Potrebbero piacerti anche
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- Pain Assessment and Management Strategies 2014Documento14 paginePain Assessment and Management Strategies 2014Dara Agusti MaulidyaNessuna valutazione finora
- Preventing Cognitive Decline in Healthy Older AdultsDocumento5 paginePreventing Cognitive Decline in Healthy Older AdultsDara Agusti MaulidyaNessuna valutazione finora
- Geriatric Pain Management 2014Documento12 pagineGeriatric Pain Management 2014Dara Agusti MaulidyaNessuna valutazione finora
- Exercise Training Effect To CognitiveDocumento21 pagineExercise Training Effect To CognitiveDara Agusti MaulidyaNessuna valutazione finora
- Pain Management in the Elderly: A ReviewDocumento9 paginePain Management in the Elderly: A ReviewDara Agusti MaulidyaNessuna valutazione finora
- Talak HT EmergensiDocumento4 pagineTalak HT EmergensiMelda Kusuma WardaniNessuna valutazione finora
- MR - Hellp SyndromDocumento21 pagineMR - Hellp SyndromDara Agusti MaulidyaNessuna valutazione finora
- Management of Chronic Pain in The Elderly 2018Documento8 pagineManagement of Chronic Pain in The Elderly 2018Dara Agusti MaulidyaNessuna valutazione finora
- RubellaDocumento8 pagineRubellaDara Agusti MaulidyaNessuna valutazione finora
- GeriGrandRounds 2015-8-7Documento63 pagineGeriGrandRounds 2015-8-7Dara Agusti MaulidyaNessuna valutazione finora
- Treatment of Hypertensive Emergencies 2017Documento1 paginaTreatment of Hypertensive Emergencies 2017Dara Agusti MaulidyaNessuna valutazione finora
- Guideline Aust Presc 2017Documento5 pagineGuideline Aust Presc 2017Endrianus Jaya PutraNessuna valutazione finora
- Lancet PDFDocumento11 pagineLancet PDFDara Agusti MaulidyaNessuna valutazione finora
- How I Treat Anemia in PregnancyDocumento11 pagineHow I Treat Anemia in PregnancyDara Agusti MaulidyaNessuna valutazione finora
- Dysmenorrhea and Related DisordersDocumento7 pagineDysmenorrhea and Related DisordersDara Agusti MaulidyaNessuna valutazione finora
- Rubella DuttaDocumento1 paginaRubella DuttaDara Agusti MaulidyaNessuna valutazione finora
- Cover Jilid 1Documento1 paginaCover Jilid 1Syahputra Parlindungan RajagukgukNessuna valutazione finora
- Read - Rubella and PregnancyDocumento8 pagineRead - Rubella and PregnancyDara Agusti MaulidyaNessuna valutazione finora
- Eye Infections PDFDocumento10 pagineEye Infections PDFDara Agusti MaulidyaNessuna valutazione finora
- COVER ReferatDocumento1 paginaCOVER ReferatDara Agusti MaulidyaNessuna valutazione finora
- Pleural Disease 2010 Pneumothorax PDFDocumento14 paginePleural Disease 2010 Pneumothorax PDFArrum Chyntia YuliyantiNessuna valutazione finora
- Instructions To AuthorsDocumento4 pagineInstructions To AuthorsDara Agusti MaulidyaNessuna valutazione finora
- Bab 36 Syok Hipovolemik PDFDocumento2 pagineBab 36 Syok Hipovolemik PDFDara Agusti MaulidyaNessuna valutazione finora
- Periorbital Vs Orbital CellulitisDocumento4 paginePeriorbital Vs Orbital CellulitisDara Agusti MaulidyaNessuna valutazione finora
- Bilateral Orbital Cellulitis Secondary To Furunculosis A Case SeriesDocumento4 pagineBilateral Orbital Cellulitis Secondary To Furunculosis A Case SeriesDara Agusti MaulidyaNessuna valutazione finora
- Submission of ManuscriptDocumento1 paginaSubmission of ManuscriptDara Agusti MaulidyaNessuna valutazione finora
- What Treatment Orbital CellulitisDocumento3 pagineWhat Treatment Orbital CellulitisDara Agusti MaulidyaNessuna valutazione finora
- Bab 25 Terapi OksigenDocumento3 pagineBab 25 Terapi OksigenAndriani Kemala SariNessuna valutazione finora
- Bab 24 Dasar Dasar Penyakit Akibat KerjaDocumento2 pagineBab 24 Dasar Dasar Penyakit Akibat KerjaLim MichaelNessuna valutazione finora
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (890)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (587)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (399)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (73)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (265)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2219)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (119)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
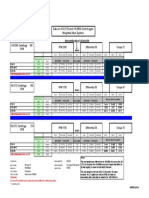
- HS-2172 Vs HS-5500 Test ComparisonDocumento1 paginaHS-2172 Vs HS-5500 Test ComparisonRicardo VillarNessuna valutazione finora
- Chapter 4 Cost MinimizationDocumento6 pagineChapter 4 Cost MinimizationXavier Hetsel Ortega BarraganNessuna valutazione finora
- Nakshatra Exaltation DebilitationDocumento3 pagineNakshatra Exaltation DebilitationBhanu Pinnamaneni100% (1)
- Understanding Earth's History Through Rock CharacteristicsDocumento1 paginaUnderstanding Earth's History Through Rock CharacteristicsSharmaine AcNessuna valutazione finora
- Speech for pecha kuchaDocumento6 pagineSpeech for pecha kuchaaira mikaela ruazolNessuna valutazione finora
- Flame Configurations in A Lean Premixed Dump Combustor With An Annular Swirling FlowDocumento8 pagineFlame Configurations in A Lean Premixed Dump Combustor With An Annular Swirling Flowعبدالله عبدالعاطيNessuna valutazione finora
- The Creators College of Science & Commerce: 1 TermDocumento2 pagineThe Creators College of Science & Commerce: 1 TermJhangir Awan33% (3)
- PepsicoDocumento18 paginePepsicorahil virani0% (1)
- Module 37 Nur 145Documento38 pagineModule 37 Nur 145Marga WreatheNessuna valutazione finora
- Grade 11 Holiday Homework Part 1Documento7 pagineGrade 11 Holiday Homework Part 1Jashfa SaboorNessuna valutazione finora
- YOKOGAWADocumento16 pagineYOKOGAWADavide ContiNessuna valutazione finora
- Enviroclean 25 LTRDocumento1 paginaEnviroclean 25 LTRMaziyarNessuna valutazione finora
- MUCLecture 2021 10311889Documento11 pagineMUCLecture 2021 10311889Ramon Angelo MendezNessuna valutazione finora
- Gante Iris PPT Pe p006Documento20 pagineGante Iris PPT Pe p006Donna Ville GanteNessuna valutazione finora
- Basic Principles of Local GovernmentDocumento72 pagineBasic Principles of Local GovernmentAnne Camille SongNessuna valutazione finora
- Stories of Prophets - 2Documento19 pagineStories of Prophets - 2Hadis MusaNessuna valutazione finora
- Orientation Report PDFDocumento13 pagineOrientation Report PDFRiaz RasoolNessuna valutazione finora
- Desiderata: by Max EhrmannDocumento6 pagineDesiderata: by Max EhrmannTanay AshwathNessuna valutazione finora
- Induction Hardening - Interpretation of Drawing & Testing PDFDocumento4 pagineInduction Hardening - Interpretation of Drawing & Testing PDFrajesh DESHMUKHNessuna valutazione finora
- The Grey Nomads Guide To AustraliaDocumento3 pagineThe Grey Nomads Guide To AustraliaFreerangecamping60% (5)
- Dimensional Analysis Similarity Lesson2 Dimensional Parameters HandoutDocumento11 pagineDimensional Analysis Similarity Lesson2 Dimensional Parameters HandoutRizqi RamadhanNessuna valutazione finora
- CV1000 CV2000 CV3000 Ice Cube Machines SpecsDocumento12 pagineCV1000 CV2000 CV3000 Ice Cube Machines SpecsAriel Godoy100% (1)
- 37th APSDC Scientific PresentationsDocumento7 pagine37th APSDC Scientific PresentationsSatyendra KumarNessuna valutazione finora
- 2 Profile OMORIS - Presentation 2020-2Documento20 pagine2 Profile OMORIS - Presentation 2020-2lemuel bacsaNessuna valutazione finora
- Kundalini Meditation & The Vagus Nerve - Eleven Minute MedsDocumento5 pagineKundalini Meditation & The Vagus Nerve - Eleven Minute Medstimsmith1081574100% (5)
- Retired Car Jacker Screen PlayDocumento4 pagineRetired Car Jacker Screen Playapi-633948182Nessuna valutazione finora
- 2290 PDFDocumento222 pagine2290 PDFmittupatel190785Nessuna valutazione finora
- 4608 Eed 01Documento29 pagine4608 Eed 01NickNessuna valutazione finora
- Plow Moldboard or Disc PlowDocumento7 paginePlow Moldboard or Disc PlowAdewaleNessuna valutazione finora
- Hot Tub BrochureDocumento124 pagineHot Tub BrochureMai Tuan AnhNessuna valutazione finora