Potrebbero piacerti anche
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (73)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- 5.thyroid Gland LectureDocumento96 pagine5.thyroid Gland Lecturesdsher100% (3)
- The Silver Lining PlaybookDocumento4 pagineThe Silver Lining PlaybookJanine Dela CruzNessuna valutazione finora
- Solar Radiation On Cloudy DaysDocumento10 pagineSolar Radiation On Cloudy Daysioan_vNessuna valutazione finora
- Light Concentration Effect On PV Performance and EfficiencyDocumento5 pagineLight Concentration Effect On PV Performance and Efficiencyioan_vNessuna valutazione finora
- Copper Oxide Based Nanostructures For Improved Solar Cell EfficiencyDocumento9 pagineCopper Oxide Based Nanostructures For Improved Solar Cell Efficiencyioan_vNessuna valutazione finora
- Effect of Light Intensity - PVEducationDocumento3 pagineEffect of Light Intensity - PVEducationioan_vNessuna valutazione finora
- Nonclassical Light GenerationDocumento12 pagineNonclassical Light Generationioan_vNessuna valutazione finora
- User Guide J2me Sony-Ericsson 2004Documento134 pagineUser Guide J2me Sony-Ericsson 2004ioan_vNessuna valutazione finora
- Basic Customization GuideDocumento32 pagineBasic Customization GuideP Clement LloydNessuna valutazione finora
- Condus EcologicDocumento1 paginaCondus Ecologicioan_vNessuna valutazione finora
- Cancer Prevention With Green Tea and Its Principal Constituent, EGCGDocumento1 paginaCancer Prevention With Green Tea and Its Principal Constituent, EGCGioan_vNessuna valutazione finora
- Piperlongumine Induces Apoptosis and Autophagy in Human Lung Cancer CellsDocumento12 paginePiperlongumine Induces Apoptosis and Autophagy in Human Lung Cancer Cellsioan_vNessuna valutazione finora
- Piperlongumine Induces Apoptosis and Autophagy in Human Lung Cancer CellsDocumento12 paginePiperlongumine Induces Apoptosis and Autophagy in Human Lung Cancer Cellsioan_vNessuna valutazione finora
- Heat of Solution DataDocumento2 pagineHeat of Solution Dataioan_vNessuna valutazione finora
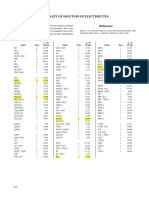
- Enthalpies of Solution of ElectrolytesDocumento1 paginaEnthalpies of Solution of ElectrolytesFavio Andrés ChavezNessuna valutazione finora
- Carbon-Steam Reaction at Elevated TemperatureDocumento4 pagineCarbon-Steam Reaction at Elevated Temperatureioan_vNessuna valutazione finora
- Physical Properties of RefrigerantsDocumento2 paginePhysical Properties of Refrigerantsioan_vNessuna valutazione finora
- Iron Phosphate Glasses PDFDocumento10 pagineIron Phosphate Glasses PDFioan_vNessuna valutazione finora
- SulfurDocumento22 pagineSulfurWijayanto AKNessuna valutazione finora
- Baterii Litiu SulfDocumento10 pagineBaterii Litiu Sulfioan_vNessuna valutazione finora
- Reduction and Oxidation PotentialDocumento1 paginaReduction and Oxidation Potentialioan_vNessuna valutazione finora
- Subclassing and Hooking With Visual Basic PDFDocumento687 pagineSubclassing and Hooking With Visual Basic PDFioan_vNessuna valutazione finora
- 8DDocumento10 pagine8DaminNessuna valutazione finora
- A Miller Heavy WaterDocumento14 pagineA Miller Heavy Waterioan_vNessuna valutazione finora
- D G Model Making Sense of Clinical Examination of The Adult Patient Hands-On GuideDocumento313 pagineD G Model Making Sense of Clinical Examination of The Adult Patient Hands-On GuidevaidyamNessuna valutazione finora
- Chist de Septum PellucidumDocumento3 pagineChist de Septum PellucidumdansarariuNessuna valutazione finora
- Couvade Syndrome and PseudocyesisDocumento4 pagineCouvade Syndrome and PseudocyesisJustin Ahorro-DionisioNessuna valutazione finora
- Warfarin Reversal Guideline 2012 PDFDocumento8 pagineWarfarin Reversal Guideline 2012 PDFVlady78Nessuna valutazione finora
- PATHOPHYSIOLOGY OF OSTEOSARCOMaDocumento1 paginaPATHOPHYSIOLOGY OF OSTEOSARCOMakyawNessuna valutazione finora
- Jama Statin and Stroke Prevention SupplementDocumento17 pagineJama Statin and Stroke Prevention SupplementMesan KoNessuna valutazione finora
- NGT LavageDocumento16 pagineNGT LavageTina Alteran100% (1)
- MNT For Rheumatic DiseaseDocumento107 pagineMNT For Rheumatic DiseasejwhssanNessuna valutazione finora
- Global Submission On IndDocumento16 pagineGlobal Submission On IndRahul PalsNessuna valutazione finora
- Medication Order ReviewDocumento34 pagineMedication Order ReviewVidho RiveraNessuna valutazione finora
- Basic Need For GeriatricsDocumento38 pagineBasic Need For GeriatricsMuhammad Yatsrib SemmeNessuna valutazione finora
- Cardiorespiratory Endurance and The Fitt PrincipleDocumento2 pagineCardiorespiratory Endurance and The Fitt Principleapi-385952225Nessuna valutazione finora
- Red Tide: Causative AgentDocumento2 pagineRed Tide: Causative Agentchristian quiaoitNessuna valutazione finora
- Doctor'S Order and Progress NotesDocumento3 pagineDoctor'S Order and Progress NotesDienizs LabiniNessuna valutazione finora
- TiroideDocumento10 pagineTiroideRosália CoutadaNessuna valutazione finora
- DRUGS Initial StockDocumento163 pagineDRUGS Initial StockdeasyNessuna valutazione finora
- Daftar DiagnosaDocumento6 pagineDaftar DiagnosaSr Immaculata SSpSNessuna valutazione finora
- Saddle BlockDocumento3 pagineSaddle BlockVasu DevanNessuna valutazione finora
- Epileptic Disorders - 2021 - Leibetseder - How To Distinguish Seizures From Non Epileptic ManifestationsDocumento23 pagineEpileptic Disorders - 2021 - Leibetseder - How To Distinguish Seizures From Non Epileptic ManifestationsFranklin SierraNessuna valutazione finora
- Fluid, Electrolytes, Acid Base BalanceDocumento18 pagineFluid, Electrolytes, Acid Base Balanceashdmb217100% (5)
- Service Annotated BibliographyDocumento6 pagineService Annotated Bibliographyapi-355966257Nessuna valutazione finora
- Medical ProformaDocumento6 pagineMedical ProformaShahaan ZulfiqarNessuna valutazione finora
- Lyrica - Prescribing InfoDocumento42 pagineLyrica - Prescribing InfoPoojaNessuna valutazione finora
- To Extract Ornot To Extract PDFDocumento2 pagineTo Extract Ornot To Extract PDFmehdi chahrourNessuna valutazione finora
- Bad Pharma - A Fraud in Clinical Trail DataDocumento27 pagineBad Pharma - A Fraud in Clinical Trail DataSimran WaghelaNessuna valutazione finora
- Presentation On Wrist DropDocumento13 paginePresentation On Wrist DropMuhammadArshadNessuna valutazione finora
- FibromyalgiaDocumento36 pagineFibromyalgiaSyed Tameem Ul HassanNessuna valutazione finora
- Mental DisorderDocumento18 pagineMental DisorderMaria Gabriela GimenezNessuna valutazione finora