Potrebbero piacerti anche
- Living with Metastatic Breast Cancer: Stories of Faith and HopeDa EverandLiving with Metastatic Breast Cancer: Stories of Faith and HopeNessuna valutazione finora
- 7 ExciDocumento4 pagine7 Exciemaqtr2018Nessuna valutazione finora
- Research ReportDocumento13 pagineResearch Reportapi-662910690Nessuna valutazione finora
- 45 FullDocumento2 pagine45 FullIsaias PrestesNessuna valutazione finora
- Falope RM Chapter 1 (18518)Documento7 pagineFalope RM Chapter 1 (18518)falopetaiwo.12Nessuna valutazione finora
- Nursing Research PaperDocumento14 pagineNursing Research Paperapi-545895101Nessuna valutazione finora
- Ca de MamaDocumento39 pagineCa de MamaMedicina Lo MejorNessuna valutazione finora
- Breast Cancer ScreeningDocumento13 pagineBreast Cancer ScreeningAinsley PNessuna valutazione finora
- Controversies RegardingDocumento15 pagineControversies RegardingCharlie BrownNessuna valutazione finora
- Breast Cancer Detection 2Documento2 pagineBreast Cancer Detection 2gpicaulyNessuna valutazione finora
- hsc402 ProblemjustificationDocumento9 paginehsc402 Problemjustificationapi-356117299Nessuna valutazione finora
- Cervical Cancer Thesis StatementDocumento6 pagineCervical Cancer Thesis StatementBecky Goins100% (2)
- Breast Cancer ScreeningDocumento21 pagineBreast Cancer ScreeningBolivar Isea100% (1)
- Factors Influencing On The Compliance of Breast Self-Examination of Nurses in A Local Area)Documento4 pagineFactors Influencing On The Compliance of Breast Self-Examination of Nurses in A Local Area)Dyam MitchNessuna valutazione finora
- Recommendation Report-1Documento8 pagineRecommendation Report-1api-346638602Nessuna valutazione finora
- Breast Cancer Thesis PDFDocumento7 pagineBreast Cancer Thesis PDFPaySomeoneToWritePaperCanada100% (2)
- Nursing CourseDocumento8 pagineNursing Coursepatel ravirajNessuna valutazione finora
- Guidelines PDFDocumento6 pagineGuidelines PDFvilla88Nessuna valutazione finora
- Fabian Ashley - Evaluating Secondary Cancer Prevention and The Role of NursesDocumento10 pagineFabian Ashley - Evaluating Secondary Cancer Prevention and The Role of Nursesapi-662856597Nessuna valutazione finora
- Breast Cancer DetectionDocumento5 pagineBreast Cancer DetectionalexlingmanchesterNessuna valutazione finora
- Breast Imaging: Linei Urban and Cicero UrbanDocumento22 pagineBreast Imaging: Linei Urban and Cicero UrbanmaytorenacgerNessuna valutazione finora
- Breast ScreeningDocumento10 pagineBreast ScreeningErick MuthengiNessuna valutazione finora
- Breast Cancer Risk Factors Literature ReviewDocumento8 pagineBreast Cancer Risk Factors Literature Reviewafdtvdcwf100% (1)
- Knowing It Exists Is Not Enough, Get Inform, Pass It OnDocumento29 pagineKnowing It Exists Is Not Enough, Get Inform, Pass It OnIretiola AdeleruNessuna valutazione finora
- Community Medicine (Update1 0)Documento30 pagineCommunity Medicine (Update1 0)hafsah sidi abdullahiNessuna valutazione finora
- Thesis FinalDocumento82 pagineThesis FinalPalwasha KhanNessuna valutazione finora
- Female University Students' Health Beliefs Regarding Tsaerb Cancer Early Detection Screening MeasurementsDocumento7 pagineFemale University Students' Health Beliefs Regarding Tsaerb Cancer Early Detection Screening MeasurementsAsmi AtikaNessuna valutazione finora
- 503 837 1 PBDocumento14 pagine503 837 1 PB5m7m2c2kryNessuna valutazione finora
- American Cancer Society Guidelines For Breast Cancer Screening: Update 2003Documento30 pagineAmerican Cancer Society Guidelines For Breast Cancer Screening: Update 2003Jose MahechaNessuna valutazione finora
- Dissertation On Cervical Cancer ScreeningDocumento7 pagineDissertation On Cervical Cancer ScreeningSomeToWriteMyPaperUK100% (1)
- CA A Cancer J Clinicians - January February 1998 - Cady - Evaluation of Common Breast Problems Guidance For Primary CareDocumento15 pagineCA A Cancer J Clinicians - January February 1998 - Cady - Evaluation of Common Breast Problems Guidance For Primary CareNelson William UsnayoNessuna valutazione finora
- Week 2 Health Impact PaperDocumento8 pagineWeek 2 Health Impact PaperMakhdoom Zain Ul AbdinNessuna valutazione finora
- Cervical Cancer Screening ThesisDocumento6 pagineCervical Cancer Screening Thesisbk1svxmr100% (3)
- Breast Cancer Staging PDFDocumento12 pagineBreast Cancer Staging PDFDanu BagoesNessuna valutazione finora
- Review: Risk Factors For Breast Cancer For Women Aged 40 To 49 YearsDocumento16 pagineReview: Risk Factors For Breast Cancer For Women Aged 40 To 49 YearsMeidy WerorNessuna valutazione finora
- Breast CancerDocumento17 pagineBreast CancerLaura CampañaNessuna valutazione finora
- Ethics of ScreeningDocumento10 pagineEthics of ScreeningTEACHBayviewNessuna valutazione finora
- Prophylactic MastectomyDocumento5 pagineProphylactic MastectomyMuhammad Darussalam DarwisNessuna valutazione finora
- SennettresearchfinalpaperDocumento5 pagineSennettresearchfinalpaperapi-490058714Nessuna valutazione finora
- Cuarteros, Richiel MDocumento2 pagineCuarteros, Richiel Mjanna mae patriarcaNessuna valutazione finora
- Breast Cancer Awareness Thesis StatementDocumento4 pagineBreast Cancer Awareness Thesis Statementhmnxivief100% (1)
- EBM2Documento8 pagineEBM2ica ssNessuna valutazione finora
- Clinical Oncology: World Journal ofDocumento13 pagineClinical Oncology: World Journal ofMATEJ MAMICNessuna valutazione finora
- Cancer Screening - Health Impact, Prevalence, Correlates and InterventionsDocumento38 pagineCancer Screening - Health Impact, Prevalence, Correlates and InterventionsMary OvbieboNessuna valutazione finora
- Factors Associated With Breast Cancer Mammographic Screening Behavior Among Iranian WomenDocumento6 pagineFactors Associated With Breast Cancer Mammographic Screening Behavior Among Iranian Womenx2.7.astiNessuna valutazione finora
- Breast Cancer ReflectionDocumento4 pagineBreast Cancer ReflectionCAJES NOLINessuna valutazione finora
- Dissertation Ovarian CancerDocumento12 pagineDissertation Ovarian CancerWriteMyPaperForCheapCanada100% (1)
- Brief: Ovarian Cancers: Evolving Paradigms in Research and CareDocumento4 pagineBrief: Ovarian Cancers: Evolving Paradigms in Research and CareFrancesco MultinuNessuna valutazione finora
- OutDocumento7 pagineOutDIAN K.A BEREBEINNessuna valutazione finora
- Master Thesis Breast CancerDocumento8 pagineMaster Thesis Breast Cancerafkodkedr100% (2)
- Breast Cancer Screening ThesisDocumento6 pagineBreast Cancer Screening ThesisThesisPapersForSaleUK100% (2)
- Literature Review On Cervical Cancer ScreeningDocumento4 pagineLiterature Review On Cervical Cancer Screeningbqvlqjugf100% (1)
- Free Research Paper On Cervical CancerDocumento6 pagineFree Research Paper On Cervical Cancerafedonkfh100% (1)
- American Cancer SocietyDocumento56 pagineAmerican Cancer SocietyranaNessuna valutazione finora
- 2207OBG EvidenceDocumento2 pagine2207OBG EvidenceSandeep SharmaNessuna valutazione finora
- Cervical Cancer ThesisDocumento8 pagineCervical Cancer Thesisafbteuawc100% (2)
- 38565-Article Text-106129-3-10-20200930Documento5 pagine38565-Article Text-106129-3-10-20200930kirito azumaNessuna valutazione finora
- Breast Self-Examination: Knowledge and Practice Among Nurses in United Arab EmiratesDocumento4 pagineBreast Self-Examination: Knowledge and Practice Among Nurses in United Arab EmiratesMuhammad AlfianNessuna valutazione finora
- EJ1078866Documento12 pagineEJ1078866valentinasecivirNessuna valutazione finora
- Unit - 8Documento44 pagineUnit - 8prathibaNessuna valutazione finora
- Yale - Abnormal Uterine Bleeding Preceptor - 389620 - 284 - 45546 - v1Documento12 pagineYale - Abnormal Uterine Bleeding Preceptor - 389620 - 284 - 45546 - v1omegasauron0gmailcomNessuna valutazione finora
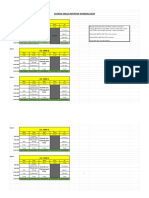
- CSI Schedule 2019-2020Documento2 pagineCSI Schedule 2019-2020omegasauron0gmailcomNessuna valutazione finora
- Remediating The Struggling ResidentDocumento52 pagineRemediating The Struggling Residentomegasauron0gmailcomNessuna valutazione finora
- Ccu Survival GuideDocumento10 pagineCcu Survival Guideomegasauron0gmailcom100% (1)
- Mary Clare Higgins-Chen, MD, MPH Donna Windish, MD, MPH: Alopecia Week 25Documento9 pagineMary Clare Higgins-Chen, MD, MPH Donna Windish, MD, MPH: Alopecia Week 25omegasauron0gmailcomNessuna valutazione finora
- EBM Therapy and Diagnosis-Interpretation of Results ExerciseDocumento3 pagineEBM Therapy and Diagnosis-Interpretation of Results Exerciseomegasauron0gmailcomNessuna valutazione finora
- Welcome To UNC Hematology/Oncology!Documento80 pagineWelcome To UNC Hematology/Oncology!omegasauron0gmailcomNessuna valutazione finora
- AM Curriculum Review-2019-2020Documento3 pagineAM Curriculum Review-2019-2020omegasauron0gmailcomNessuna valutazione finora
- Allergy H&PDocumento3 pagineAllergy H&Pomegasauron0gmailcomNessuna valutazione finora
- EBM Video TutorialsDocumento1 paginaEBM Video Tutorialsomegasauron0gmailcomNessuna valutazione finora
- Therapy Article questions-ALLHATDocumento2 pagineTherapy Article questions-ALLHATomegasauron0gmailcomNessuna valutazione finora
- Supplemental Guide For Allergy and ImmunologyDocumento52 pagineSupplemental Guide For Allergy and Immunologyomegasauron0gmailcomNessuna valutazione finora
- Breast LectureDocumento98 pagineBreast LectureTopher ReyesNessuna valutazione finora
- 0607 Nbccedp Fs PDFDocumento4 pagine0607 Nbccedp Fs PDFNunung BuchoriNessuna valutazione finora
- CPG - Management of Breast Cancer (2nd Edition)Documento100 pagineCPG - Management of Breast Cancer (2nd Edition)umiraihana1Nessuna valutazione finora
- Capstone Project MethodologyDocumento7 pagineCapstone Project MethodologyTushar GNessuna valutazione finora
- Breast Imagingand InterventionalDocumento353 pagineBreast Imagingand Interventionalservice iyadMedicalNessuna valutazione finora
- FMcase 1Documento24 pagineFMcase 1Ryan Townsend100% (2)
- Reading Task 1-Breast Cancer and The ElderlyDocumento6 pagineReading Task 1-Breast Cancer and The ElderlyJats_Fru_1741100% (5)
- Birads 2013Documento6 pagineBirads 2013Citlaly RojasNessuna valutazione finora
- 380 (Olive Peart) Lange QA Mammography Examination PDFDocumento186 pagine380 (Olive Peart) Lange QA Mammography Examination PDFGabriel Callupe100% (1)
- Breast Cancer Awareness (2023)Documento2 pagineBreast Cancer Awareness (2023)The Livingston County NewsNessuna valutazione finora
- Referat CA MamaeDocumento101 pagineReferat CA MamaeNalathifaNessuna valutazione finora
- Breast 46Documento16 pagineBreast 46ahmad.aljaberiNessuna valutazione finora
- Meng Mammogram JulDocumento4 pagineMeng Mammogram JulLivia MillNessuna valutazione finora
- Reiser DBTDocumento10 pagineReiser DBTMelanie DascăluNessuna valutazione finora
- The American College of Radiology BI-RADS Atlas 5 Edition: Frequently Asked QuestionsDocumento18 pagineThe American College of Radiology BI-RADS Atlas 5 Edition: Frequently Asked QuestionssatanioNessuna valutazione finora
- BI-RADS Classification For Management of Abnormal MammogramsDocumento4 pagineBI-RADS Classification For Management of Abnormal MammogramsRaweewan ThanetphonkunNessuna valutazione finora
- A Study To Assess The Effectiveness of StructuredDocumento26 pagineA Study To Assess The Effectiveness of StructuredGopalLandge100% (1)
- Digital Mammography Novel Applications. Radiologic Clinics of North AmericaDocumento13 pagineDigital Mammography Novel Applications. Radiologic Clinics of North AmericaEduardo Alejandro IIINessuna valutazione finora
- Research ProposalDocumento21 pagineResearch Proposalapi-351044176Nessuna valutazione finora
- 1485 Digital Breast TomosynthesisDocumento156 pagine1485 Digital Breast TomosynthesisWinston Mauricio Casco SobalvarroNessuna valutazione finora
- 19-Mammography Positioning (FreeDownloadBooksForRadiographer)Documento105 pagine19-Mammography Positioning (FreeDownloadBooksForRadiographer)إسلام الجزيري100% (2)
- Global Saini Tomayo Case Study FinalDocumento4 pagineGlobal Saini Tomayo Case Study FinalAsim AliNessuna valutazione finora
- Tomosynthesis in Diagnostic Mammography: Reni Butler - Regina J. HooleyDocumento17 pagineTomosynthesis in Diagnostic Mammography: Reni Butler - Regina J. HooleyNimeniNessuna valutazione finora
- 12 Neha Dahiya 2017 Knowledge and Practices Related To Screening For Breast Cancer Among Women in Delhi IndiaDocumento5 pagine12 Neha Dahiya 2017 Knowledge and Practices Related To Screening For Breast Cancer Among Women in Delhi IndiaArick Frendi AndriyanNessuna valutazione finora
- Group Capstone TusharDocumento14 pagineGroup Capstone TusharTushar GNessuna valutazione finora
- Breast CancerDocumento8 pagineBreast CancerJeyser T. Gamutia100% (1)
- Cancer Screening in Older AdultsDocumento13 pagineCancer Screening in Older AdultsEsteban MatusNessuna valutazione finora
- Screening of Breast CancerDocumento19 pagineScreening of Breast CancerIncredible DivineNessuna valutazione finora
- Medcosmossurgery Blogspot inDocumento40 pagineMedcosmossurgery Blogspot inSajag GuptaNessuna valutazione finora
- 10 Abdulmohsen H. Al-Zalabani 2016 Breast Cancer Knowledge and Screening Practice and Barriers Among Women in Madinah Saudi ArabiaDocumento7 pagine10 Abdulmohsen H. Al-Zalabani 2016 Breast Cancer Knowledge and Screening Practice and Barriers Among Women in Madinah Saudi ArabiaArick Frendi AndriyanNessuna valutazione finora
- Love Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)Da EverandLove Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)Valutazione: 3 su 5 stelle3/5 (1)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionDa EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionValutazione: 4 su 5 stelle4/5 (404)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsDa EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNessuna valutazione finora
- The Age of Magical Overthinking: Notes on Modern IrrationalityDa EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityValutazione: 4 su 5 stelle4/5 (31)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisDa EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisValutazione: 4.5 su 5 stelle4.5/5 (42)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDDa EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDValutazione: 5 su 5 stelle5/5 (3)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeDa EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeValutazione: 2 su 5 stelle2/5 (1)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedDa EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedValutazione: 4.5 su 5 stelle4.5/5 (82)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryDa EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryValutazione: 4 su 5 stelle4/5 (46)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaDa EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaValutazione: 4.5 su 5 stelle4.5/5 (266)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsDa EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsValutazione: 4 su 5 stelle4/5 (4)
- The Obesity Code: Unlocking the Secrets of Weight LossDa EverandThe Obesity Code: Unlocking the Secrets of Weight LossValutazione: 4 su 5 stelle4/5 (6)
- Manipulation: The Ultimate Guide To Influence People with Persuasion, Mind Control and NLP With Highly Effective Manipulation TechniquesDa EverandManipulation: The Ultimate Guide To Influence People with Persuasion, Mind Control and NLP With Highly Effective Manipulation TechniquesValutazione: 4.5 su 5 stelle4.5/5 (1412)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsDa EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsValutazione: 5 su 5 stelle5/5 (1)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Da EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Valutazione: 4.5 su 5 stelle4.5/5 (110)
- Why We Die: The New Science of Aging and the Quest for ImmortalityDa EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityValutazione: 4 su 5 stelle4/5 (5)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsDa EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsValutazione: 4.5 su 5 stelle4.5/5 (170)
- Summary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisDa EverandSummary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisValutazione: 5 su 5 stelle5/5 (8)
- When the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisDa EverandWhen the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisValutazione: 3.5 su 5 stelle3.5/5 (2)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessDa EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessValutazione: 4.5 su 5 stelle4.5/5 (328)
- Troubled: A Memoir of Foster Care, Family, and Social ClassDa EverandTroubled: A Memoir of Foster Care, Family, and Social ClassValutazione: 4.5 su 5 stelle4.5/5 (27)
- Dark Psychology: Learn To Influence Anyone Using Mind Control, Manipulation And Deception With Secret Techniques Of Dark Persuasion, Undetected Mind Control, Mind Games, Hypnotism And BrainwashingDa EverandDark Psychology: Learn To Influence Anyone Using Mind Control, Manipulation And Deception With Secret Techniques Of Dark Persuasion, Undetected Mind Control, Mind Games, Hypnotism And BrainwashingValutazione: 4 su 5 stelle4/5 (1138)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeDa EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeValutazione: 4.5 su 5 stelle4.5/5 (253)