Potrebbero piacerti anche
- The Little Book of The Little Book ofDocumento38 pagineThe Little Book of The Little Book ofHani Gowai80% (5)
- Rating Scale for Auditory HallucinationsDocumento9 pagineRating Scale for Auditory HallucinationsYuli HdyNessuna valutazione finora
- Cognitive Processing Therapy (CPT) For Post Traumatic Stress DisorderDocumento11 pagineCognitive Processing Therapy (CPT) For Post Traumatic Stress DisorderDaniel R. Gaita, MA, LMSWNessuna valutazione finora
- Trauma in the Lives of Children: Crisis and Stress Management Techniques for Counselors, Teachers, and Other ProfessionalsDa EverandTrauma in the Lives of Children: Crisis and Stress Management Techniques for Counselors, Teachers, and Other ProfessionalsNessuna valutazione finora
- APA - DSM 5 Depression Bereavement Exclusion PDFDocumento2 pagineAPA - DSM 5 Depression Bereavement Exclusion PDFDaniel NgNessuna valutazione finora
- Connecting Paradigms: A Trauma Informed & Neurobiological Framework for Motivational Interviewing ImplementationDa EverandConnecting Paradigms: A Trauma Informed & Neurobiological Framework for Motivational Interviewing ImplementationNessuna valutazione finora
- Compendium Version 2Documento136 pagineCompendium Version 2J100% (1)
- Adverse Childhood Experiences StudyDocumento9 pagineAdverse Childhood Experiences Studytheplatinumlife7364Nessuna valutazione finora
- Fact Sheet Assignment On DyslexiaDocumento2 pagineFact Sheet Assignment On DyslexiaMBCass100% (1)
- Myers Briggs TestDocumento13 pagineMyers Briggs TestRaluca Roxana MărgineanNessuna valutazione finora
- Dissociative Amnesia: Epidemiology, Pathogenesis, Clinical Manifestations, Course, and DiagnosisDocumento26 pagineDissociative Amnesia: Epidemiology, Pathogenesis, Clinical Manifestations, Course, and DiagnosisZiggy GonNessuna valutazione finora
- Childhood Trauma and Maladaptive DaydreamingDocumento16 pagineChildhood Trauma and Maladaptive DaydreamingRose DarugarNessuna valutazione finora
- Amistoso - DMDDDocumento25 pagineAmistoso - DMDDAndréAmistosoNessuna valutazione finora
- Psychiatric Disorders: An Overview of Major Conditions and TreatmentsDocumento14 paginePsychiatric Disorders: An Overview of Major Conditions and Treatmentsrpascua123100% (1)
- The Adverse Childhood Experiences (ACE) StudyDocumento14 pagineThe Adverse Childhood Experiences (ACE) Studyalongtheheavens100% (5)
- ACE - Adverse Childhood ExperiencesDocumento7 pagineACE - Adverse Childhood ExperiencesMário JorgeNessuna valutazione finora
- Psychiatry: DementiaDocumento3 paginePsychiatry: DementiaSok-Moi Chok100% (2)
- ADHD Symptoms in Healthy Adults Are Associated With Stressful Life Events and Negative Memory BiasDocumento10 pagineADHD Symptoms in Healthy Adults Are Associated With Stressful Life Events and Negative Memory BiasRaúl Añari100% (1)
- DSM 5 TR What's NewDocumento2 pagineDSM 5 TR What's NewRafael Gaede Carrillo100% (1)
- Self Concept in Children and Adolescents With ADHDDocumento32 pagineSelf Concept in Children and Adolescents With ADHDpsihopedcarmenNessuna valutazione finora
- RWJF: Adverse Childhood Experiences InfographicDocumento1 paginaRWJF: Adverse Childhood Experiences InfographicforumonenergyNessuna valutazione finora
- More Than Just Words and Numbers:: The Top 15 Fundamental Changes To The Dsm-5 & The Transition To Icd-10Documento107 pagineMore Than Just Words and Numbers:: The Top 15 Fundamental Changes To The Dsm-5 & The Transition To Icd-10Hilma Harry'sNessuna valutazione finora
- Mullen Polksys ArticleDocumento6 pagineMullen Polksys Articleapi-249796934Nessuna valutazione finora
- DSM 5 Adhd Fact SheetDocumento2 pagineDSM 5 Adhd Fact SheetMario MendozaNessuna valutazione finora
- Global Assessment FunctioningDocumento8 pagineGlobal Assessment Functioningapi-260339450Nessuna valutazione finora
- Shared Psychotic Disorder - NCBIDocumento8 pagineShared Psychotic Disorder - NCBI5KevNessuna valutazione finora
- Assure Readers That I Am Strongly Pro-Meditation For The Traumatized and Non-Traumatized Alike. As A Long-TermDocumento12 pagineAssure Readers That I Am Strongly Pro-Meditation For The Traumatized and Non-Traumatized Alike. As A Long-TermIgnat SorinaNessuna valutazione finora
- School Refusal: Children Who Can't or Won't Go to SchoolDa EverandSchool Refusal: Children Who Can't or Won't Go to SchoolNessuna valutazione finora
- Suicide Risk Assessment Summary.08Documento1 paginaSuicide Risk Assessment Summary.08Pintiliciuc-aga MihaiNessuna valutazione finora
- Disability Handbook - FinalDocumento44 pagineDisability Handbook - Finalapi-544907296Nessuna valutazione finora
- TF-CBT and Complex TraumaDocumento14 pagineTF-CBT and Complex TraumaDaniel Hidalgo LimaNessuna valutazione finora
- Co-Occurring DisordersDocumento91 pagineCo-Occurring DisordersEmilyNessuna valutazione finora
- Summary of The Body Keeps the Score: Brain, Mind, and Body in the Healing of Trauma by Bessel van der Kolk MD (Fireside Reads)Da EverandSummary of The Body Keeps the Score: Brain, Mind, and Body in the Healing of Trauma by Bessel van der Kolk MD (Fireside Reads)Nessuna valutazione finora
- Biological Psychiatry's Decline and FallDocumento2 pagineBiological Psychiatry's Decline and FallEnrique Martinez100% (1)
- PPDGJ 3 PDFDocumento279 paginePPDGJ 3 PDFtri ummiNessuna valutazione finora
- Neurodevelopmental Psychiatry - An Introduction For Medical StudentsDocumento68 pagineNeurodevelopmental Psychiatry - An Introduction For Medical StudentsNiranjana MahalingamNessuna valutazione finora
- Insomnia and Fatigue after Traumatic Brain Injury: A CBT Approach to Assessment and TreatmentDa EverandInsomnia and Fatigue after Traumatic Brain Injury: A CBT Approach to Assessment and TreatmentValutazione: 5 su 5 stelle5/5 (1)
- History of DepressionDocumento7 pagineHistory of Depressionklysmanu93Nessuna valutazione finora
- The Child Bipolar QuestionnaireDocumento10 pagineThe Child Bipolar QuestionnairefranciscatomiNessuna valutazione finora
- DSM 5 - DSM 5Documento7 pagineDSM 5 - DSM 5Roxana ClsNessuna valutazione finora
- ACE Study Congressional Briefing Anda PDFDocumento31 pagineACE Study Congressional Briefing Anda PDFUnited Way of East Central Iowa100% (3)
- Post-Traumatic Stress Disorder: A Guide for Primary Care Clinicians and TherapistsDa EverandPost-Traumatic Stress Disorder: A Guide for Primary Care Clinicians and TherapistsNessuna valutazione finora
- Exposure Therapy Training Strategies Jad PDFDocumento7 pagineExposure Therapy Training Strategies Jad PDFFarhang WarzshyNessuna valutazione finora
- How The Special Needs Brain Learns,: Chapter-By-Chapter Study Guide ForDocumento2 pagineHow The Special Needs Brain Learns,: Chapter-By-Chapter Study Guide ForElizabeth Clarissa Palar - NainggolanNessuna valutazione finora
- The Little Handbook of Understanding Panic and Anxiety DisorderDa EverandThe Little Handbook of Understanding Panic and Anxiety DisorderNessuna valutazione finora
- Index: SR No. ParticularsDocumento10 pagineIndex: SR No. Particularstarang1994Nessuna valutazione finora
- Biosketch Sample Forms DDocumento3 pagineBiosketch Sample Forms DLindsayNessuna valutazione finora
- A Dissociative Survival Mechanism: Traumatic AmnesiaDocumento23 pagineA Dissociative Survival Mechanism: Traumatic AmnesiaJanaína RNessuna valutazione finora
- Decisions and Consequences: The Realities of Being a ManDa EverandDecisions and Consequences: The Realities of Being a ManNessuna valutazione finora
- First Aid Tips for Depression: Overcoming Depression In 4 Simple StepsDa EverandFirst Aid Tips for Depression: Overcoming Depression In 4 Simple StepsNessuna valutazione finora
- Primary and Secundary DepersonalizationDocumento8 paginePrimary and Secundary DepersonalizationRobert WilliamsNessuna valutazione finora
- Ross Green - Advanced Explosive Child - Options For Handing ProblemsDocumento9 pagineRoss Green - Advanced Explosive Child - Options For Handing ProblemsTed IndykNessuna valutazione finora
- A Mind That Found Itself An AutobiographyDa EverandA Mind That Found Itself An AutobiographyValutazione: 5 su 5 stelle5/5 (1)
- Out of the Silence: My Journey into Post-Traumatic Stress Disorder and BackDa EverandOut of the Silence: My Journey into Post-Traumatic Stress Disorder and BackNessuna valutazione finora
- Adhd Resource Pt1Documento23 pagineAdhd Resource Pt1drpameladhNessuna valutazione finora
- CBT For ChildrenDocumento10 pagineCBT For ChildrenGabriella RiosNessuna valutazione finora
- Norman Bates-Assessment and DiagnosisDocumento16 pagineNorman Bates-Assessment and DiagnosisDiana-Luisa AvramNessuna valutazione finora
- Amines and SchizophreniaDa EverandAmines and SchizophreniaHarold E. HimwichNessuna valutazione finora
- OCD in Children and Adolescents: Causes, Symptoms, and TreatmentsDocumento10 pagineOCD in Children and Adolescents: Causes, Symptoms, and TreatmentsFaris Aziz PridiantoNessuna valutazione finora
- The Violent Person at Work: The Ultimate Guide to Identifying Dangerous PersonsDa EverandThe Violent Person at Work: The Ultimate Guide to Identifying Dangerous PersonsNessuna valutazione finora
- Tobacco Harm Reduction 2010Documento304 pagineTobacco Harm Reduction 2010Billy HadjisNessuna valutazione finora
- Trauma FocusedCognitive BehavioralTherapy (TF CBT)Documento2 pagineTrauma FocusedCognitive BehavioralTherapy (TF CBT)Joel RamosNessuna valutazione finora
- Norme Istallaz. Serie DLX 03-04Documento1 paginaNorme Istallaz. Serie DLX 03-04sjsshipNessuna valutazione finora
- D48877F DEIF Control PanelDocumento1 paginaD48877F DEIF Control PanelsjsshipNessuna valutazione finora
- Boiler Low Level Control Electrical DrawingDocumento1 paginaBoiler Low Level Control Electrical DrawingsjsshipNessuna valutazione finora
- D48877F DEIF Control PanelDocumento1 paginaD48877F DEIF Control PanelsjsshipNessuna valutazione finora
- Ratio Exam QuestionsDocumento2 pagineRatio Exam QuestionssjsshipNessuna valutazione finora
- Egg 1Documento2 pagineEgg 1sjsshipNessuna valutazione finora
- Egg 3Documento3 pagineEgg 3sjsshipNessuna valutazione finora
- Easter Egg SearchDocumento1 paginaEaster Egg SearchsjsshipNessuna valutazione finora
- 1000 Ideas About Easter Riddles On Pinterest Scavenger HuntDocumento1 pagina1000 Ideas About Easter Riddles On Pinterest Scavenger HuntsjsshipNessuna valutazione finora
- LEWIS Backhoe Range for Tractors 15-60HP</TITLEDocumento8 pagineLEWIS Backhoe Range for Tractors 15-60HP</TITLEsjsshipNessuna valutazione finora
- 1000 Ideas About Easter Riddles On Pinterest Scavenger HuntDocumento1 pagina1000 Ideas About Easter Riddles On Pinterest Scavenger HuntsjsshipNessuna valutazione finora
- Egg Hunt Clue Map with 17 Hiding PlacesDocumento2 pagineEgg Hunt Clue Map with 17 Hiding PlacessjsshipNessuna valutazione finora
- MOSS-Vessel GH SpecificationDocumento3 pagineMOSS-Vessel GH SpecificationsjsshipNessuna valutazione finora
- 164 Service Sheet6 PDFDocumento4 pagine164 Service Sheet6 PDFsjsshipNessuna valutazione finora
- 164 Service Sheet6 PDFDocumento4 pagine164 Service Sheet6 PDFsjsshipNessuna valutazione finora
- 164 Service Sheet5 PDFDocumento4 pagine164 Service Sheet5 PDFsjsshipNessuna valutazione finora
- R134A Temperature Pressure Chart for Evaporator and CondenserDocumento5 pagineR134A Temperature Pressure Chart for Evaporator and CondensersjsshipNessuna valutazione finora
- UT-Vessel GH SpecificationDocumento3 pagineUT-Vessel GH SpecificationsjsshipNessuna valutazione finora
- 164 Service Sheet6 PDFDocumento4 pagine164 Service Sheet6 PDFsjsshipNessuna valutazione finora
- 164 Service Sheet5 PDFDocumento4 pagine164 Service Sheet5 PDFsjsshipNessuna valutazione finora
- 164 Service Sheet4 PDFDocumento4 pagine164 Service Sheet4 PDFsjsshipNessuna valutazione finora
- 164 Service Sheet TesterDocumento4 pagine164 Service Sheet TesterJill WilsonNessuna valutazione finora
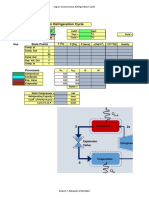
- Vapor Compression Refrigeration Cycle: State PointsDocumento6 pagineVapor Compression Refrigeration Cycle: State PointssjsshipNessuna valutazione finora
- 164 Service Sheet4 PDFDocumento4 pagine164 Service Sheet4 PDFsjsshipNessuna valutazione finora
- 164 Service Sheet5 PDFDocumento4 pagine164 Service Sheet5 PDFsjsshipNessuna valutazione finora
- 164 Service Sheet TesterDocumento4 pagine164 Service Sheet TesterJill WilsonNessuna valutazione finora
- 164 Service Sheet TesterDocumento4 pagine164 Service Sheet TesterJill WilsonNessuna valutazione finora
- Recharge FeonDocumento8 pagineRecharge FeonsjsshipNessuna valutazione finora
- Frequently Asked Questions: " (Type Subject of Faqs) " Rulefinder User GuideDocumento1 paginaFrequently Asked Questions: " (Type Subject of Faqs) " Rulefinder User GuidesjsshipNessuna valutazione finora
- Hiller Plant InstructableDocumento5 pagineHiller Plant InstructablesjsshipNessuna valutazione finora
- DTSCH Arztebl Int-114-0121Documento9 pagineDTSCH Arztebl Int-114-0121Aqsa KadiriNessuna valutazione finora
- Laertes Diagnosed WithDocumento10 pagineLaertes Diagnosed Withapi-356693509Nessuna valutazione finora
- ConfabulationDocumento3 pagineConfabulationapi-311966893Nessuna valutazione finora
- Psykolog Complicated Grief Therapy (CGT) - A Novel Third Wave CBT For ProDocumento3 paginePsykolog Complicated Grief Therapy (CGT) - A Novel Third Wave CBT For ProRob KorényiNessuna valutazione finora
- Fields of PsychologyDocumento3 pagineFields of PsychologyTayyibaNessuna valutazione finora
- IAFNR Newsletter October 2018Documento24 pagineIAFNR Newsletter October 2018Tela KayneNessuna valutazione finora
- Neurospa - Manual 2016 - 220829 - 202650Documento8 pagineNeurospa - Manual 2016 - 220829 - 202650Liza HaeberleNessuna valutazione finora
- 2112 2021 NT - Practice Test No12Documento9 pagine2112 2021 NT - Practice Test No12Hà LinhhNessuna valutazione finora
- Psilocybin and MDMA Prove Their Psychotherapeutic MettleDocumento1 paginaPsilocybin and MDMA Prove Their Psychotherapeutic MettleKarlus ProNessuna valutazione finora
- Realistic Thinking FormDocumento2 pagineRealistic Thinking FormjefrirezaNessuna valutazione finora
- Dwnload Full Psychiatric Mental Health Nursing 5th Edition Fortinash Test Bank PDFDocumento35 pagineDwnload Full Psychiatric Mental Health Nursing 5th Edition Fortinash Test Bank PDFchilyransei100% (10)
- Bad Trip Due To Anticholinergic Effect of CannabisDocumento2 pagineBad Trip Due To Anticholinergic Effect of CannabisRobert DinuNessuna valutazione finora
- 2020 NGSC Mission Team 18 MagazineDocumento10 pagine2020 NGSC Mission Team 18 MagazineIbu OluyiNessuna valutazione finora
- Glover - The Therapeutic Effect of Inexact InterpretationDocumento16 pagineGlover - The Therapeutic Effect of Inexact InterpretationHugo Tannous JorgeNessuna valutazione finora
- Effects of Mental Health For Student LearningDocumento20 pagineEffects of Mental Health For Student Learningclara dupitasNessuna valutazione finora
- Vermont Psychiatric Care HospitalDocumento15 pagineVermont Psychiatric Care HospitalEsayase AsnakeNessuna valutazione finora
- Overcoming agoraphobia: A self-help manualDocumento41 pagineOvercoming agoraphobia: A self-help manualvasilikiserNessuna valutazione finora
- Safari - 05-May-2020 at 03:13 PDFDocumento1 paginaSafari - 05-May-2020 at 03:13 PDFvkbasavaNessuna valutazione finora
- Narcolepsy As A Psychogenic Symptom : Leo Angelo Spiegel, M.D., and C. P. Oberndo F, M.DDocumento8 pagineNarcolepsy As A Psychogenic Symptom : Leo Angelo Spiegel, M.D., and C. P. Oberndo F, M.DariscesNessuna valutazione finora
- The P FactorDocumento29 pagineThe P FactorAndrea PuimeNessuna valutazione finora
- Diagnosing Mental IllnessDocumento3 pagineDiagnosing Mental IllnessRuva Oscass JimmyNessuna valutazione finora
- DIAGNOSIS OF HYSTERIA (Eliot Slater)Documento5 pagineDIAGNOSIS OF HYSTERIA (Eliot Slater)Francisco OrellanaNessuna valutazione finora
- Parenting and Family Adjustment Among Parents 14-20 PDFDocumento7 pagineParenting and Family Adjustment Among Parents 14-20 PDFIndian Journal of Psychiatric Social WorkNessuna valutazione finora
- Anxiety Research Paper 10Documento10 pagineAnxiety Research Paper 10api-582860150Nessuna valutazione finora
- How Depression Changes Your BrainDocumento4 pagineHow Depression Changes Your BrainMatoula SerefaNessuna valutazione finora
- Research Proposal DRAFT - Ver2Documento31 pagineResearch Proposal DRAFT - Ver2sahil4INDNessuna valutazione finora