Potrebbero piacerti anche
- Diabetes DrugsDocumento1 paginaDiabetes Drugsmed testNessuna valutazione finora
- Bacterial VaginosisDocumento12 pagineBacterial VaginosisAudioBhaskara TitalessyNessuna valutazione finora
- Local Anesthetics - Blockers K+ Channel Blockers Ca2+ Channel BlockersDocumento4 pagineLocal Anesthetics - Blockers K+ Channel Blockers Ca2+ Channel Blockersmed testNessuna valutazione finora
- Sphere: These DiarrheaDocumento3 pagineSphere: These Diarrheamed testNessuna valutazione finora
- Infectious Disease Naplex QuestionsDocumento3 pagineInfectious Disease Naplex QuestionsSARANYA0% (1)
- Pharmacology Drug Chart: Drug Name Receptor Therapeutic Uses Adverse EffectsDocumento18 paginePharmacology Drug Chart: Drug Name Receptor Therapeutic Uses Adverse EffectsPadmavathy Naidu Chokkapu100% (2)
- Antibiotics Cheat SheetDocumento2 pagineAntibiotics Cheat SheetAlejandro Rodas Salinas100% (1)
- List of Medical MnemonicsDocumento47 pagineList of Medical MnemonicsSUBHADIPNessuna valutazione finora
- BMC PediaDocumento4 pagineBMC PediaRenette Uy100% (1)
- Cardiovascular Drug IntroductionDocumento3 pagineCardiovascular Drug IntroductionSamah Khan100% (1)
- NSAIDS and SteroidsDocumento2 pagineNSAIDS and Steroidsmed testNessuna valutazione finora
- Endocrine Drug ChartDocumento1 paginaEndocrine Drug ChartJessicaNessuna valutazione finora
- Updated Antibiotic Chart - 2016 PDFDocumento2 pagineUpdated Antibiotic Chart - 2016 PDFmugenzi eric100% (1)
- Pharmacology SummaryDocumento16 paginePharmacology Summaryshenric16Nessuna valutazione finora
- Pharm-Drugs ChartsDocumento21 paginePharm-Drugs ChartsCandace Flowers100% (3)
- Comprehensive Nclex Notes Easy To Read PDFDocumento97 pagineComprehensive Nclex Notes Easy To Read PDFKenia GeorgesNessuna valutazione finora
- ACLS Simulation ScenariosDocumento14 pagineACLS Simulation ScenariosVanessa HermioneNessuna valutazione finora
- Medical MnemonicsDocumento107 pagineMedical MnemonicsdrabuelaNessuna valutazione finora
- Test InformationDocumento5 pagineTest InformationCatalina BorquezNessuna valutazione finora
- BED12 - Antibiotics PharmacologyDocumento2 pagineBED12 - Antibiotics PharmacologyAmir AmirulNessuna valutazione finora
- Drug Mechanism Clincal Use Side Effects Antifungal: Amphote Ricin BDocumento30 pagineDrug Mechanism Clincal Use Side Effects Antifungal: Amphote Ricin BCess Lagera Ybanez0% (1)
- IV Solutions CheatsheetDocumento1 paginaIV Solutions CheatsheetRosemaryCastroNessuna valutazione finora
- A Simple Guide to Hypovolemia, Diagnosis, Treatment and Related ConditionsDa EverandA Simple Guide to Hypovolemia, Diagnosis, Treatment and Related ConditionsNessuna valutazione finora
- Diabetes Mellitus Drug ChartDocumento3 pagineDiabetes Mellitus Drug Chartlui.stephanie1751100% (1)
- Bumetanide Torsemide: Desmopressin - V2Documento1 paginaBumetanide Torsemide: Desmopressin - V2med testNessuna valutazione finora
- Nursing Fluids and ElectrolytesDocumento14 pagineNursing Fluids and Electrolytesaga1028100% (18)
- Pharm Calcium Channel Blockers (Bahar&Amy) "Vera Dialed The Calcium Channel To Buy A Knife" Verapramil, Diltizaem, NifedipineDocumento7 paginePharm Calcium Channel Blockers (Bahar&Amy) "Vera Dialed The Calcium Channel To Buy A Knife" Verapramil, Diltizaem, Nifedipinecherrybombaz100% (4)
- Antibiotc Made Easy PDFDocumento12 pagineAntibiotc Made Easy PDFAmjad_2020100% (1)
- Anti Infective Drug ChartDocumento1 paginaAnti Infective Drug ChartJessica100% (1)
- Pharmacology MapsDocumento18 paginePharmacology MapsPERUBATAN Cawangan Zagazig100% (1)
- (HGT X 18.18) 140 Units 20Documento3 pagine(HGT X 18.18) 140 Units 20Jorelyn FriasNessuna valutazione finora
- Critical Care Drug Reference SheetDocumento12 pagineCritical Care Drug Reference SheetYanina CoxNessuna valutazione finora
- Pediatric Notes Draft 12 1Documento98 paginePediatric Notes Draft 12 1Aljon S. TemploNessuna valutazione finora
- Pharmacology-ATI 150 Drug Cards PDFDocumento4 paginePharmacology-ATI 150 Drug Cards PDFhollyNessuna valutazione finora
- Nclex Testing TipsDocumento28 pagineNclex Testing Tipsnkuligowski100% (2)
- 100 Essential Drugs1Documento8 pagine100 Essential Drugs1Sudip DevadasNessuna valutazione finora
- Med-Surg HESI Study GuideDocumento13 pagineMed-Surg HESI Study GuideTravis Hargett93% (14)
- Drugclasses Pharmacologypart 1 PDFDocumento25 pagineDrugclasses Pharmacologypart 1 PDFSutanya100% (2)
- Utmc - Utoledo.edu Depts Nursing Pdfs Basic EKG RefresherDocumento210 pagineUtmc - Utoledo.edu Depts Nursing Pdfs Basic EKG RefresherTrish HồNessuna valutazione finora
- ClarithromycinDocumento4 pagineClarithromycinNoi Maya Anggrita SariNessuna valutazione finora
- A.1. Community-Acquired: Use Antibiotics JudiciouslyDocumento33 pagineA.1. Community-Acquired: Use Antibiotics JudiciouslymaxgroovesNessuna valutazione finora
- ShockDocumento5 pagineShocknkuligowski100% (2)
- Medication Preparation Dosage Remarks: Antipyretic/AnalgesicDocumento4 pagineMedication Preparation Dosage Remarks: Antipyretic/AnalgesicTIFFANIE CHRISTEL UYNessuna valutazione finora
- Drug Study I MetronidazoleDocumento2 pagineDrug Study I MetronidazoleKimberly Ann Aquino50% (2)
- PHARMACOLOGY Anti Microbial DrugsDocumento17 paginePHARMACOLOGY Anti Microbial DrugsLeilani Sablan100% (2)
- Pediatric Meds List1Documento38 paginePediatric Meds List1Arman Carl DulayNessuna valutazione finora
- Pelvic Inflammatory DiseaseDocumento9 paginePelvic Inflammatory DiseaseSohanInduwaraGamage100% (2)
- Post-Partum Review Questions - Handout 2 With Answers /rationalesDocumento9 paginePost-Partum Review Questions - Handout 2 With Answers /rationalesnkuligowski100% (2)
- I. Inspection: Cardiovascular ExamDocumento136 pagineI. Inspection: Cardiovascular ExamMarbella39Nessuna valutazione finora
- Drug Names - Stems, Prefixes, Roots and Suffixes - NCLEX MasteryDocumento5 pagineDrug Names - Stems, Prefixes, Roots and Suffixes - NCLEX MasteryMarcel YoungNessuna valutazione finora
- Refrigerate: Hives, RashDocumento5 pagineRefrigerate: Hives, RashstarobinNessuna valutazione finora
- Drug Classification TemplateDocumento1 paginaDrug Classification Templatehovismj100% (1)
- Complete Drug GuideDocumento225 pagineComplete Drug GuideJessica 'Baker' IsaacsNessuna valutazione finora
- Template Drug Card1Documento1 paginaTemplate Drug Card1Kay TaylorNessuna valutazione finora
- Agents Causing Coma or SeizuresDocumento3 pagineAgents Causing Coma or SeizuresShaira Aquino VerzosaNessuna valutazione finora
- Post Assessment PediatricsDocumento4 paginePost Assessment Pediatricscuicuita100% (4)
- Ace Inhibitors MnemonicDocumento1 paginaAce Inhibitors MnemonicGirish Waru0% (2)
- Ninja - Anemias PDFDocumento1 paginaNinja - Anemias PDFErica Hyeyeon LeeNessuna valutazione finora
- Lile Bai 1: Area/Site Common Organism Useful Abx Other NotesDocumento3 pagineLile Bai 1: Area/Site Common Organism Useful Abx Other NotesNicole BerryNessuna valutazione finora
- Acid Base DisordersDocumento5 pagineAcid Base DisordersMillenial VoiceNessuna valutazione finora
- Pharmacology Questions CardiacDocumento5 paginePharmacology Questions CardiacAmanda SimpsonNessuna valutazione finora
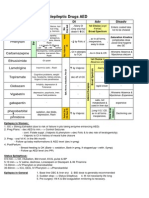
- Antiepileptic Drugs AED: D' DI Disadv SE AdvDocumento1 paginaAntiepileptic Drugs AED: D' DI Disadv SE Advrayooona88Nessuna valutazione finora
- Hmg-Coa Reductase Inhibitors (Statins) : Side Effects, Contraindications, InteractionsDocumento6 pagineHmg-Coa Reductase Inhibitors (Statins) : Side Effects, Contraindications, Interactionswaste78Nessuna valutazione finora
- Cholinergic Drugs - TablesDocumento7 pagineCholinergic Drugs - TablesThuan Tăng NguyenNessuna valutazione finora
- Drugs WorksheetDocumento16 pagineDrugs Worksheetninja-2001Nessuna valutazione finora
- Antibiotic Table BucherJones 2013 UpdateDocumento8 pagineAntibiotic Table BucherJones 2013 UpdatenamanNessuna valutazione finora
- Austin Pets Alive Cat Medication Chart 52F6Documento6 pagineAustin Pets Alive Cat Medication Chart 52F6Shakira FerreiraNessuna valutazione finora
- Med MissionDocumento3 pagineMed MissionNicole CabahugNessuna valutazione finora
- PedoDocumento2 paginePedoHenyo AkoNessuna valutazione finora
- Abd DX and TX PlansDocumento23 pagineAbd DX and TX PlansnkuligowskiNessuna valutazione finora
- Combined Hormone Pill, Patch, Ring Progestin Only Mini Pill, Depo-Provera, IUDDocumento1 paginaCombined Hormone Pill, Patch, Ring Progestin Only Mini Pill, Depo-Provera, IUDnkuligowskiNessuna valutazione finora
- HivDocumento5 pagineHivnkuligowskiNessuna valutazione finora
- EyeDocumento86 pagineEyenkuligowskiNessuna valutazione finora
- Start A Method Today.: Choosing A Method: What Matters Most To Me?Documento1 paginaStart A Method Today.: Choosing A Method: What Matters Most To Me?nkuligowskiNessuna valutazione finora
- NURP423 Exam 1Documento45 pagineNURP423 Exam 1nkuligowskiNessuna valutazione finora
- Critical CareDocumento40 pagineCritical Carenkuligowski100% (6)
- Lecture # 2Documento7 pagineLecture # 2nkuligowskiNessuna valutazione finora
- Lecture#1 01-14-14 Why Is Nursing of Children Different?Documento12 pagineLecture#1 01-14-14 Why Is Nursing of Children Different?nkuligowskiNessuna valutazione finora
- All CancersDocumento22 pagineAll Cancersnkuligowski100% (2)
- Lecture # 3Documento21 pagineLecture # 3nkuligowskiNessuna valutazione finora
- DevelopmentDocumento4 pagineDevelopmentnkuligowski100% (2)
- OBGYN 3a - NewbornDocumento2 pagineOBGYN 3a - NewbornnkuligowskiNessuna valutazione finora
- HESI BLUE BOOK Pg. 182 Developmental MilestonesDocumento8 pagineHESI BLUE BOOK Pg. 182 Developmental Milestonesnkuligowski0% (1)
- 2013 NCLEX Candidate BulletinDocumento20 pagine2013 NCLEX Candidate BulletinnkuligowskiNessuna valutazione finora
- Intro ABG and ElectrolytesDocumento6 pagineIntro ABG and ElectrolytesnkuligowskiNessuna valutazione finora
- Review Notes in Infection Control - NCLEXDocumento1 paginaReview Notes in Infection Control - NCLEXwyndz100% (10)
- OBGYN 3 - NewbornDocumento6 pagineOBGYN 3 - NewbornnkuligowskiNessuna valutazione finora
- OBGYN 4 - PostpartumDocumento9 pagineOBGYN 4 - PostpartumnkuligowskiNessuna valutazione finora
- Magnesium and CalciumDocumento50 pagineMagnesium and CalciumnkuligowskiNessuna valutazione finora
- Fundamental Keypoint Chapter 7Documento1 paginaFundamental Keypoint Chapter 7nkuligowskiNessuna valutazione finora
- Acid Base 1Documento22 pagineAcid Base 1nkuligowskiNessuna valutazione finora
- Acid Base Imbalance 2Documento29 pagineAcid Base Imbalance 2nkuligowskiNessuna valutazione finora
- Fundamental Keypoint Chapter 6Documento1 paginaFundamental Keypoint Chapter 6nkuligowskiNessuna valutazione finora
- 3.2. QuantificationDocumento80 pagine3.2. QuantificationBrhanu belayNessuna valutazione finora
- Entamoeba HistolyticaDocumento5 pagineEntamoeba HistolyticaiqraNessuna valutazione finora
- Antibiotic Prophylaxis: Francis Neil C. CaranayDocumento11 pagineAntibiotic Prophylaxis: Francis Neil C. CaranayNdor BariboloNessuna valutazione finora
- Nur 1210 Pedia Concept Module 4B Alterations With Infectious, Inflammatory and Immunologic ResponseDocumento19 pagineNur 1210 Pedia Concept Module 4B Alterations With Infectious, Inflammatory and Immunologic ResponseweissNessuna valutazione finora
- Vaginitis EmedicineDocumento17 pagineVaginitis EmedicineIndah HaneNessuna valutazione finora
- Management of Intra-Abdominal InfectionDocumento65 pagineManagement of Intra-Abdominal InfectionKamran SherazNessuna valutazione finora
- Pentazine, Phenazine, Phencen,, Phenoject-50, Prometh, Prorex, Prothazine, V-GanDocumento34 paginePentazine, Phenazine, Phencen,, Phenoject-50, Prometh, Prorex, Prothazine, V-GankotonashiNessuna valutazione finora
- Genital Tract InfectionDocumento52 pagineGenital Tract InfectionRahma Putri50% (2)
- Journal ReadingDocumento21 pagineJournal ReadingMelvita KurniawanNessuna valutazione finora
- Drug Therapeutic Record TemplateDocumento1 paginaDrug Therapeutic Record TemplateAubrey Justine GaleonNessuna valutazione finora
- Update On Antimicrobial Therapy in Management of Acute Odontogenic Infection in Oral and Maxillofacial SurgeryDocumento9 pagineUpdate On Antimicrobial Therapy in Management of Acute Odontogenic Infection in Oral and Maxillofacial SurgeryMARISOL GALLEGO DUQUENessuna valutazione finora
- Trichomonas VaginalisDocumento2 pagineTrichomonas Vaginalistutan_santosNessuna valutazione finora
- Drugs Commonly Used in TVCCDocumento20 pagineDrugs Commonly Used in TVCCAjinkya JadhaoNessuna valutazione finora
- Drugs PGNTDocumento7 pagineDrugs PGNTJoanna Marie Datahan EstomoNessuna valutazione finora
- Placenta PreviaDocumento87 paginePlacenta PreviaKaye Cueto100% (1)
- AntibiotikDocumento10 pagineAntibiotikGeubrina FitrianandaNessuna valutazione finora
- AcyclovirDocumento20 pagineAcyclovirBrian Enrile Dorado0% (1)
- NCP DIarrheaDocumento8 pagineNCP DIarrheakamini ChoudharyNessuna valutazione finora
- B11Ph02 AntihelmenticsDocumento6 pagineB11Ph02 AntihelmenticsDonnaBells Hermo LabaniegoNessuna valutazione finora
- Guidelines For Office Gynecology in JapanDocumento17 pagineGuidelines For Office Gynecology in JapanKatherine ZevallosNessuna valutazione finora
- STI Treatment Guidelines 2012 PDFDocumento8 pagineSTI Treatment Guidelines 2012 PDFPaolo Castelblanco VelandiaNessuna valutazione finora
- Fire Belly ToadsDocumento12 pagineFire Belly ToadsAmy Thomas StanislawskiNessuna valutazione finora
- Drug Study CholeDocumento5 pagineDrug Study CholejpmlodiNessuna valutazione finora