Potrebbero piacerti anche
- Application For Barangay Protection Order: Vawc Form#3 CONTROL NO.Documento1 paginaApplication For Barangay Protection Order: Vawc Form#3 CONTROL NO.Jacjac Famador86% (7)
- Application For Barangay Protection OrderDocumento3 pagineApplication For Barangay Protection OrderGeraldine Longasa-Templonuevo100% (2)
- DILG VAWC FormDocumento5 pagineDILG VAWC FormMah Jane Divina100% (1)
- VAWC FormsDocumento4 pagineVAWC Formsemmanuel quirinoNessuna valutazione finora
- Barangay Protection Order: (Date and Time)Documento2 pagineBarangay Protection Order: (Date and Time)Patrick Jorge Sibayan100% (8)
- Application For Barangay Protection OrderDocumento3 pagineApplication For Barangay Protection OrderTabuco Barangay HallNessuna valutazione finora
- Vawc FormDocumento1 paginaVawc FormSheila Corpuz100% (3)
- B.P.O Vawc Form4Documento1 paginaB.P.O Vawc Form4Marilyn Garcio100% (3)
- Barangay Protection OrderDocumento1 paginaBarangay Protection OrderYsa Reyes70% (20)
- Barangay Protection Order: Vawc Form#4 CTRL - NO.Documento2 pagineBarangay Protection Order: Vawc Form#4 CTRL - NO.Jacjac Famador95% (21)
- Barangay Protection Order (Bpo)Documento1 paginaBarangay Protection Order (Bpo)John Arbrith Isip Esposo83% (6)
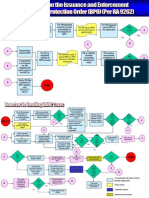
- BPO FlowchartDocumento2 pagineBPO Flowchartnhaeizy100% (14)
- Vawc FormDocumento1 paginaVawc FormRegina Palafox Tolosa100% (3)
- KP Cases Report FormDocumento3 pagineKP Cases Report FormJes Sel100% (1)
- Brgy. Protection OrderDocumento2 pagineBrgy. Protection OrderGraffiti Mugs81% (16)
- Barangay VAW Desk Quarterly Accomplishment ReportDocumento1 paginaBarangay VAW Desk Quarterly Accomplishment ReportNicodeo Vicente Ignacio75% (4)
- KP Form #28 (Monthly Transmittal of Final Reports)Documento1 paginaKP Form #28 (Monthly Transmittal of Final Reports)Murphy Red100% (5)
- Lupong Tagapamayapa Incentives Awards 2018 Barangay Gubatan Maco ComVal Province EntryDocumento40 pagineLupong Tagapamayapa Incentives Awards 2018 Barangay Gubatan Maco ComVal Province EntryArniel Fred Tormis Fernandez92% (25)
- BCPC Refferral FormDocumento1 paginaBCPC Refferral FormJana Lei Cayanan Daquiado100% (2)
- Flowchart in Handling VAWC Cases Part 1Documento1 paginaFlowchart in Handling VAWC Cases Part 1myjourney75% (4)
- VAWC NEW FORMAT QuarterlyDocumento1 paginaVAWC NEW FORMAT QuarterlyBrgy. Roxas75% (4)
- Intake Sheet For VAWCDocumento2 pagineIntake Sheet For VAWCDaisy Palero Tibayan88% (8)
- VAWC Referral FormDocumento2 pagineVAWC Referral FormBarangay Perez100% (1)
- Resolution Organizing BDCDocumento3 pagineResolution Organizing BDCAilex Store84% (19)
- BCPC Action Plan 2017Documento3 pagineBCPC Action Plan 2017Danilo Posion86% (7)
- Individual Record of Barangay InhabitantsDocumento1 paginaIndividual Record of Barangay InhabitantsAldrin Dela Cruz80% (5)
- Barangay Protection Order SampleDocumento1 paginaBarangay Protection Order SampleRaymond Galang100% (6)
- Executive Order BHERTsDocumento2 pagineExecutive Order BHERTsJemarie Faith de Guzman0% (1)
- BADAC FORM - Activity ReportDocumento2 pagineBADAC FORM - Activity ReportMikeNessuna valutazione finora
- VAW Desk Form 5Documento1 paginaVAW Desk Form 5neneng sa pinta100% (1)
- VAWC Accomplishment ReportDocumento1 paginaVAWC Accomplishment ReportBarangay Palabotan100% (4)
- VAW Desk Form 5Documento1 paginaVAW Desk Form 5Eduardo Cases100% (4)
- Handling Anti-Vawc Cases FlowchartDocumento2 pagineHandling Anti-Vawc Cases FlowchartJaylyn Joya Ammang100% (7)
- VAW Feedback FormDocumento1 paginaVAW Feedback FormBarangay Mabacan100% (2)
- 2017 BPOC Activity Report Anti-TerrorismDocumento2 pagine2017 BPOC Activity Report Anti-TerrorismChristy Ledesma-NavarroNessuna valutazione finora
- BCPC Intake FormDocumento2 pagineBCPC Intake FormAileen Labastida BarcenasNessuna valutazione finora
- E.O. Creating Barangay Cluster LeadersDocumento3 pagineE.O. Creating Barangay Cluster LeadersRB Beltran100% (2)
- BCPC Executive Order 008-2016Documento2 pagineBCPC Executive Order 008-2016Romergalba Alba90% (73)
- VAW Desk Form 5Documento1 paginaVAW Desk Form 5Eduardo Cases100% (2)
- DILG MC 2016-58 (LTIA) Enhanced Criteria & GuidelinesDocumento51 pagineDILG MC 2016-58 (LTIA) Enhanced Criteria & GuidelinesDex Castro Narrido100% (3)
- BCPC 2nd QTR Meeting Minutes 2017Documento2 pagineBCPC 2nd QTR Meeting Minutes 2017Anne Abellanosa100% (2)
- EO 2016-001 Brgy Nutrition CommitteeDocumento1 paginaEO 2016-001 Brgy Nutrition CommitteeChona Burgos73% (22)
- Vawc New Format QuarterlyDocumento1 paginaVawc New Format QuarterlyBrgy. Roxas100% (2)
- RBI Form 1Documento2 pagineRBI Form 1lorena85% (13)
- BCPC GuidelinesDocumento6 pagineBCPC GuidelinesValred57% (7)
- Kasambahay FormDocumento1 paginaKasambahay FormMarieta Alejo0% (1)
- Barangay Official Information Sheet FormDocumento3 pagineBarangay Official Information Sheet Formrbero100% (1)
- BNEO 10 Anti-Violence Against Women and Their ChildrenDocumento61 pagineBNEO 10 Anti-Violence Against Women and Their ChildrenCarlito F. Faina, Jr.100% (1)
- Barangay Disiplina Brigade EODocumento3 pagineBarangay Disiplina Brigade EOPatrick Jorge Sibayan100% (3)
- Office of The Punong Barangay: MinutesDocumento3 pagineOffice of The Punong Barangay: MinutesNoraisa Midtimbang67% (3)
- Vawc Form #3 Application For BPODocumento1 paginaVawc Form #3 Application For BPOJoy Toledo EnarsicoNessuna valutazione finora
- Barangay Protection OrderDocumento1 paginaBarangay Protection OrderJhon Lloyd Sumabat CarbonquilloNessuna valutazione finora
- VAWC FormDocumento1 paginaVAWC FormJoaquin Iniego SebastianNessuna valutazione finora
- Bpo Form No. 3Documento1 paginaBpo Form No. 3Jonas QuilantipNessuna valutazione finora
- Bpo Application FormDocumento2 pagineBpo Application FormJerome Magno BalaquidanNessuna valutazione finora
- Vawc Form #5Documento2 pagineVawc Form #5Joy Toledo Enarsico100% (1)
- 9048 10172 Form 1.1 CCE BCDocumento2 pagine9048 10172 Form 1.1 CCE BCjennylynne100% (1)
- VAWC FormsDocumento4 pagineVAWC Formsjohn dexter abiertasNessuna valutazione finora
- Office of The Punong-Barangay: OrderDocumento4 pagineOffice of The Punong-Barangay: Orderjay jay sagunNessuna valutazione finora
- Petition For Correction of Clerical Error in The Certificate of Live BirthDocumento2 paginePetition For Correction of Clerical Error in The Certificate of Live BirthWreigh ParisNessuna valutazione finora
- Justice Carpio Speech On China's Claim Over Spratly'sDocumento5 pagineJustice Carpio Speech On China's Claim Over Spratly'sAnnaLynneL.TaguilingNessuna valutazione finora
- Vikramgad Assembly FactbookDocumento16 pagineVikramgad Assembly FactbookKHUSHI WADHAWANNessuna valutazione finora
- Ethnic Relations in Peninsular Malaysia: The Cultural and Economic DimensionsDocumento48 pagineEthnic Relations in Peninsular Malaysia: The Cultural and Economic DimensionsTimy Foo100% (1)
- 04 - Asymmetric Information - Moral HazardDocumento24 pagine04 - Asymmetric Information - Moral Hazardepl_manutdNessuna valutazione finora
- Health Is Wealth: An Analysis On Domestic and International Healthcare SystemsDocumento2 pagineHealth Is Wealth: An Analysis On Domestic and International Healthcare SystemsKrizelle ClaveriaNessuna valutazione finora
- Council For National PolicDocumento63 pagineCouncil For National PolicGregory HooNessuna valutazione finora
- RULE 7 of The Rules of Court New (FINAL)Documento55 pagineRULE 7 of The Rules of Court New (FINAL)YenMojicaNessuna valutazione finora
- Content:: Saudi Arabian Oil Company (Saudi Aramco) General Instruction ManualDocumento6 pagineContent:: Saudi Arabian Oil Company (Saudi Aramco) General Instruction Manualmalika_00100% (1)
- Coop by LawsDocumento35 pagineCoop by LawsJodie AldeaNessuna valutazione finora
- Rural Livelihoods in ZimbabweDocumento74 pagineRural Livelihoods in ZimbabweAlchristel100% (1)
- Revolutionary MovementsDocumento39 pagineRevolutionary MovementsanahidalNessuna valutazione finora
- Renunciation of Citizenship FormDocumento11 pagineRenunciation of Citizenship FormjosephkiwiNessuna valutazione finora
- 01-26. in Re Elmo AbadDocumento3 pagine01-26. in Re Elmo AbadOdette JumaoasNessuna valutazione finora
- Chicken Soup With Barley Resource PackDocumento24 pagineChicken Soup With Barley Resource PackSreelakshmi ShylajanNessuna valutazione finora
- Qadira Stephens v. Multnomah County OHSU Providence For Malpractice, Child Abuse, Burn, Hate CrimeDocumento71 pagineQadira Stephens v. Multnomah County OHSU Providence For Malpractice, Child Abuse, Burn, Hate Crimemary engNessuna valutazione finora
- 450 California History IntroductionDocumento25 pagine450 California History IntroductionJay JaberNessuna valutazione finora
- United Nations High Commissioner For RefugeesDocumento2 pagineUnited Nations High Commissioner For RefugeesNataliaNessuna valutazione finora
- Chapter 5 Congress: The Legislative BranchDocumento40 pagineChapter 5 Congress: The Legislative BranchlightbeatleNessuna valutazione finora
- Does Greek Historical Memory Shape NostalgiaDocumento9 pagineDoes Greek Historical Memory Shape NostalgiaAisha KhanNessuna valutazione finora
- Brgy. & SK Elections Watchers' GuideDocumento103 pagineBrgy. & SK Elections Watchers' GuideuntayaoNessuna valutazione finora
- English Essay - Mandatory National Service RequirementDocumento4 pagineEnglish Essay - Mandatory National Service RequirementhomenetworkNessuna valutazione finora
- Salvini AscendantDocumento22 pagineSalvini AscendantLuis ImbachNessuna valutazione finora
- Ferdinand MarcosDocumento23 pagineFerdinand MarcosAllison SilvestreNessuna valutazione finora
- Tanggungjawab Dan Tindakan Tanggungjawab Tindakan MKP/MKKDocumento13 pagineTanggungjawab Dan Tindakan Tanggungjawab Tindakan MKP/MKKAmalinaNessuna valutazione finora
- Historical Foundations of RaceDocumento2 pagineHistorical Foundations of Raceapi-533945853Nessuna valutazione finora
- APOLINARIO AMANDA VALDEZ, G.R. No. 201655 DIGESTDocumento3 pagineAPOLINARIO AMANDA VALDEZ, G.R. No. 201655 DIGESTMichael James Madrid MalinginNessuna valutazione finora
- Game Plan Naviance StudentDocumento4 pagineGame Plan Naviance Studentapi-458881081Nessuna valutazione finora
- 2hours Training ModuleDocumento24 pagine2hours Training ModuleMacky Paul Masong AmoresNessuna valutazione finora
- Key Take-Away or Doctrine To RememberDocumento2 pagineKey Take-Away or Doctrine To RememberMarie TitularNessuna valutazione finora
- G20 Report EngDocumento156 pagineG20 Report EngCynthiaMcLeodSunNessuna valutazione finora