Potrebbero piacerti anche
- EM Basic Chest Pain: Pet Mac P E T M A CDocumento7 pagineEM Basic Chest Pain: Pet Mac P E T M A CAkanksha VermaNessuna valutazione finora
- Common Calls For InternsDocumento1 paginaCommon Calls For Internstheusuals100% (1)
- EM Basic - Pocket GuideDocumento97 pagineEM Basic - Pocket Guidemainertoo100% (2)
- Acute Care: James Finnie - Senior RotationDocumento15 pagineAcute Care: James Finnie - Senior RotationFarhanaNessuna valutazione finora
- Pulmonary Thrombo EmbolismDocumento3 paginePulmonary Thrombo EmbolismTom MallinsonNessuna valutazione finora
- EM Basic-Altered Mental Status (AMS)Documento2 pagineEM Basic-Altered Mental Status (AMS)Sara ZareiNessuna valutazione finora
- Inbound 2469239670550275995Documento17 pagineInbound 2469239670550275995BALCAC Eloisa Gayle I.Nessuna valutazione finora
- IM ReviewDocumento4 pagineIM ReviewPäw YusophNessuna valutazione finora
- Reviewer For DutyDocumento4 pagineReviewer For DutyBenedict James BermasNessuna valutazione finora
- Neuro Form 1Documento2 pagineNeuro Form 1skylar0% (1)
- Respiratory Paediatrics ExaminationDocumento1 paginaRespiratory Paediatrics ExaminationRatnahKumar28Nessuna valutazione finora
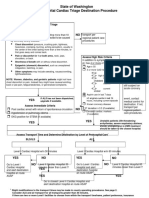
- State of Washington Prehospital Cardiac Triage Destination ProcedureDocumento4 pagineState of Washington Prehospital Cardiac Triage Destination ProcedureNanda Dwi Bintoro ZiehenShopNessuna valutazione finora
- Pediatric Emergencies DR CruzDocumento7 paginePediatric Emergencies DR CruzJustine MembridoNessuna valutazione finora
- NTILS GuideDocumento11 pagineNTILS GuideNeil ThomasNessuna valutazione finora
- Tetralogy of Fallot - LantiDocumento5 pagineTetralogy of Fallot - LantiChristian LantanoNessuna valutazione finora
- Protocol 13: Chest Pain: A&E DoctorDocumento4 pagineProtocol 13: Chest Pain: A&E DoctorVanessa HermioneNessuna valutazione finora
- Perfusion, Class 11 ReviewedDocumento45 paginePerfusion, Class 11 ReviewedMelissa GPNessuna valutazione finora
- Merge Live Online Nle Review 2021: Anatomy of The Nle (Nurse Licensure Examination)Documento16 pagineMerge Live Online Nle Review 2021: Anatomy of The Nle (Nurse Licensure Examination)Johnmer Avelino100% (1)
- Chest Pain: Sumit Bose, MD PGY-3Documento55 pagineChest Pain: Sumit Bose, MD PGY-3Irfan100% (1)
- Sindroma Koroner Akut: World Heart Day 29 SEPTEMBER 2021Documento68 pagineSindroma Koroner Akut: World Heart Day 29 SEPTEMBER 2021Dafhina Store100% (1)
- Cardio MTB 2:3 Notes DONEDocumento10 pagineCardio MTB 2:3 Notes DONESumatt KaurNessuna valutazione finora
- Departemen Kardiologi FK USU RSUP. H. Adam Malik MedanDocumento64 pagineDepartemen Kardiologi FK USU RSUP. H. Adam Malik MedanBonitavanyNessuna valutazione finora
- To KnowDocumento5 pagineTo KnowDalwadi1Nessuna valutazione finora
- Chest Pain Investigation Diagnosis and TreatmentDocumento4 pagineChest Pain Investigation Diagnosis and TreatmentHadsabsaNessuna valutazione finora
- Cardiopulmonary Ressucitation: Presented by Siwani Rai M.Sc. Nursing-IDocumento39 pagineCardiopulmonary Ressucitation: Presented by Siwani Rai M.Sc. Nursing-ISiwani raiNessuna valutazione finora
- Approach To Chest PainDocumento52 pagineApproach To Chest PainChris Jardine LiNessuna valutazione finora
- CN 118 - Assessment (Reviewer)Documento5 pagineCN 118 - Assessment (Reviewer)Camille SanguyoNessuna valutazione finora
- Pulmonary Embolism - International Emergency Medicine Education ProjectDocumento24 paginePulmonary Embolism - International Emergency Medicine Education ProjectקרוליינהסתםחולםNessuna valutazione finora
- Satjit Bhusri, MD Cardiologist Lenox Hill Hospital: Jeff Chianfagna Rpa-CDocumento76 pagineSatjit Bhusri, MD Cardiologist Lenox Hill Hospital: Jeff Chianfagna Rpa-CAjaz JunachNessuna valutazione finora
- Morning Report: Department of Internal MedicineDocumento11 pagineMorning Report: Department of Internal MedicineSharly Ayu PuspitaNessuna valutazione finora
- NBME CMS Forms NotesDocumento4 pagineNBME CMS Forms NotesJack Guccione100% (7)
- MEGACODEDocumento6 pagineMEGACODESafety JNessuna valutazione finora
- NCM 118Documento8 pagineNCM 118Zanie CruzNessuna valutazione finora
- Chest Pain - Investigation, Diagnosis and TreatmentDocumento5 pagineChest Pain - Investigation, Diagnosis and Treatmentsoumabho paruiNessuna valutazione finora
- Nean Salubre-Ansale, RN: CU, Clinical InstructorDocumento23 pagineNean Salubre-Ansale, RN: CU, Clinical InstructorNean Salubre AnsaleNessuna valutazione finora
- Word AssociationDocumento27 pagineWord AssociationMilan Kolovrat100% (1)
- (Nelson Hour) The CV System - HX and PEDocumento30 pagine(Nelson Hour) The CV System - HX and PEJustin Ng SincoNessuna valutazione finora
- IMA Nurse KKV SaifurDocumento69 pagineIMA Nurse KKV Saifureva munartyNessuna valutazione finora
- Word Association PANCEDocumento31 pagineWord Association PANCEnevmerka100% (1)
- Cardiovascular System: By: Marc Anthony Liao RNDocumento59 pagineCardiovascular System: By: Marc Anthony Liao RNloveseeker06Nessuna valutazione finora
- Chest Pain: LSU Medical Student Clerkship, New Orleans, LADocumento56 pagineChest Pain: LSU Medical Student Clerkship, New Orleans, LAGlucose DRglucoseNessuna valutazione finora
- By: DR - Wesam AbdelazizDocumento48 pagineBy: DR - Wesam AbdelazizTIRTH GANATRANessuna valutazione finora
- This Study Resource Was: Assessment & Reasoning Cardiac SystemDocumento6 pagineThis Study Resource Was: Assessment & Reasoning Cardiac SystemSharon TanveerNessuna valutazione finora
- Word AssociationDocumento31 pagineWord Associationjr_brewerNessuna valutazione finora
- Arrythmias and Cardiac TumorsDocumento30 pagineArrythmias and Cardiac TumorsRabea DiaNessuna valutazione finora
- Back Pain: Group 4Documento71 pagineBack Pain: Group 4Cesar Guico Jr.Nessuna valutazione finora
- ATLSDocumento9 pagineATLSAdi Dharmawan100% (7)
- NAC Osce NotesDocumento34 pagineNAC Osce NotesInAbsentia675% (4)
- Cardiovascular: Stable Angina PectorisDocumento2 pagineCardiovascular: Stable Angina PectoriselverineNessuna valutazione finora
- Cardiology Plabable PDFDocumento22 pagineCardiology Plabable PDFTirtha Taposh100% (1)
- How and When Are Defibrillation and Synchronized Cardioversion Done?Documento14 pagineHow and When Are Defibrillation and Synchronized Cardioversion Done?Catherine Dettelbach LakeNessuna valutazione finora
- Reading Reference 3-Approach To Chest PainDocumento14 pagineReading Reference 3-Approach To Chest PainVarshini Tamil SelvanNessuna valutazione finora
- Acute Coronary SyndromeDocumento36 pagineAcute Coronary SyndromeSiti FatimahNessuna valutazione finora
- UK Medical AbbreviationsDocumento5 pagineUK Medical AbbreviationsRNessuna valutazione finora
- Cardiovascular SystemDocumento205 pagineCardiovascular Systemizuku midoriyaNessuna valutazione finora
- Chest Pain CBCRDocumento7 pagineChest Pain CBCROsuri MapitigamaNessuna valutazione finora
- CVS Case ProformaDocumento2 pagineCVS Case ProformaRiyaSingh100% (1)
- Pediatric Cardiovascular System History & ExaminationDocumento74 paginePediatric Cardiovascular System History & Examinationعبدالله Abdullah INessuna valutazione finora
- CLS - Chest Pain ACS 2023Documento40 pagineCLS - Chest Pain ACS 2023popaprostu89Nessuna valutazione finora
- The Radiology Handbook: A Pocket Guide to Medical ImagingDa EverandThe Radiology Handbook: A Pocket Guide to Medical ImagingValutazione: 3.5 su 5 stelle3.5/5 (8)
- Eras 2020 Summary ReportDocumento5 pagineEras 2020 Summary ReporthabbouraNessuna valutazione finora
- CAP ObjectivesDocumento1 paginaCAP ObjectiveshabbouraNessuna valutazione finora
- Copd ObjectivesDocumento2 pagineCopd ObjectiveshabbouraNessuna valutazione finora
- Opd EbmDocumento21 pagineOpd EbmhabbouraNessuna valutazione finora
- Dizziness - PPPD Information SheetDocumento8 pagineDizziness - PPPD Information Sheettan_siqi100% (1)
- DiabetesDocumento2 pagineDiabeteshabbouraNessuna valutazione finora
- Reading EKGs IIDocumento7 pagineReading EKGs IIMark Hammerschmidt100% (1)
- Obgyn ObjectivesDocumento4 pagineObgyn ObjectiveshabbouraNessuna valutazione finora
- Chest Pain DifferentialDocumento2 pagineChest Pain DifferentialhabbouraNessuna valutazione finora
- History Taking For A Patient With SyncopeDocumento4 pagineHistory Taking For A Patient With SyncopehabbouraNessuna valutazione finora
- Obstetrics Case TakingDocumento42 pagineObstetrics Case TakingAnusree AnusreervNessuna valutazione finora
- Elderly Patient History TakingDocumento5 pagineElderly Patient History TakinghabbouraNessuna valutazione finora
- Management of Diabetic IndividualDocumento3 pagineManagement of Diabetic IndividualhabbouraNessuna valutazione finora
- Approach To A Patient With FeverDocumento6 pagineApproach To A Patient With FeverhabbouraNessuna valutazione finora
- UVA Family Questions W/ AnswersDocumento60 pagineUVA Family Questions W/ AnswersSamuel Rothschild0% (1)
- What To Ask:: Infection (LRTI)Documento11 pagineWhat To Ask:: Infection (LRTI)habbouraNessuna valutazione finora
- ALTERED BOWEL HABITS AND ABDOMINAL PAIN v.2 SIMPLIFIED Med 1Documento3 pagineALTERED BOWEL HABITS AND ABDOMINAL PAIN v.2 SIMPLIFIED Med 1habbouraNessuna valutazione finora
- Prescription Writing - HandoutDocumento3 paginePrescription Writing - HandouthabbouraNessuna valutazione finora
- H P MedicineDocumento2 pagineH P Medicinerishu2Nessuna valutazione finora
- Cystitis & UrethritisDocumento13 pagineCystitis & UrethritisfemmyNessuna valutazione finora
- How I Use The Evidence in Dysphagia Management (2) : A Question of TasteDocumento3 pagineHow I Use The Evidence in Dysphagia Management (2) : A Question of TasteSpeech & Language Therapy in Practice100% (3)
- Essay On Fracture ComplicationsDocumento9 pagineEssay On Fracture ComplicationsadibahNessuna valutazione finora
- Herpes Zoster: Shingles Acute Posterior GanglionitisDocumento23 pagineHerpes Zoster: Shingles Acute Posterior GanglionitisHannah Clarisse Monge IgniNessuna valutazione finora
- Water Birth PPDocumento5 pagineWater Birth PPAzi SamiNessuna valutazione finora
- A Case of Achalasia Causing Aspiration PneumoniaDocumento5 pagineA Case of Achalasia Causing Aspiration PneumoniafannyNessuna valutazione finora
- DermatologyDocumento30 pagineDermatologyCarlos HernándezNessuna valutazione finora
- Positive and Negative Syndrome Scale (Panss)Documento2 paginePositive and Negative Syndrome Scale (Panss)Cruizer Davis100% (1)
- PWAT (Panographic Wound Assesment Tool) RevisedDocumento4 paginePWAT (Panographic Wound Assesment Tool) RevisedYunie ArmyatiNessuna valutazione finora
- Shwayder, T., Schneider, S. L., Icecreamwala, D., & Jahnke, M. N. (2019) - Longitudinal Observation of Pediatric Dermatology Patients.Documento255 pagineShwayder, T., Schneider, S. L., Icecreamwala, D., & Jahnke, M. N. (2019) - Longitudinal Observation of Pediatric Dermatology Patients.Cristina GilcaNessuna valutazione finora
- Acute Stress Disorder 1Documento22 pagineAcute Stress Disorder 1Seiska MegaNessuna valutazione finora
- Hypertensive Disorders of Pregnancy and AssociatedDocumento10 pagineHypertensive Disorders of Pregnancy and AssociatedMedrechEditorialNessuna valutazione finora
- Gender Identity Disorder Not Otherwise SpecifiedDocumento4 pagineGender Identity Disorder Not Otherwise SpecifiedJona AddatuNessuna valutazione finora
- Feeding Device Shaju V Cherian and Dipu KCDocumento20 pagineFeeding Device Shaju V Cherian and Dipu KCShaju V CherianNessuna valutazione finora
- MRCGP Exam CSA Case Course Courses Chest PainDocumento6 pagineMRCGP Exam CSA Case Course Courses Chest PainMRCGP CSA Prep Courses / CSA courseNessuna valutazione finora
- HyperacusisDocumento5 pagineHyperacusisAve FenixNessuna valutazione finora
- Azide Dextrose BrothDocumento1 paginaAzide Dextrose BrothJHOSELINE KHATERINE RAMIREZ BARBARANNessuna valutazione finora
- HIRA ToolDocumento26 pagineHIRA Toolsreekala2007Nessuna valutazione finora
- Bowel EliminationDocumento5 pagineBowel EliminationDimple Castañeto CalloNessuna valutazione finora
- Tablet PCR Cheat SheetDocumento4 pagineTablet PCR Cheat Sheetapi-253658656Nessuna valutazione finora
- Diastolic DysfunctionDocumento6 pagineDiastolic DysfunctionMarina SecureanuNessuna valutazione finora
- General Physiology: APEC Exam Study NotesDocumento9 pagineGeneral Physiology: APEC Exam Study NotesKC PalattaoNessuna valutazione finora
- Pi Is 0022347617311927Documento1 paginaPi Is 0022347617311927Umesh BabuNessuna valutazione finora
- Effectiveness of Psychotherapy On Suicidal Risk - A Systematic Review of Observational Studies (MENDEZ, Et Al, 2019)Documento10 pagineEffectiveness of Psychotherapy On Suicidal Risk - A Systematic Review of Observational Studies (MENDEZ, Et Al, 2019)JAVIERA CONSTANZA MUÑOZ VERGARANessuna valutazione finora
- Pharmacology McqNEW 2Documento7 paginePharmacology McqNEW 2Ayman Ragab100% (2)
- GRANDPAR-PATHOPHYSIOLOGY-4 (1) Pertusis Whooping Cough Secondary To PneumoniaDocumento5 pagineGRANDPAR-PATHOPHYSIOLOGY-4 (1) Pertusis Whooping Cough Secondary To PneumoniaJustin AlejoNessuna valutazione finora
- Renal, Urinary Systems - ElectrolytesDocumento692 pagineRenal, Urinary Systems - ElectrolytesRoshan MevadaNessuna valutazione finora
- ATT Induced Hepatotoxicity: Dr. K. K. SharmaDocumento36 pagineATT Induced Hepatotoxicity: Dr. K. K. SharmaSucharita Ray100% (1)
- GuideDocumento52 pagineGuidemihaelklajner100% (1)
- Right-Sided Heart Failure: College of NursingDocumento30 pagineRight-Sided Heart Failure: College of NursingMatelyn OargaNessuna valutazione finora