Potrebbero piacerti anche
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5795)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1091)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (345)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (74)
- Crypts of Kelemvor 5eDocumento15 pagineCrypts of Kelemvor 5eΜιχάλης ΤερζάκηςNessuna valutazione finora
- Reference BookletDocumento35 pagineReference BookletΜιχάλης Τερζάκης57% (7)
- Exc Cat #17 320 CuDocumento2 pagineExc Cat #17 320 CuWashington Santamaria100% (4)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- Shop Manual PC78MR-6-SEBM030601 PDFDocumento592 pagineShop Manual PC78MR-6-SEBM030601 PDFBudi Waskito95% (20)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- Old-School Essentials Adventure Anthology 1 v0-4Documento44 pagineOld-School Essentials Adventure Anthology 1 v0-4Μιχάλης Τερζάκης20% (5)
- Case 4 Sakhalin 1 ProjectDocumento29 pagineCase 4 Sakhalin 1 ProjectashmitNessuna valutazione finora
- ITIL Cobit MappingDocumento16 pagineITIL Cobit Mappingapi-383689667% (3)
- Frangible Roof To Shell JointDocumento1 paginaFrangible Roof To Shell JointSAGARNessuna valutazione finora
- Stonehell Dungeon, Lost Level (LL)Documento8 pagineStonehell Dungeon, Lost Level (LL)Μιχάλης ΤερζάκηςNessuna valutazione finora
- The Isle of Forgotten Gods (Basic, BX)Documento38 pagineThe Isle of Forgotten Gods (Basic, BX)Μιχάλης Τερζάκης100% (1)
- Recruitment (Robotic) Process Automation (RPA)Documento6 pagineRecruitment (Robotic) Process Automation (RPA)Anuja BhakuniNessuna valutazione finora
- Dolmenwood Hex Crawl ProcedureDocumento2 pagineDolmenwood Hex Crawl ProcedureΜιχάλης Τερζάκης100% (2)
- Old-School Essentials Adventure Anthology 2 v0-3Documento38 pagineOld-School Essentials Adventure Anthology 2 v0-3Μιχάλης Τερζάκης0% (2)
- OSE The Pelietic ChurchDocumento3 pagineOSE The Pelietic ChurchΜιχάλης ΤερζάκηςNessuna valutazione finora
- Tangled (Pages) (OSE)Documento24 pagineTangled (Pages) (OSE)Μιχάλης Τερζάκης50% (8)
- Dolmenwood House Rules (NGP) (Basic, BX)Documento1 paginaDolmenwood House Rules (NGP) (Basic, BX)Μιχάλης Τερζάκης0% (1)
- Key Performance IndicatorsDocumento72 pagineKey Performance Indicatorstamhieu75% (4)
- ENIRAM - Guide To Dynamic Trim Optimization 280611 PDFDocumento14 pagineENIRAM - Guide To Dynamic Trim Optimization 280611 PDFPhineas MagellanNessuna valutazione finora
- OSE Random Gear - FUNNEL GEARDocumento1 paginaOSE Random Gear - FUNNEL GEARΜιχάλης ΤερζάκηςNessuna valutazione finora
- Illmire Pre-Gen CharDocumento7 pagineIllmire Pre-Gen CharΜιχάλης ΤερζάκηςNessuna valutazione finora
- GE Lighting Systems Indoor Lighting Designers Guide 1970Documento56 pagineGE Lighting Systems Indoor Lighting Designers Guide 1970Alan Masters100% (1)
- The Dolmenwood CalendarDocumento22 pagineThe Dolmenwood CalendarΜιχάλης Τερζάκης100% (1)
- T Series TorqueDocumento8 pagineT Series TorqueBrian OctavianusNessuna valutazione finora
- Social Epidimiology - HistoryDocumento7 pagineSocial Epidimiology - HistoryΜιχάλης ΤερζάκηςNessuna valutazione finora
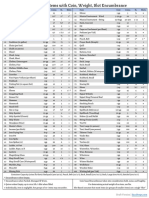
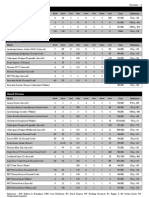
- Item Cost Coins Lb. Slots Item Cost Coins Lb. Slots: Draft VersionDocumento1 paginaItem Cost Coins Lb. Slots Item Cost Coins Lb. Slots: Draft VersionΜιχάλης ΤερζάκηςNessuna valutazione finora
- Gauld Et Al WHR 2008 PHC Policy How Wide Is The Gap Between Agenta and Implementation 12 High IncomeDocumento21 pagineGauld Et Al WHR 2008 PHC Policy How Wide Is The Gap Between Agenta and Implementation 12 High IncomeΜιχάλης ΤερζάκηςNessuna valutazione finora
- Origins of PHC and SPHCDocumento11 pagineOrigins of PHC and SPHCΜιχάλης ΤερζάκηςNessuna valutazione finora
- Difference SPHC Vs CPHCDocumento9 pagineDifference SPHC Vs CPHCΜιχάλης ΤερζάκηςNessuna valutazione finora
- Hikvision Fever Screening Thermal CameraDocumento1 paginaHikvision Fever Screening Thermal CameraΜιχάλης ΤερζάκηςNessuna valutazione finora
- DRA12 - The Barber of Silverymoon PDFDocumento13 pagineDRA12 - The Barber of Silverymoon PDFlordejulioNessuna valutazione finora
- REC-551-POC-Quiz - 2Documento1 paginaREC-551-POC-Quiz - 2Jinendra JainNessuna valutazione finora
- The Masterbuilder - July 2013 - Concrete SpecialDocumento286 pagineThe Masterbuilder - July 2013 - Concrete SpecialChaitanya Raj GoyalNessuna valutazione finora
- Woolridge - Reasnoning About Rational AgentsDocumento232 pagineWoolridge - Reasnoning About Rational AgentsAlejandro Vázquez del MercadoNessuna valutazione finora
- CNC Macine Dimesions-ModelDocumento1 paginaCNC Macine Dimesions-ModelNaveen PrabhuNessuna valutazione finora
- DUROFLEX2020 LimpiadorDocumento8 pagineDUROFLEX2020 LimpiadorSolid works ArgentinaNessuna valutazione finora
- Content - EJ 2014 Galvanised GratesDocumento32 pagineContent - EJ 2014 Galvanised GratesFilip StojkovskiNessuna valutazione finora
- Introduction To Web TechnologiesDocumento8 pagineIntroduction To Web TechnologiesManeela SiriNessuna valutazione finora
- Passenger Terminal Building ProposalDocumento6 paginePassenger Terminal Building ProposalHimawan Aryo DewantoroNessuna valutazione finora
- Lab 2 WorksheetDocumento3 pagineLab 2 WorksheetPohuyistNessuna valutazione finora
- Accreditation Grading Metrics - Skills Ecosystem Guidelines10 - 04Documento8 pagineAccreditation Grading Metrics - Skills Ecosystem Guidelines10 - 04Jagdish RajanNessuna valutazione finora
- Brosur All New Innova MUVs 16393Documento7 pagineBrosur All New Innova MUVs 16393Roni SetyawanNessuna valutazione finora
- Skiold Trough Augers: SkioldgroupDocumento2 pagineSkiold Trough Augers: SkioldgroupLuis NunesNessuna valutazione finora
- 4.1 Introduction To Studying Two Factors: ESGC 6112: Lecture 4 Two-Factor Cross-Classification DesignsDocumento14 pagine4.1 Introduction To Studying Two Factors: ESGC 6112: Lecture 4 Two-Factor Cross-Classification DesignsragunatharaoNessuna valutazione finora
- Pengumuman Matakuliah Pilihan 2110 - KMGDocumento85 paginePengumuman Matakuliah Pilihan 2110 - KMGMartha Wulan TumangkengNessuna valutazione finora
- SR5 TOOL Equipment, Drones (Buyable), Compiled ListDocumento3 pagineSR5 TOOL Equipment, Drones (Buyable), Compiled ListBeki LokaNessuna valutazione finora
- Oil and DrillingDocumento3 pagineOil and DrillingAmri YogiNessuna valutazione finora
- Bomb Oil AisinDocumento38 pagineBomb Oil AisinMAURICIONessuna valutazione finora
- 12jun27 FC Perfect Stores Add Zing To HUL's Sales Growth - tcm114 289918 PDFDocumento1 pagina12jun27 FC Perfect Stores Add Zing To HUL's Sales Growth - tcm114 289918 PDFSantosh SinghNessuna valutazione finora
- Guide To Creating and Editing Metadata in Arcgis For Publishing To The Msdis GeoportalDocumento24 pagineGuide To Creating and Editing Metadata in Arcgis For Publishing To The Msdis Geoportalvela.letaNessuna valutazione finora
- TCH Assignment Success Rate (%)Documento7 pagineTCH Assignment Success Rate (%)AbebeNessuna valutazione finora