Potrebbero piacerti anche
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- 6th Central Pay Commission Salary CalculatorDocumento15 pagine6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (74)
- ENT Mnemonics 1Documento13 pagineENT Mnemonics 1Riham Mohye Eldeen Mohammed88% (8)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- Specific Indications in Clinical PracticeDocumento58 pagineSpecific Indications in Clinical PracticeOccult Librarian100% (5)
- The Infant of An Addicted MotherDocumento15 pagineThe Infant of An Addicted Mothernursereview100% (8)
- Critical Care Total MRCS Part BDocumento21 pagineCritical Care Total MRCS Part BSnehanshNessuna valutazione finora
- Tea Blending Unit: Profile No.: 211 NIC Code: 10791Documento12 pagineTea Blending Unit: Profile No.: 211 NIC Code: 10791P AgarwalNessuna valutazione finora
- FLCCC Protocols - A Guide To The Management of COVID 19 PDFDocumento39 pagineFLCCC Protocols - A Guide To The Management of COVID 19 PDFSteph Cliche100% (2)
- Neonatal SepsisDocumento18 pagineNeonatal SepsisMoe KebabNessuna valutazione finora
- Policies On Rational Antimicrobial Use Based On The Hospital Antibiogram and Survailance of AmrDocumento10 paginePolicies On Rational Antimicrobial Use Based On The Hospital Antibiogram and Survailance of AmrAnonymous jQM5jMK0100% (3)
- Medical-Surgical Nursing Assessment and Management of Clinical Problems 9e Chapter 67Documento11 pagineMedical-Surgical Nursing Assessment and Management of Clinical Problems 9e Chapter 67sarasjunkNessuna valutazione finora
- Clinical Case Report Powerpoint PresentationDocumento24 pagineClinical Case Report Powerpoint Presentationapi-354139540100% (1)
- Updated Sixteenth Adult List enDocumento43 pagineUpdated Sixteenth Adult List enFikin AminuNessuna valutazione finora
- Helpage India GuideDocumento84 pagineHelpage India Guidesumit1975Nessuna valutazione finora
- Prevalence, Awareness, and Control of Hypertension in The Slums of KolkataDocumento9 paginePrevalence, Awareness, and Control of Hypertension in The Slums of KolkataIndadul MozumdarNessuna valutazione finora
- Salt and High Blood Pressure: Sailesh MOHAN and Norm R. C. CAMPBELLDocumento11 pagineSalt and High Blood Pressure: Sailesh MOHAN and Norm R. C. CAMPBELLIndadul MozumdarNessuna valutazione finora
- Sbi Login Dup PWDDocumento2 pagineSbi Login Dup PWDapi-3792961Nessuna valutazione finora
- Final Merit List of Candidates For Counselling For The Post of MO (MBBS) 1 Year Compulsory Rural Posting Under NHM, AssamDocumento38 pagineFinal Merit List of Candidates For Counselling For The Post of MO (MBBS) 1 Year Compulsory Rural Posting Under NHM, AssamIndadul MozumdarNessuna valutazione finora
- How To Start A Business Enterprise PDFDocumento22 pagineHow To Start A Business Enterprise PDFDhana RedNessuna valutazione finora
- Salt and High Blood Pressure: Sailesh MOHAN and Norm R. C. CAMPBELLDocumento11 pagineSalt and High Blood Pressure: Sailesh MOHAN and Norm R. C. CAMPBELLIndadul MozumdarNessuna valutazione finora
- Mustafa QutationsDocumento1 paginaMustafa QutationsIndadul MozumdarNessuna valutazione finora
- Interim Report APEDA 21 Sep Final PDFDocumento10 pagineInterim Report APEDA 21 Sep Final PDFIndadul MozumdarNessuna valutazione finora
- Interim Report APEDA 21 Sep Final PDFDocumento10 pagineInterim Report APEDA 21 Sep Final PDFIndadul MozumdarNessuna valutazione finora
- Guidelines For: University Grants Commission Bhadur Shah Zafar Marg NEW DELHI - 110 002Documento4 pagineGuidelines For: University Grants Commission Bhadur Shah Zafar Marg NEW DELHI - 110 002tushar sharmaNessuna valutazione finora
- Retaxis Cost&FeatureSheet B2BMarketplace SAAS IndadDocumento14 pagineRetaxis Cost&FeatureSheet B2BMarketplace SAAS IndadIndadul MozumdarNessuna valutazione finora
- 03 Brain BasicsDocumento25 pagine03 Brain BasicsarseniosilvaNessuna valutazione finora
- 9781904627241Documento30 pagine9781904627241HyhyiNessuna valutazione finora
- Neurological Exam Lecture NotesDocumento26 pagineNeurological Exam Lecture NotesNaveen KovalNessuna valutazione finora
- Show PDFDocumento2 pagineShow PDFIndadul MozumdarNessuna valutazione finora
- HospitalDocumento6 pagineHospitalIndadul MozumdarNessuna valutazione finora
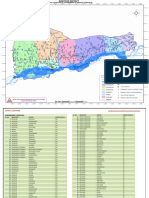
- Village ListDocumento15 pagineVillage ListIndadul MozumdarNessuna valutazione finora
- Nsap GuidelinesDocumento56 pagineNsap GuidelinesArnik JainNessuna valutazione finora
- Delhi Medical 19 4Documento20 pagineDelhi Medical 19 4Paras AhujaNessuna valutazione finora
- EMS Concept PaperDocumento18 pagineEMS Concept PaperRahul Shastri100% (2)
- PharmaDocumento10 paginePharmaIndadul MozumdarNessuna valutazione finora
- Iron Plus Initiative For 6 Months - 5 YearsDocumento2 pagineIron Plus Initiative For 6 Months - 5 Yearsprasenjit_gayenNessuna valutazione finora
- BhmsDocumento4 pagineBhmsIndadul MozumdarNessuna valutazione finora
- EducationDocumento1 paginaEducationIndadul MozumdarNessuna valutazione finora
- Top 100 Secrets About Critical CareDocumento8 pagineTop 100 Secrets About Critical CareMariaUlfaNessuna valutazione finora
- Nutritional Management in Critically Ill ConditionDocumento30 pagineNutritional Management in Critically Ill Conditiondwi ayieNessuna valutazione finora
- E Coli 2016Documento27 pagineE Coli 2016alanbecker_alNessuna valutazione finora
- Critical Appraisal RCTDocumento7 pagineCritical Appraisal RCTAisya FikritamaNessuna valutazione finora
- An In-Vitro Study of Antimicrobial Activity of Homoeopathic Medicine Pyrogenium Against Escherichia ColiDocumento5 pagineAn In-Vitro Study of Antimicrobial Activity of Homoeopathic Medicine Pyrogenium Against Escherichia ColiAghosh B Prasad100% (1)
- 03 - Neonatal Intestinal ObstructionDocumento28 pagine03 - Neonatal Intestinal Obstructionmahmoud khaledNessuna valutazione finora
- Shock - Critical Care Medicine - MSD Manual Professional EditionDocumento11 pagineShock - Critical Care Medicine - MSD Manual Professional Editionazaria zhafirahNessuna valutazione finora
- Chapter 39 - What Is The Role of Empirical Antibiotic Therapy in SepsisDocumento16 pagineChapter 39 - What Is The Role of Empirical Antibiotic Therapy in SepsisIkhlasul Amal WellNessuna valutazione finora
- Forensic MnemonicsDocumento9 pagineForensic MnemonicsVijay KumarNessuna valutazione finora
- 2014 Paediatric Sepsis 6 v10Documento2 pagine2014 Paediatric Sepsis 6 v10Nisar ShaikNessuna valutazione finora
- Best Practice & Research Clinical RheumatologyDocumento15 pagineBest Practice & Research Clinical RheumatologyTatiana GonzalezNessuna valutazione finora
- Benefits of Marketing Information System (MIS) : 1. Prediction of Consumer DemandDocumento9 pagineBenefits of Marketing Information System (MIS) : 1. Prediction of Consumer DemandGorebet GpsNessuna valutazione finora
- Sepsis 2018 Definitions and Guideline Changes PDFDocumento9 pagineSepsis 2018 Definitions and Guideline Changes PDFSyahrul HamidNessuna valutazione finora
- Crystalloids Versus Colloids Exploring.17Documento14 pagineCrystalloids Versus Colloids Exploring.17Maria Siachoque JaraNessuna valutazione finora
- 1630362901-Efficacy of Brazilian Green Propolis As An Adjunct Treatment For Hospitalized Covid-19 Patients - Review JournalDocumento11 pagine1630362901-Efficacy of Brazilian Green Propolis As An Adjunct Treatment For Hospitalized Covid-19 Patients - Review JournalTheo RadityaNessuna valutazione finora
- Noncardiogenic Pulmonary Edema - UpToDateDocumento17 pagineNoncardiogenic Pulmonary Edema - UpToDateStefani AtlleNessuna valutazione finora
- Paediatrica IndonesianaDocumento6 paginePaediatrica IndonesianayusrinastitiNessuna valutazione finora
- Shock - StatPearls - NCBI BookshelfDocumento5 pagineShock - StatPearls - NCBI BookshelfSYAFIRA LAILA NURULITANessuna valutazione finora
- Expert Statement For Management Hypovolemia in Sepsis PDFDocumento8 pagineExpert Statement For Management Hypovolemia in Sepsis PDFRobi HeryantoNessuna valutazione finora
- PSMID Covid Guidelines March 31, 20208080312298125101472Documento62 paginePSMID Covid Guidelines March 31, 20208080312298125101472Rina Fajardo - NacinNessuna valutazione finora
- Postoperative Enterocutaneous FistulaDocumento10 paginePostoperative Enterocutaneous FistulaJoon RaynerNessuna valutazione finora
- Severe Sepsis Is Sepsis CausingDocumento6 pagineSevere Sepsis Is Sepsis CausingHerryanto AgustriadiNessuna valutazione finora