of BreastfeedingESPINOSA JHANNANessuna valutazione finora
- Relactation WebinarDocumento30 pagineRelactation WebinarDelia ParamithaNessuna valutazione finora
- Breast Feeding FactsDocumento4 pagineBreast Feeding FactsJennifer VelascoNessuna valutazione finora
- WIC BF Info PumpingAndStoringBreastmilkForYourBaby PDFDocumento2 pagineWIC BF Info PumpingAndStoringBreastmilkForYourBaby PDFMarkGuirhemNessuna valutazione finora
- Lactation Management Training SampleDocumento12 pagineLactation Management Training SampleCart Sunrise100% (1)
- HTP BreastfeedingDocumento2 pagineHTP BreastfeedingSalvara Jane DanielNessuna valutazione finora