Potrebbero piacerti anche
- Nursing Care Plan of The MotherDocumento20 pagineNursing Care Plan of The Motherbuang2390% (382)
- Start Where You Are A Journal For Self Exploration PDFDocumento1 paginaStart Where You Are A Journal For Self Exploration PDFNyemwerai Muterere22% (9)
- Polyhydramnios CASE STUDYDocumento17 paginePolyhydramnios CASE STUDYamit86% (37)
- Cambridge Igcse Literature in English Teacher S Resource CD Rom Cambridge Education Cambridge U Samples PDFDocumento14 pagineCambridge Igcse Literature in English Teacher S Resource CD Rom Cambridge Education Cambridge U Samples PDFMorshedHumayunNessuna valutazione finora
- GASTROSCHISISDocumento4 pagineGASTROSCHISISVin Custodio100% (1)
- IntussusceptionDocumento2 pagineIntussusceptionkentkriziaNessuna valutazione finora
- Midwifery and Obsterical Nursing PDFDocumento24 pagineMidwifery and Obsterical Nursing PDFSudipta Kumar BeraNessuna valutazione finora
- Fiber Optic Color ChartDocumento1 paginaFiber Optic Color Charttohamy2009100% (2)
- Sri Nikunja-Keli-VirudavaliDocumento12 pagineSri Nikunja-Keli-VirudavaliIronChavesNessuna valutazione finora
- AtresiaDocumento5 pagineAtresiakirtiNessuna valutazione finora
- A Tracheoesophageal FistulaDocumento11 pagineA Tracheoesophageal FistulaaparnaprasadmNessuna valutazione finora
- Congenital AnomaliesDocumento10 pagineCongenital Anomaliesربيع ضياء ربيعNessuna valutazione finora
- Esophageal Atresia and Tracheoesophageal Fistula: A Guide For ParentsDocumento4 pagineEsophageal Atresia and Tracheoesophageal Fistula: A Guide For ParentsMaya Asharie HarahapNessuna valutazione finora
- BaldwinDocumento6 pagineBaldwinalexafarrenNessuna valutazione finora
- Esophageal AtresiaDocumento21 pagineEsophageal AtresiaOktania Putri Kusnawan100% (2)
- Esophageal AtresiaDocumento9 pagineEsophageal AtresiaAnonymous 9xHTwHYNessuna valutazione finora
- Esophageal AtresiaDocumento3 pagineEsophageal AtresiaTiti AfriantoNessuna valutazione finora
- Tracheoesophageal Atresia: Mrs - Smitha.M Associate Professor Vijaya College of Nursing KottarakkaraDocumento10 pagineTracheoesophageal Atresia: Mrs - Smitha.M Associate Professor Vijaya College of Nursing KottarakkarakrishnasreeNessuna valutazione finora
- Congenital Anomalies of The Esophagus PDFDocumento3 pagineCongenital Anomalies of The Esophagus PDFSpecialName100% (1)
- 19-Pediatric SurgeryDocumento39 pagine19-Pediatric Surgerycallisto3487Nessuna valutazione finora
- Gastric DisordersDocumento135 pagineGastric DisordersEsmareldah Henry SirueNessuna valutazione finora
- Bishaw Assigment of GI DisorderDocumento98 pagineBishaw Assigment of GI DisorderRas Siko SafoNessuna valutazione finora
- Anorectal MalformationDocumento29 pagineAnorectal Malformationbimaindra97Nessuna valutazione finora
- Esophageal FistulaDocumento3 pagineEsophageal FistulaD Dimpy ThakurNessuna valutazione finora
- Surgery - Pediatric GIT, Abdominal Wall, Neoplasms - 2014ADocumento14 pagineSurgery - Pediatric GIT, Abdominal Wall, Neoplasms - 2014ATwinkle SalongaNessuna valutazione finora
- Common Pediatric Surgery ProblemsDocumento141 pagineCommon Pediatric Surgery Problemssedaka26100% (4)
- Gastrointestinal Disorders: Saint Louis UniversityDocumento5 pagineGastrointestinal Disorders: Saint Louis UniversityAle SandraNessuna valutazione finora
- PEDI 2. Embryologic Basis of GI Malformations 2021Documento54 paginePEDI 2. Embryologic Basis of GI Malformations 2021Hayle MaryamNessuna valutazione finora
- OmphaloceleDocumento23 pagineOmphaloceleFred PupeNessuna valutazione finora
- Intestinal Atresia and StenosisDocumento7 pagineIntestinal Atresia and StenosisMichael NafarinNessuna valutazione finora
- Choanal AtresiaDocumento32 pagineChoanal AtresiaGreeshma ShajiNessuna valutazione finora
- Esophagus Atresia: Dwi Rezki Amalia Medical Faculty of Lambung Mangkurat UniversityDocumento26 pagineEsophagus Atresia: Dwi Rezki Amalia Medical Faculty of Lambung Mangkurat UniversityDwi Rezky AmaliaNessuna valutazione finora
- Imperforate Anus PDFDocumento3 pagineImperforate Anus PDFNajwaNessuna valutazione finora
- Tracheo Esophageal FistulaDocumento6 pagineTracheo Esophageal Fistulablast2111Nessuna valutazione finora
- IntussusceptionDocumento4 pagineIntussusceptionlovethestarNessuna valutazione finora
- Esophageal AtresiaDocumento4 pagineEsophageal Atresiafidc_0428Nessuna valutazione finora
- Esophageal Atresia: DR - Ibrahim AlsbouDocumento21 pagineEsophageal Atresia: DR - Ibrahim Alsbouraed faisalNessuna valutazione finora
- RLQ PainDocumento20 pagineRLQ PainBEATRICE SOPHIA PARMANessuna valutazione finora
- Pediatrics - Failure To Pass Meconium PDFDocumento2 paginePediatrics - Failure To Pass Meconium PDFJasmine KangNessuna valutazione finora
- Meconium Plug SyndromeDocumento3 pagineMeconium Plug SyndromeGlen Jacobs SumadihardjaNessuna valutazione finora
- Shalita Dastamuar Pediatric Surgery Subdivision, Surgery Department Mohammad Hoesin HospitalDocumento18 pagineShalita Dastamuar Pediatric Surgery Subdivision, Surgery Department Mohammad Hoesin HospitalSoni TfacNessuna valutazione finora
- Pyloric StenosisDocumento3 paginePyloric Stenosismagisasamundo100% (1)
- Muhimbili University of Health and Allied Sciences. School of NursingDocumento21 pagineMuhimbili University of Health and Allied Sciences. School of NursingJerilee SoCute WattsNessuna valutazione finora
- Duodenal AtresiaDocumento18 pagineDuodenal AtresiaRianto Noviady RamliNessuna valutazione finora
- Pediatric Surgery Notes For NursesDocumento8 paginePediatric Surgery Notes For NursesAhmed SamyNessuna valutazione finora
- Atresia EsofagusDocumento7 pagineAtresia EsofagusTommysNessuna valutazione finora
- Esophageal Surgery in Newborns, Infants and Children: and K.L.N. RaoDocumento5 pagineEsophageal Surgery in Newborns, Infants and Children: and K.L.N. RaoDonny Artya KesumaNessuna valutazione finora
- Oesophageal Atresia by GabriellaDocumento7 pagineOesophageal Atresia by GabriellaGabrielleNessuna valutazione finora
- Screenshot 2022-05-30 at 9.43.21 PMDocumento23 pagineScreenshot 2022-05-30 at 9.43.21 PMAZNessuna valutazione finora
- Oesophagealatresia 120920081900 Phpapp01Documento37 pagineOesophagealatresia 120920081900 Phpapp01Mulugeta AbenehNessuna valutazione finora
- Chapter X.4. Intussusception: Case Based Pediatrics For Medical Students and ResidentsDocumento5 pagineChapter X.4. Intussusception: Case Based Pediatrics For Medical Students and ResidentsNawaf Rahi AlshammariNessuna valutazione finora
- Emergencies in GITDocumento7 pagineEmergencies in GITsssajiNessuna valutazione finora
- Git Congenital AbnormalitiesDocumento3 pagineGit Congenital Abnormalitiesokureblessing33Nessuna valutazione finora
- IntussusceptionDocumento24 pagineIntussusceptionOjambo Flavia100% (1)
- Umbilical Hernia - Wikipedia PDFDocumento31 pagineUmbilical Hernia - Wikipedia PDFNeelamNessuna valutazione finora
- Case Report Duodenal Stenosis in 3 Month Boy: Compiled byDocumento15 pagineCase Report Duodenal Stenosis in 3 Month Boy: Compiled byMuhammad Khairuna SyahPutraNessuna valutazione finora
- Imperforate AnusDocumento8 pagineImperforate AnusBâchtyăr Đ'jâckêrsNessuna valutazione finora
- Cleft PalateDocumento16 pagineCleft PalateAnu Priya GopuNessuna valutazione finora
- Pyloric Stenosis WDocumento11 paginePyloric Stenosis WKlaue Neiv CallaNessuna valutazione finora
- Anorectal Malformations HandoutDocumento4 pagineAnorectal Malformations HandoutShikha Acharya100% (1)
- Rectal & Large Intestinal Atresia/Stenosis: Minnesota Department of Health Fact Sheet November 2005Documento3 pagineRectal & Large Intestinal Atresia/Stenosis: Minnesota Department of Health Fact Sheet November 2005chuck55Nessuna valutazione finora
- Navan Ee Than 2015Documento7 pagineNavan Ee Than 2015Yacine Tarik AizelNessuna valutazione finora
- EA TEF Review 1970Documento23 pagineEA TEF Review 1970Gunduz AgaNessuna valutazione finora
- GastroentrologyDocumento204 pagineGastroentrologyahmed_abu_alrobNessuna valutazione finora
- IntussusceptionDocumento4 pagineIntussusceptionBlue TechNessuna valutazione finora
- Dysphagia, A Simple Guide To The Condition, Treatment And Related ConditionsDa EverandDysphagia, A Simple Guide To The Condition, Treatment And Related ConditionsValutazione: 5 su 5 stelle5/5 (1)
- Case Study in Obstetrics and Gynaecology - Lecture Notes, Study Material and Important Questions, AnswersDocumento11 pagineCase Study in Obstetrics and Gynaecology - Lecture Notes, Study Material and Important Questions, AnswersM.V. TV100% (2)
- Pone 0230978Documento20 paginePone 0230978Sanket TelangNessuna valutazione finora
- GTDocumento26 pagineGTKhunsa JunaidNessuna valutazione finora
- The Feeding Practices and Structure Questionnaire: Construction and Initial Validation in A Sample of Australian First-Time Mothers and Their 2-Year OldsDocumento14 pagineThe Feeding Practices and Structure Questionnaire: Construction and Initial Validation in A Sample of Australian First-Time Mothers and Their 2-Year OldsSanket TelangNessuna valutazione finora
- Community and Health NursingDocumento22 pagineCommunity and Health NursingRam TyagiNessuna valutazione finora
- Mrs.G. Prameela, Prof.A.PadmajaDocumento9 pagineMrs.G. Prameela, Prof.A.PadmajaSanket TelangNessuna valutazione finora
- KAB Baseline FeedingQuestionnaire04July07Documento7 pagineKAB Baseline FeedingQuestionnaire04July07Sanket TelangNessuna valutazione finora
- Oertay: PathogevleaisDocumento5 pagineOertay: PathogevleaisSanket TelangNessuna valutazione finora
- Pe 09042Documento8 paginePe 09042Sanket TelangNessuna valutazione finora
- Efficiency of Breastfeeding As Compared To BottleDocumento9 pagineEfficiency of Breastfeeding As Compared To BottleSanket TelangNessuna valutazione finora
- Factors Influencing High Socio-Economic Class Mothers' Decision Regarding Formula-Feeding Practices in The Cape MetropoleDocumento8 pagineFactors Influencing High Socio-Economic Class Mothers' Decision Regarding Formula-Feeding Practices in The Cape MetropoleSanket TelangNessuna valutazione finora
- Assessment of The Nutritional Status of Bottle-FedDocumento7 pagineAssessment of The Nutritional Status of Bottle-FedSanket TelangNessuna valutazione finora
- Abruptio Placentae Nursing Care & ManagementDocumento10 pagineAbruptio Placentae Nursing Care & ManagementSanket TelangNessuna valutazione finora
- CopfrontDocumento1 paginaCopfrontSanket TelangNessuna valutazione finora
- Efficiency of Breastfeeding As Compared To BottleDocumento9 pagineEfficiency of Breastfeeding As Compared To BottleSanket TelangNessuna valutazione finora
- Placenta Previa Nursing Care Plan and ManagementDocumento9 paginePlacenta Previa Nursing Care Plan and ManagementSanket TelangNessuna valutazione finora
- Adobe Scan 03 Dec 2020Documento1 paginaAdobe Scan 03 Dec 2020Sanket TelangNessuna valutazione finora
- (A Depinttom: Public HeDocumento4 pagine(A Depinttom: Public HeSanket TelangNessuna valutazione finora
- Neko 3 Z 1573311312Documento180 pagineNeko 3 Z 1573311312Sanket TelangNessuna valutazione finora
- Care of Patient With ECTDocumento1 paginaCare of Patient With ECTSanket TelangNessuna valutazione finora
- Budgeting: Features of BudgetDocumento5 pagineBudgeting: Features of BudgetSanket TelangNessuna valutazione finora
- MSN Assignment - HeadacheDocumento10 pagineMSN Assignment - HeadacheSanket TelangNessuna valutazione finora
- Wardmanagement Peditric WardDocumento19 pagineWardmanagement Peditric WardSanket TelangNessuna valutazione finora
- Viva QuestionsDocumento2 pagineViva QuestionsSanket TelangNessuna valutazione finora
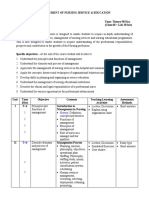
- Management SyllabusDocumento13 pagineManagement SyllabussandhyakrishnanNessuna valutazione finora
- Aniket 1723Documento1 paginaAniket 1723Sanket TelangNessuna valutazione finora
- Grounded Theory - WikipediaDocumento103 pagineGrounded Theory - WikipediaSanket TelangNessuna valutazione finora
- Indian Entrepreneur Fund PresentationDocumento44 pagineIndian Entrepreneur Fund PresentationHARIHARAN ANessuna valutazione finora
- Current Trends in Teaching and Learning EFLDocumento13 pagineCurrent Trends in Teaching and Learning EFLyimigor100% (1)
- Queens, Consorts, ConcubinesDocumento217 pagineQueens, Consorts, ConcubinesAlbertoPitaNessuna valutazione finora
- How To Pay by DBSDocumento2 pagineHow To Pay by DBSYe GaungNessuna valutazione finora
- TPHSF Feb 2006Documento8 pagineTPHSF Feb 2006nsidneyNessuna valutazione finora
- Quality TranslationDocumento33 pagineQuality TranslationCarolina ContrerasNessuna valutazione finora
- Lesson Plan 9th Grade ScienceDocumento2 pagineLesson Plan 9th Grade Scienceapi-316973807Nessuna valutazione finora
- Cryptocurrency: Presented By: Shashi KumarDocumento15 pagineCryptocurrency: Presented By: Shashi KumaraabhasNessuna valutazione finora
- Dot Net TricksDocumento101 pagineDot Net TrickssathishmnmNessuna valutazione finora
- Tata Steel Europe LTDDocumento22 pagineTata Steel Europe LTDEntertainment OverloadedNessuna valutazione finora
- Payment Item Charges (RM) Discount (RM) Service Tax (RM) Payment Method Final Charges (RM)Documento1 paginaPayment Item Charges (RM) Discount (RM) Service Tax (RM) Payment Method Final Charges (RM)Md IsmailNessuna valutazione finora
- PW 1987 01 PDFDocumento80 paginePW 1987 01 PDFEugenio Martin CuencaNessuna valutazione finora
- C Programming UnionsDocumento3 pagineC Programming UnionsslspaNessuna valutazione finora
- Advanced Space Propulsion Based On VacuumDocumento17 pagineAdvanced Space Propulsion Based On VacuumMystery Wire100% (1)
- The Lucid Dream Exchange Magazine Issue 36Documento36 pagineThe Lucid Dream Exchange Magazine Issue 36api-384230967% (3)
- Seven Days in The Art World - Sarah ThorntonDocumento249 pagineSeven Days in The Art World - Sarah ThorntonTô Tiêu NgọcNessuna valutazione finora
- FijiTimes - June 7 2013Documento48 pagineFijiTimes - June 7 2013fijitimescanadaNessuna valutazione finora
- Additive ManufactDocumento61 pagineAdditive ManufactAnca Maria TruscaNessuna valutazione finora
- Map of Jeju: For Muslim TouristsDocumento7 pagineMap of Jeju: For Muslim TouristslukmannyeoNessuna valutazione finora
- 2001OxfEnc - Oxford Encyclopaedia of Ancient EgyptDocumento13 pagine2001OxfEnc - Oxford Encyclopaedia of Ancient EgyptDorrcolacNessuna valutazione finora
- Nunez Rodarte v. Holder, JR., 10th Cir. (2010)Documento7 pagineNunez Rodarte v. Holder, JR., 10th Cir. (2010)Scribd Government DocsNessuna valutazione finora
- Safari - 15 Nov 2023 at 8:34 PMDocumento1 paginaSafari - 15 Nov 2023 at 8:34 PMrgk966c275Nessuna valutazione finora
- Hamlet Greek TragedyDocumento21 pagineHamlet Greek TragedyJorge CanoNessuna valutazione finora
- Faunus Homebrew PDFDocumento3 pagineFaunus Homebrew PDFPaul FernandezNessuna valutazione finora
- MC DuroDesign EDocumento8 pagineMC DuroDesign Epetronela.12Nessuna valutazione finora
- Against Temple Adverse Possession by Private PersonDocumento12 pagineAgainst Temple Adverse Possession by Private PersonBest NiftyNessuna valutazione finora