Potrebbero piacerti anche
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (120)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- Mind Maps PDFDocumento208 pagineMind Maps PDFAnonymous 9uu04elNessuna valutazione finora
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- English Reading Kit Level 1: Pupil's Assessment ManualDocumento15 pagineEnglish Reading Kit Level 1: Pupil's Assessment ManualGretylle Quicoy100% (1)
- Low Intermediate Korean Vocabulary and GrammarDocumento10 pagineLow Intermediate Korean Vocabulary and GrammarTuong Van Nguyen100% (3)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (73)
- Active Listening HANDOUT PDFDocumento26 pagineActive Listening HANDOUT PDFMiguel Cuevas DolotNessuna valutazione finora
- A Book of Beasts PDFDocumento32 pagineA Book of Beasts PDFbrad drac100% (2)
- Fouts Federal LawsuitDocumento28 pagineFouts Federal LawsuitWXYZ-TV DetroitNessuna valutazione finora
- Anesthesia Pocket Cards 7 18 18Documento6 pagineAnesthesia Pocket Cards 7 18 18Miguel Cuevas DolotNessuna valutazione finora
- History Taking ExaminationDocumento7 pagineHistory Taking ExaminationIndunil AnuruddhikaNessuna valutazione finora
- Castigliano's 2nd TheoremDocumento29 pagineCastigliano's 2nd TheoremMiddle East100% (4)
- Community-Acquired Pneumonia - CPG 2016Documento26 pagineCommunity-Acquired Pneumonia - CPG 2016Jamie SebastianNessuna valutazione finora
- Click Here For Download: (PDF) HerDocumento2 pagineClick Here For Download: (PDF) HerJerahm Flancia0% (1)
- The Saving Cross of The Suffering Christ: Benjamin R. WilsonDocumento228 pagineThe Saving Cross of The Suffering Christ: Benjamin R. WilsonTri YaniNessuna valutazione finora
- InvestMemo TemplateDocumento6 pagineInvestMemo TemplatealiranagNessuna valutazione finora
- Effectiveness of Transdermal MagnesiumDocumento2 pagineEffectiveness of Transdermal MagnesiumMiguel Cuevas Dolot100% (1)
- Covid 19 CPR 7 RulesDocumento21 pagineCovid 19 CPR 7 RulesMiguel Cuevas DolotNessuna valutazione finora
- How Can Patients Visitors Help - May18Documento2 pagineHow Can Patients Visitors Help - May18Miguel Cuevas DolotNessuna valutazione finora
- PSB 368Documento6 paginePSB 368Miguel Cuevas DolotNessuna valutazione finora
- Covid 19 CPR 7 RulesDocumento21 pagineCovid 19 CPR 7 RulesMiguel Cuevas DolotNessuna valutazione finora
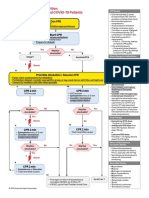
- ACLS Cardiac Arrest Algorithm For Suspected or Confirmed COVID-19 PatientsDocumento1 paginaACLS Cardiac Arrest Algorithm For Suspected or Confirmed COVID-19 PatientsMariuxi Tatiana ChocoNessuna valutazione finora
- (MED) COVID-19 Trans V. 2.0Documento6 pagine(MED) COVID-19 Trans V. 2.0Isabel VinasNessuna valutazione finora
- Covid 19 PDFDocumento18 pagineCovid 19 PDFMiguel Cuevas DolotNessuna valutazione finora
- Physical Examination in ENT: Ussana Promyothin, MDDocumento60 paginePhysical Examination in ENT: Ussana Promyothin, MDMiguel Cuevas DolotNessuna valutazione finora
- Clinical Examination of The Ear, Nose and Throat: Dave Pothier ST Mary's 2003Documento30 pagineClinical Examination of The Ear, Nose and Throat: Dave Pothier ST Mary's 2003Ekambaram TrmNessuna valutazione finora
- Physical Examination in ENT: Ussana Promyothin, MDDocumento60 paginePhysical Examination in ENT: Ussana Promyothin, MDMiguel Cuevas DolotNessuna valutazione finora
- Physical Assessment: Ear, Nose, Mouth, and ThroatDocumento59 paginePhysical Assessment: Ear, Nose, Mouth, and ThroatMiguel Cuevas DolotNessuna valutazione finora
- Vertigo Gail Ishiyama 1 13 10Documento40 pagineVertigo Gail Ishiyama 1 13 10Myname Rama LienNessuna valutazione finora
- Pedia Tickler Update 2017Documento2 paginePedia Tickler Update 2017Tani BokNessuna valutazione finora
- Cook Book (Filipino) 13 PDFDocumento23 pagineCook Book (Filipino) 13 PDFAdina AnghelNessuna valutazione finora
- Drug IndexDocumento2 pagineDrug IndexMiguel Cuevas DolotNessuna valutazione finora
- Nocturnals Physiology 2018Documento14 pagineNocturnals Physiology 2018Miguel Cuevas DolotNessuna valutazione finora
- Benign Paroxysmal Positional Vertigo: Waseem WatadDocumento37 pagineBenign Paroxysmal Positional Vertigo: Waseem WatadnoviNessuna valutazione finora
- A Case-Control Study of The Association of Diet and Obesity With Gout in Taiwan PDFDocumento12 pagineA Case-Control Study of The Association of Diet and Obesity With Gout in Taiwan PDFMiguel Cuevas DolotNessuna valutazione finora
- A Case-Control Study of The Association of Diet and Obesity With Gout in Taiwan PDFDocumento12 pagineA Case-Control Study of The Association of Diet and Obesity With Gout in Taiwan PDFMiguel Cuevas DolotNessuna valutazione finora
- Clinical AbstractDocumento4 pagineClinical AbstractMiguel Cuevas DolotNessuna valutazione finora
- TCVS - Cardiac Surgery Part 2 Dr. de AsisDocumento8 pagineTCVS - Cardiac Surgery Part 2 Dr. de AsisMiguel Cuevas DolotNessuna valutazione finora
- Neurologic ExamDocumento1 paginaNeurologic ExamMiguel Cuevas DolotNessuna valutazione finora
- HEMAreviewDocumento3 pagineHEMAreviewMiguel Cuevas DolotNessuna valutazione finora
- Kerosene PDFDocumento31 pagineKerosene PDFRudyMLanaNessuna valutazione finora
- SunEdison Pancho Perez Complaint As FiledDocumento47 pagineSunEdison Pancho Perez Complaint As FiledLizHoffmanNessuna valutazione finora
- 1.3 Digital Communication and AnalogueDocumento6 pagine1.3 Digital Communication and AnaloguenvjnjNessuna valutazione finora
- Iver Brevik, Olesya Gorbunova and Diego Saez-Gomez - Casimir Effects Near The Big Rip Singularity in Viscous CosmologyDocumento7 pagineIver Brevik, Olesya Gorbunova and Diego Saez-Gomez - Casimir Effects Near The Big Rip Singularity in Viscous CosmologyDex30KMNessuna valutazione finora
- Knut - Fleur de LisDocumento10 pagineKnut - Fleur de LisoierulNessuna valutazione finora
- Yield of Concrete - tcm45-341215 PDFDocumento3 pagineYield of Concrete - tcm45-341215 PDFBijaya RaulaNessuna valutazione finora
- Info Cad Engb FestoDocumento14 pagineInfo Cad Engb FestoBayu RahmansyahNessuna valutazione finora
- Oral Communication in Context Quarter 2: Week 1 Module in Communicative Strategies 1Documento10 pagineOral Communication in Context Quarter 2: Week 1 Module in Communicative Strategies 1Agatha Sigrid GonzalesNessuna valutazione finora
- Speakout Language BankDocumento7 pagineSpeakout Language BankСаша БулуєвNessuna valutazione finora
- The Trials of The Rizal Bill (Gist)Documento2 pagineThe Trials of The Rizal Bill (Gist)CJ IbaleNessuna valutazione finora
- Correct Translation of 2-16Documento19 pagineCorrect Translation of 2-16muhammad_zubair708110Nessuna valutazione finora
- مذكرة التأسيس الرائعة لغة انجليزية للمبتدئين?Documento21 pagineمذكرة التأسيس الرائعة لغة انجليزية للمبتدئين?Manar SwaidanNessuna valutazione finora
- Second Unit Test 2022: Radha Madhav Public School BareillyDocumento4 pagineSecond Unit Test 2022: Radha Madhav Public School BareillyRaghav AgarwalNessuna valutazione finora
- Description of Medical Specialties Residents With High Levels of Workplace Harassment Psychological Terror in A Reference HospitalDocumento16 pagineDescription of Medical Specialties Residents With High Levels of Workplace Harassment Psychological Terror in A Reference HospitalVictor EnriquezNessuna valutazione finora
- Sales Purchases Returns Day BookDocumento8 pagineSales Purchases Returns Day BookAung Zaw HtweNessuna valutazione finora
- Akhbar Al Fuqaha Narration - Non Raful Yadayn From Ibn Umar - Reply To Zubair Ali ZaiDocumento15 pagineAkhbar Al Fuqaha Narration - Non Raful Yadayn From Ibn Umar - Reply To Zubair Ali ZaiAbdullah YusufNessuna valutazione finora
- Sec 25 HmaDocumento3 pagineSec 25 HmaMukul BajajNessuna valutazione finora
- Physical Education 10 WEEK 2Documento10 paginePhysical Education 10 WEEK 2Israel MarquezNessuna valutazione finora
- History RizalDocumento6 pagineHistory RizalIrvin LevieNessuna valutazione finora
- An Aging Game Simulation Activity For Al PDFDocumento13 pagineAn Aging Game Simulation Activity For Al PDFramzan aliNessuna valutazione finora
- Shipping Operation Diagram: 120' (EVERY 30')Documento10 pagineShipping Operation Diagram: 120' (EVERY 30')Hafid AriNessuna valutazione finora
- Merger of Bank of Karad Ltd. (BOK) With Bank of India (BOI)Documento17 pagineMerger of Bank of Karad Ltd. (BOK) With Bank of India (BOI)Alexander DeckerNessuna valutazione finora