Potrebbero piacerti anche
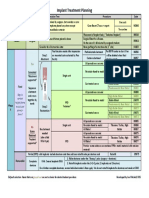
- Implant TX Plan GridDocumento1 paginaImplant TX Plan GridAhmed BadrNessuna valutazione finora
- Guided Bone Regeneration ProcedureDocumento16 pagineGuided Bone Regeneration ProcedureAymen Elatrash100% (4)
- ENDODONTIC PreclinicBookDocumento9 pagineENDODONTIC PreclinicBookhunarsandhuNessuna valutazione finora
- 8 - Clinical Outcome in Periradicular Surgery Effect of Patient - and Tooth-Related Factors - A Multicenter StudyDocumento8 pagine8 - Clinical Outcome in Periradicular Surgery Effect of Patient - and Tooth-Related Factors - A Multicenter StudykochikaghochiNessuna valutazione finora
- Jung 2018Documento11 pagineJung 2018Sebastien MelloulNessuna valutazione finora
- DIAGNOSTIC METHODS (Emphasis On Recent Advances) IN EndodonticsDocumento51 pagineDIAGNOSTIC METHODS (Emphasis On Recent Advances) IN EndodonticsKalpesh DeyNessuna valutazione finora
- Endodontic Topics Volume 31 Issue 1 2014 (Doi 10.1111/etp.12066) Baba, Nadim Z. Goodacre, Charles J. - Restoration of Endodontically Treated Teeth - Contemporary Concepts andDocumento16 pagineEndodontic Topics Volume 31 Issue 1 2014 (Doi 10.1111/etp.12066) Baba, Nadim Z. Goodacre, Charles J. - Restoration of Endodontically Treated Teeth - Contemporary Concepts andardeleanoana100% (1)
- 1.GIT All DisordersDocumento240 pagine1.GIT All DisordersCabdisacid yasinNessuna valutazione finora
- Regenerative Endodontics Study GuideDocumento21 pagineRegenerative Endodontics Study GuideKristineNessuna valutazione finora
- Atypically Grown Large Periradicular Cyst Affecting Adjacent Teeth and Leading To Confounding Diagnosis of Non-Endodontic PathologyDocumento10 pagineAtypically Grown Large Periradicular Cyst Affecting Adjacent Teeth and Leading To Confounding Diagnosis of Non-Endodontic PathologyJorge OrbeNessuna valutazione finora
- Implant Maintenance - A Clinical UpdateDocumento9 pagineImplant Maintenance - A Clinical UpdateDr. Minkle GulatiNessuna valutazione finora
- Implant Course.Documento76 pagineImplant Course.mustafaNessuna valutazione finora
- IB - Acids and Bases Practice QuestionsDocumento12 pagineIB - Acids and Bases Practice QuestionshunarsandhuNessuna valutazione finora
- Administration of Coagulation-Altering Therapy in The Patient Presenting For Oral Health and Maxillofacial SurgeryDocumento18 pagineAdministration of Coagulation-Altering Therapy in The Patient Presenting For Oral Health and Maxillofacial SurgeryLaura Giraldo QuinteroNessuna valutazione finora
- Dentistry EmergenciesDocumento5 pagineDentistry EmergenciesSofia PereiraNessuna valutazione finora
- A New Classification Scheme For Periodontal and Peri-Implant Diseases and Conditions - Introduction and Key Changes From The 1999 ClassificationDocumento8 pagineA New Classification Scheme For Periodontal and Peri-Implant Diseases and Conditions - Introduction and Key Changes From The 1999 Classificationvaleria Gonzalez BalloteNessuna valutazione finora
- RPD ManualDocumento108 pagineRPD ManualMahesa Vaza100% (4)
- Advancement of GTR Membrane For Dental ApplicationsDocumento21 pagineAdvancement of GTR Membrane For Dental ApplicationsNawshad MuhammadNessuna valutazione finora
- IB Topic 10: Organic Chemistry Practice QuestionsDocumento36 pagineIB Topic 10: Organic Chemistry Practice Questionshunarsandhu50% (2)
- Diagnosis and Management of Odontogenic InfectionsDocumento52 pagineDiagnosis and Management of Odontogenic InfectionsAhmed EmadNessuna valutazione finora
- Periodontal Surgery Biological WidthDocumento7 paginePeriodontal Surgery Biological WidthhunarsandhuNessuna valutazione finora
- Interpretation Basics of Cone Beam Computed TomographyDa EverandInterpretation Basics of Cone Beam Computed TomographyValutazione: 4 su 5 stelle4/5 (1)
- Root Resorption Diagnosis, Classification and Treatment Choices Based On Stimulation FactorsDocumento8 pagineRoot Resorption Diagnosis, Classification and Treatment Choices Based On Stimulation FactorsAhmad AssariNessuna valutazione finora
- The Etiology of Hard and Soft Tissue Deformities at Dental ImplantsDocumento13 pagineThe Etiology of Hard and Soft Tissue Deformities at Dental ImplantsCam Tran NguyenNessuna valutazione finora
- Ridge AugmentationDocumento109 pagineRidge AugmentationSingh Jyoti100% (3)
- Berglundh Et Al-2018-Journal of Clinical PeriodontologyDocumento6 pagineBerglundh Et Al-2018-Journal of Clinical PeriodontologyCristian CulcitchiNessuna valutazione finora
- Endo-Perio Lesions Diagnosis and InterdisciplinaryDocumento5 pagineEndo-Perio Lesions Diagnosis and InterdisciplinaryGabriela ArgeseanuNessuna valutazione finora
- Types of Needles Used in The Irrigation of Root CanalDocumento8 pagineTypes of Needles Used in The Irrigation of Root Canalhunarsandhu100% (1)
- Peri Implant Disease PDFDocumento32 paginePeri Implant Disease PDFHajra FarooqNessuna valutazione finora
- Treatment Concept Periodontal Surgery enDocumento11 pagineTreatment Concept Periodontal Surgery enMark Jason MinaNessuna valutazione finora
- Rationale of Endodontic TreatmentDocumento30 pagineRationale of Endodontic Treatmentaakriti100% (1)
- Inflammation and Oral Cancer: From Bench to BedsideDa EverandInflammation and Oral Cancer: From Bench to BedsideHiroyuki TomitaNessuna valutazione finora
- Nano-Antimicrobials in EndodonticsDocumento14 pagineNano-Antimicrobials in EndodonticsIJAR JOURNALNessuna valutazione finora
- Clinical Outcomes of Vertical Bone Augmentation To Enable Dental Implant Placement: A Systematic ReviewDocumento13 pagineClinical Outcomes of Vertical Bone Augmentation To Enable Dental Implant Placement: A Systematic Reviewvanessa_werbickyNessuna valutazione finora
- Innate ImmunityDocumento43 pagineInnate ImmunityhunarsandhuNessuna valutazione finora
- Implant-Related Complications and FailuresDocumento91 pagineImplant-Related Complications and FailuresSaman MohammadzadehNessuna valutazione finora
- Endodontic NotesDocumento44 pagineEndodontic Noteshunarsandhu100% (1)
- JIAP July 2011 - Guided Tissue Regeneration - A Decision-Making ModelDocumento8 pagineJIAP July 2011 - Guided Tissue Regeneration - A Decision-Making ModelLouis HutahaeanNessuna valutazione finora
- PHA2022 Unit GuideDocumento30 paginePHA2022 Unit GuidehunarsandhuNessuna valutazione finora
- Endodontic MicrobiologyDocumento9 pagineEndodontic MicrobiologySarah KahilNessuna valutazione finora
- CHAP 10 Dental Calculus SelfDocumento38 pagineCHAP 10 Dental Calculus SelfarshmeentariqNessuna valutazione finora
- Epidemiology of Periodontal DiseasesDocumento14 pagineEpidemiology of Periodontal DiseasesFrancisca DinamarcaNessuna valutazione finora
- Periodontal Literature ReviewDocumento70 paginePeriodontal Literature ReviewSmitha Kapani gowdaNessuna valutazione finora
- Irrigation in EndodonticsDocumento5 pagineIrrigation in EndodonticshunarsandhuNessuna valutazione finora
- Intracanal MedicamentDocumento11 pagineIntracanal MedicamentAsh PeiNessuna valutazione finora
- Regenerative Dentistry::: Meera NairDocumento55 pagineRegenerative Dentistry::: Meera NairArickta100% (1)
- The Key To Profound Local Anesthesia: NeuroanatomyDocumento8 pagineThe Key To Profound Local Anesthesia: NeuroanatomyRavik FidayatikaNessuna valutazione finora
- Complication of Dentoalveolar SurgeryDocumento21 pagineComplication of Dentoalveolar Surgerywhussien7376Nessuna valutazione finora
- The Socket-Shield Technique To Support The Buccofacial Tissues at Immediate Implant Placement PDFDocumento7 pagineThe Socket-Shield Technique To Support The Buccofacial Tissues at Immediate Implant Placement PDFAhmed Mohammed Saaduddin SapriNessuna valutazione finora
- 3-Access Cavity Preparation PDFDocumento60 pagine3-Access Cavity Preparation PDFAllisyia MalauNessuna valutazione finora
- Tooth Discolour at Ion PedoDocumento28 pagineTooth Discolour at Ion PedoFourthMolar.comNessuna valutazione finora
- Splinting Journal PDFDocumento7 pagineSplinting Journal PDFhanataniarNessuna valutazione finora
- Catherine A. Hebert, D.D.S .: Internal Vs External ResorptionDocumento2 pagineCatherine A. Hebert, D.D.S .: Internal Vs External ResorptionJames OnealNessuna valutazione finora
- Stem Cells in Periodontal RegenerationDocumento10 pagineStem Cells in Periodontal RegenerationInternational Organization of Scientific Research (IOSR)Nessuna valutazione finora
- Alveolar Exostosis - Revisited A Narrative Review of The LiteratureDocumento6 pagineAlveolar Exostosis - Revisited A Narrative Review of The Literatureغمدان دماج الحمزيNessuna valutazione finora
- Endodontic and Restorative Management of A Lower Molar With A Calcified Pulp Chamber.Documento7 pagineEndodontic and Restorative Management of A Lower Molar With A Calcified Pulp Chamber.Nicolas SantanderNessuna valutazione finora
- Perio 2000 VOL-76 Treatment of Pathologic Peri-Implant Pocket PDFDocumento11 paginePerio 2000 VOL-76 Treatment of Pathologic Peri-Implant Pocket PDFchandanaNessuna valutazione finora
- Basic Surgical Principles With ITI ImplantsDocumento10 pagineBasic Surgical Principles With ITI ImplantsEliza DN100% (1)
- Facial SpaceDocumento19 pagineFacial SpacePreetam PatnalaNessuna valutazione finora
- ANTI-PLAQUE-anticalculus AgentsDocumento99 pagineANTI-PLAQUE-anticalculus Agentst sNessuna valutazione finora
- JISPPD Supplement 19 PDFDocumento71 pagineJISPPD Supplement 19 PDFmadhu kakanurNessuna valutazione finora
- 10 1016@j Joen 2020 04 007Documento9 pagine10 1016@j Joen 2020 04 007rasagna reddyNessuna valutazione finora
- Apical Seal Versus Coronal SealDocumento8 pagineApical Seal Versus Coronal SealSalem RawashdahNessuna valutazione finora
- Management of Peri-Implant Mucositis and Peri-Implantitis PDFDocumento19 pagineManagement of Peri-Implant Mucositis and Peri-Implantitis PDFgirl33Nessuna valutazione finora
- List of Infectious Diseases Covered by EPI (Expanded Program of ImmunizationDocumento13 pagineList of Infectious Diseases Covered by EPI (Expanded Program of ImmunizationPalwasha KhanNessuna valutazione finora
- HalitosisDocumento6 pagineHalitosispratyusha vallamNessuna valutazione finora
- Library DissertationDocumento201 pagineLibrary Dissertationhaneefmdf100% (2)
- Complication of ExodontiaDocumento54 pagineComplication of ExodontiaHudh HudNessuna valutazione finora
- Periodontal Therapy in Older AdultsDocumento15 paginePeriodontal Therapy in Older AdultsPathivada Lumbini100% (1)
- Headches and Facial PainDocumento33 pagineHeadches and Facial PainIsak ShatikaNessuna valutazione finora
- 10 1016@j Joen 2020 01 023Documento23 pagine10 1016@j Joen 2020 01 023Jorge OrbeNessuna valutazione finora
- NazilaApplications of Nanotechnology in Endodontic - A ReviewDocumento6 pagineNazilaApplications of Nanotechnology in Endodontic - A ReviewElsa Di GiuseppeNessuna valutazione finora
- Nonsurgical Periodontal Therapy DCNADocumento12 pagineNonsurgical Periodontal Therapy DCNAdhwanit31Nessuna valutazione finora
- Lecture 5 Laser in Operative DentistryDocumento7 pagineLecture 5 Laser in Operative DentistryDt omarNessuna valutazione finora
- Week 7 Histology Physiology of Dental Pulp MiriamDocumento4 pagineWeek 7 Histology Physiology of Dental Pulp MiriamDelaney IslipNessuna valutazione finora
- Methadone Treatment in VictoriaDocumento34 pagineMethadone Treatment in VictoriahunarsandhuNessuna valutazione finora
- Decision Tree For Oral Mucosal Lesion PDFDocumento1 paginaDecision Tree For Oral Mucosal Lesion PDFcreature123100% (1)
- Med HX Dental RelevanceDocumento4 pagineMed HX Dental RelevancehunarsandhuNessuna valutazione finora
- Endodontics and Fixed Prosthodontics Past Exam QuestionsDocumento6 pagineEndodontics and Fixed Prosthodontics Past Exam QuestionshunarsandhuNessuna valutazione finora
- The Role of Fissure Sealants in Caries PreventionDocumento29 pagineThe Role of Fissure Sealants in Caries PreventionhunarsandhuNessuna valutazione finora
- Adaptive Immune Response in PeriodontitisDocumento39 pagineAdaptive Immune Response in PeriodontitishunarsandhuNessuna valutazione finora
- Staging and Grading Template For PeriodontitisDocumento1 paginaStaging and Grading Template For PeriodontitishunarsandhuNessuna valutazione finora
- Endodontic Flare UpsDocumento6 pagineEndodontic Flare UpshunarsandhuNessuna valutazione finora
- Oral Manifestations of SyphilisDocumento7 pagineOral Manifestations of SyphilishunarsandhuNessuna valutazione finora
- Oral Viral Infections Diagnosis and ManagementDocumento13 pagineOral Viral Infections Diagnosis and ManagementhunarsandhuNessuna valutazione finora
- Root Canal Irrigation - A Mini ReviewDocumento4 pagineRoot Canal Irrigation - A Mini ReviewhunarsandhuNessuna valutazione finora
- Irrigation Technique Used in Cleaning and ShapingDocumento6 pagineIrrigation Technique Used in Cleaning and ShapinghunarsandhuNessuna valutazione finora
- Infectious Diseases of Oral CavityDocumento21 pagineInfectious Diseases of Oral CavityhunarsandhuNessuna valutazione finora
- BMS2052 Unit GuideDocumento21 pagineBMS2052 Unit GuidehunarsandhuNessuna valutazione finora
- Antimicrobial Lecture NotesDocumento55 pagineAntimicrobial Lecture Noteshunarsandhu100% (2)
- Understanding The Stresses and Strains of Being A DoctorDocumento4 pagineUnderstanding The Stresses and Strains of Being A DoctorhunarsandhuNessuna valutazione finora
- Genetics Workbook UpdateDocumento36 pagineGenetics Workbook UpdateLauren WinnettNessuna valutazione finora
- BMS2062 Unit GuideDocumento37 pagineBMS2062 Unit Guidehunarsandhu100% (1)
- Defining Resilience - IB Psychology High Level - Options - Developmental PsychologyDocumento1 paginaDefining Resilience - IB Psychology High Level - Options - Developmental PsychologyhunarsandhuNessuna valutazione finora
- Periosteal Pocket Flap Technique. A Comparative StudyDocumento10 paginePeriosteal Pocket Flap Technique. A Comparative StudyosiglesiNessuna valutazione finora
- (22857079 - Acta Medica Transilvanica) Management and Prevention of Complications of Guided Bone RegenerationDocumento3 pagine(22857079 - Acta Medica Transilvanica) Management and Prevention of Complications of Guided Bone RegenerationGabriela ArgeseanuNessuna valutazione finora
- Current Concepts in Alveolar Ridge AugmentationDocumento12 pagineCurrent Concepts in Alveolar Ridge AugmentationAthenaeum Scientific PublishersNessuna valutazione finora
- (E-Catalog) COLLA - EN - CompressedDocumento6 pagine(E-Catalog) COLLA - EN - CompressedAyush MalhotraNessuna valutazione finora
- Wafer TechniquesDocumento10 pagineWafer TechniquesCeeta IndustriesNessuna valutazione finora
- Supervivencia Dental A Largo Plazo Después Del Tratamiento Regenerativo de Defectos IntraóseosDocumento7 pagineSupervivencia Dental A Largo Plazo Después Del Tratamiento Regenerativo de Defectos IntraóseosAgustin BuryakNessuna valutazione finora
- Bonegraftingforimplant Surgery: Ladi Doonquah,, Pierre-John Holmes,, Laxman Kumar Ranganathan,, Hughette RobertsonDocumento19 pagineBonegraftingforimplant Surgery: Ladi Doonquah,, Pierre-John Holmes,, Laxman Kumar Ranganathan,, Hughette RobertsonJason LeeNessuna valutazione finora
- Perio 2000 ArticlesDocumento21 paginePerio 2000 ArticlesDrRahat SaleemNessuna valutazione finora
- Periodontics: Which Statement Regarding An Autogenous Free Gingival Graft Is True? Select All That ApplyDocumento2.018 paginePeriodontics: Which Statement Regarding An Autogenous Free Gingival Graft Is True? Select All That ApplymariaNessuna valutazione finora
- Evaluation of Mineralized Plasmatic Matrix During Sinus Lift With The Simultaneous Placement of Dental ImplantsDocumento10 pagineEvaluation of Mineralized Plasmatic Matrix During Sinus Lift With The Simultaneous Placement of Dental ImplantsIJAR JOURNALNessuna valutazione finora
- The Modified Papilla Preservation-1Documento6 pagineThe Modified Papilla Preservation-1Razvan SalageanNessuna valutazione finora
- Manual For Preventive Dentistry I-Ii & Clinical Periodontics I - IiDocumento77 pagineManual For Preventive Dentistry I-Ii & Clinical Periodontics I - IiSalma MentariNessuna valutazione finora
- Lingual Orthodontics and Forced Eruption: A Means For Osseous and Tissue Regeneration. Case ReportDocumento12 pagineLingual Orthodontics and Forced Eruption: A Means For Osseous and Tissue Regeneration. Case ReportqoutNessuna valutazione finora
- Clasificacion Horizontal Del Reborde - FlattenedDocumento28 pagineClasificacion Horizontal Del Reborde - FlattenedJuan Carlos Montañez BenavidesNessuna valutazione finora
- 96 IJPRD CTG Vs GTRDocumento9 pagine96 IJPRD CTG Vs GTRinamboy7Nessuna valutazione finora
- Regenerative Periodontal Therapy: PeriodontologyDocumento8 pagineRegenerative Periodontal Therapy: PeriodontologyEmilian ChiperNessuna valutazione finora
- Regeneración Periodontal de Defectos Infraóseos HumanosDocumento7 pagineRegeneración Periodontal de Defectos Infraóseos HumanosAgustin BuryakNessuna valutazione finora
- Tooth Out Whats Next ENDocumento69 pagineTooth Out Whats Next ENAdela Pérez MeyerNessuna valutazione finora
- 7 Shreeprada Dash IJPHRDDecember 2018 IssueDocumento7 pagine7 Shreeprada Dash IJPHRDDecember 2018 IssueSahana RangarajanNessuna valutazione finora
- Aggressive Periodontitis: By: Dr. Mahendra Kumar Singh Pgiindyear Department of Periodontia GDCHDocumento54 pagineAggressive Periodontitis: By: Dr. Mahendra Kumar Singh Pgiindyear Department of Periodontia GDCHDrMahendra SagarNessuna valutazione finora
- Essential Techniques of Alveolar Bone Augmentation in Implant Dentistry A Surgical Manual 2Nd Edition Len Tolstunov Full ChapterDocumento68 pagineEssential Techniques of Alveolar Bone Augmentation in Implant Dentistry A Surgical Manual 2Nd Edition Len Tolstunov Full Chapterrichard.rathbone385100% (5)
- Non KeratinocytesDocumento21 pagineNon KeratinocytesAbi AbiramithangamNessuna valutazione finora
- Company and Soft Tissue Regeneration ProductsDocumento51 pagineCompany and Soft Tissue Regeneration ProductsPaulus LagadanNessuna valutazione finora