Potrebbero piacerti anche
- Rapid Interpretation of EKG's 6th EdDocumento14 pagineRapid Interpretation of EKG's 6th EdDenise De Los Reyes100% (2)
- Symbols of Oil Gas PipingDocumento3 pagineSymbols of Oil Gas PipingDelvin Davis M0% (1)
- 2020 FAS1 Section IV Resource Reviews-1 PDFDocumento24 pagine2020 FAS1 Section IV Resource Reviews-1 PDFAbhilasha SharmaNessuna valutazione finora
- GCSE Higher Student Book Unit Test AnswersDocumento26 pagineGCSE Higher Student Book Unit Test Answersswiftmessi100% (5)
- Achidram, Ashwamedham & KatakamDocumento228 pagineAchidram, Ashwamedham & KatakamSubhash Sharma100% (9)
- HVAC Control in The New MillenniumDocumento389 pagineHVAC Control in The New Millenniumnicky1213aNessuna valutazione finora
- Scholl Hammer 2015Documento7 pagineScholl Hammer 2015jesslynNessuna valutazione finora
- JCDR 8 JC13Documento4 pagineJCDR 8 JC13andi hajrahNessuna valutazione finora
- WJG 25 3823Documento16 pagineWJG 25 3823monica ortizNessuna valutazione finora
- Nutritional Status and Anaemia in Medical Students of Sgrdimsar, AmritsarDocumento5 pagineNutritional Status and Anaemia in Medical Students of Sgrdimsar, AmritsarOcha24 TupamahuNessuna valutazione finora
- 4 - M - NizarDocumento10 pagine4 - M - NizarDianLianyNessuna valutazione finora
- Jurnal 3Documento10 pagineJurnal 3rinaldy agungNessuna valutazione finora
- Dietary Patterns and Gallstone Risks in Chinese AdDocumento7 pagineDietary Patterns and Gallstone Risks in Chinese AdInfo TradersNessuna valutazione finora
- UlcerDocumento5 pagineUlcerabriyahNessuna valutazione finora
- Kleinman 2011Documento9 pagineKleinman 2011rsthsn6z8xNessuna valutazione finora
- 10 11648 J Ajim 20150303 13Documento8 pagine10 11648 J Ajim 20150303 13Fate ChanNessuna valutazione finora
- Prevalence of Dysmenorrhea and Its Sequel Among Medical Students in A Malaysian UniversityDocumento12 paginePrevalence of Dysmenorrhea and Its Sequel Among Medical Students in A Malaysian UniversityClaudia MadonnaNessuna valutazione finora
- Me Dite RanianDocumento10 pagineMe Dite Raniantamita21airenNessuna valutazione finora
- Medication Adherence in Inflammatory Bowel Disease: ReviewDocumento12 pagineMedication Adherence in Inflammatory Bowel Disease: ReviewVirgo WNessuna valutazione finora
- AdvBiomedRes71127-3687982 - 101439 INTERNATIONALDocumento10 pagineAdvBiomedRes71127-3687982 - 101439 INTERNATIONALHidayatt NurulNessuna valutazione finora
- Eating Habits and Nutritional Status Among the Bangladeshi Medical مهم 2Documento5 pagineEating Habits and Nutritional Status Among the Bangladeshi Medical مهم 2د.شيماءسعيدNessuna valutazione finora
- 2 +vania+et+al+ (8-18)Documento11 pagine2 +vania+et+al+ (8-18)Brin UndikmaNessuna valutazione finora
- Sarc X Con 2Documento6 pagineSarc X Con 2Samuel SilvaNessuna valutazione finora
- 10884-Article Text-46324-3-10-20230725mDocumento8 pagine10884-Article Text-46324-3-10-20230725mMacchiatoNessuna valutazione finora
- Prevalence of Gastroesophageal Reflux Disease (GERD) in Dyspepsia Patients in Primary Referral HospitalDocumento6 paginePrevalence of Gastroesophageal Reflux Disease (GERD) in Dyspepsia Patients in Primary Referral HospitalAbrar TaraNessuna valutazione finora
- A Study of Helicobacter Pylori Infection, Dietary Pattern and Habits in Patients With Gastric Cancer in South IndiaDocumento3 pagineA Study of Helicobacter Pylori Infection, Dietary Pattern and Habits in Patients With Gastric Cancer in South Indiacut irnandaNessuna valutazione finora
- Prevalensi Dan Faktor AsosiasiDocumento11 paginePrevalensi Dan Faktor Asosiasisahama2508Nessuna valutazione finora
- Kata Kunci: Pengetahuan Gizi Seimbang, Praktik Gizi SeimbangDocumento9 pagineKata Kunci: Pengetahuan Gizi Seimbang, Praktik Gizi SeimbangShifa Minhatun Niza'Nessuna valutazione finora
- Prevalence of A Gluten Free Diet and Improvement of ClinicalDocumento9 paginePrevalence of A Gluten Free Diet and Improvement of ClinicalNejc KovačNessuna valutazione finora
- Nutritional Assessment of Children With CHD CompareDocumento9 pagineNutritional Assessment of Children With CHD CompareIntan Robi'ahNessuna valutazione finora
- 3 7 38 579Documento5 pagine3 7 38 579Jasleen KaurNessuna valutazione finora
- Sand 2019Documento9 pagineSand 2019isragelNessuna valutazione finora
- Junk Food Consumption Awareness and Its Health ConDocumento6 pagineJunk Food Consumption Awareness and Its Health Concristine borjaNessuna valutazione finora
- Depresi ckd3Documento14 pagineDepresi ckd3sufaNessuna valutazione finora
- Article Wjpps 1406544176 PDFDocumento14 pagineArticle Wjpps 1406544176 PDFoanacrisNessuna valutazione finora
- Lactobacillus Rhamnosus GG Versus Placebo For Acute Gastroenteritis in ChildrenDocumento21 pagineLactobacillus Rhamnosus GG Versus Placebo For Acute Gastroenteritis in ChildrenMarsella Epifania SuwignyoNessuna valutazione finora
- Prevalence and Predictors of Gastritis Among Patients Attending Health Care Facilities in Jazan, KSADocumento8 paginePrevalence and Predictors of Gastritis Among Patients Attending Health Care Facilities in Jazan, KSAShirleyNessuna valutazione finora
- Correlation of Nutritional Anemia and Blood Group Prevalence Among Adolescent Girls in Pudukkottai District of IndiaDocumento4 pagineCorrelation of Nutritional Anemia and Blood Group Prevalence Among Adolescent Girls in Pudukkottai District of IndiaOmWawanNessuna valutazione finora
- Uq333400 Oa PDFDocumento5 pagineUq333400 Oa PDFSindhi Waseem BalochNessuna valutazione finora
- 1246 7206 1 PBDocumento6 pagine1246 7206 1 PBNensy AnggrainyNessuna valutazione finora
- 2003 A Validated Symptoms Questionnaire Chinese GERDQ For Thediagnosis of Gastro Oesophageal Reflux Disease in The ChinesepopulationDocumento7 pagine2003 A Validated Symptoms Questionnaire Chinese GERDQ For Thediagnosis of Gastro Oesophageal Reflux Disease in The ChinesepopulationAhmad Yar SukheraNessuna valutazione finora
- Influence of Nutritional Status On Clinical Outcomes in Critically Ill ChildrenDocumento5 pagineInfluence of Nutritional Status On Clinical Outcomes in Critically Ill ChildrenIvana YunitaNessuna valutazione finora
- Influence of Nutritional Status On Clinical Outcomes in Critically Ill ChildrenDocumento5 pagineInfluence of Nutritional Status On Clinical Outcomes in Critically Ill ChildrenAnonymous h0DxuJTNessuna valutazione finora
- Effectiveness of Curry Leaf and Mint Decoction On Indigestion Among Geriatric Clients at Kondancherry Village, Thiruvallur DistrictDocumento5 pagineEffectiveness of Curry Leaf and Mint Decoction On Indigestion Among Geriatric Clients at Kondancherry Village, Thiruvallur DistrictEditor IJTSRDNessuna valutazione finora
- Tayem PDFDocumento8 pagineTayem PDFCynthia MelindaNessuna valutazione finora
- Intestinal - Rehabilitation - Programs - in - The Pediatric Failure and Shhort Bowel SyndromeDocumento9 pagineIntestinal - Rehabilitation - Programs - in - The Pediatric Failure and Shhort Bowel SyndromeMinosska Pinto LazoNessuna valutazione finora
- Rajiv Gandhi University of Health Sciences, Karnataka BangaloreDocumento13 pagineRajiv Gandhi University of Health Sciences, Karnataka BangaloreFebri SuryoNessuna valutazione finora
- Stadium Hiv/Aids Dan Perilaku Gizi Odha Hubungannya Dengan Status Gizi (Studi Di Rawat Jalan RSUP. Dr. Kariadi Semarang)Documento3 pagineStadium Hiv/Aids Dan Perilaku Gizi Odha Hubungannya Dengan Status Gizi (Studi Di Rawat Jalan RSUP. Dr. Kariadi Semarang)Chusnul ChotimahNessuna valutazione finora
- Nutritional and Health Status of Medical Students at A University in Northwestern Saudi ArabiaDocumento9 pagineNutritional and Health Status of Medical Students at A University in Northwestern Saudi ArabiaMiss LeslieNessuna valutazione finora
- Improving Adherence and Biomedical Markers in Hemodialysis Patients: The Effects of Relaxation TherapyDocumento9 pagineImproving Adherence and Biomedical Markers in Hemodialysis Patients: The Effects of Relaxation TherapyheriNessuna valutazione finora
- Jurnal IndaDocumento14 pagineJurnal Indabangtan illegirlNessuna valutazione finora
- Association of Gastroesophageal Reflux Disease With Anxiety, Depression, and Sleep Disorders Original ArticleDocumento8 pagineAssociation of Gastroesophageal Reflux Disease With Anxiety, Depression, and Sleep Disorders Original Articlebarokahgroup groupNessuna valutazione finora
- Comparison of Malnutrition and Malnutrition Screening Tools in Pediatric Oncology Patients A Cross-Sectional StudyDocumento5 pagineComparison of Malnutrition and Malnutrition Screening Tools in Pediatric Oncology Patients A Cross-Sectional StudySebastian MarinNessuna valutazione finora
- Ournal of Utrition Ollege: Journal of Nutrition CollegeDocumento11 pagineOurnal of Utrition Ollege: Journal of Nutrition CollegeBunga HalimNessuna valutazione finora
- 1 PB PDFDocumento12 pagine1 PB PDFMegayana Yessy MarettaNessuna valutazione finora
- Cisapride Use in Pediatric Patients With Intestinal Failure and Its Impact On Progression of Enteral NutritionDocumento6 pagineCisapride Use in Pediatric Patients With Intestinal Failure and Its Impact On Progression of Enteral Nutritionmango91286Nessuna valutazione finora
- Assessment of Dietary Pattern and Nutritional Status of Undergraduate Students in A Private University in Southern NigeriaDocumento8 pagineAssessment of Dietary Pattern and Nutritional Status of Undergraduate Students in A Private University in Southern NigeriaSunita KarkiNessuna valutazione finora
- Pharmacoeconomical Evaluationof Oral Hypoglycemic AgentsDocumento6 paginePharmacoeconomical Evaluationof Oral Hypoglycemic AgentsNamithaNessuna valutazione finora
- Evaluating The Quality of Life of Adult Patients oDocumento1 paginaEvaluating The Quality of Life of Adult Patients opspd anakNessuna valutazione finora
- Global Assessment (PG-SGA) Berhubungan Dengan Asupan ZatDocumento5 pagineGlobal Assessment (PG-SGA) Berhubungan Dengan Asupan ZatDea SaptanovaNessuna valutazione finora
- Grundmann O. & Yoon S.L. - Complementary and Alternative Medicines in IBS - An Integrative View (2014)Documento18 pagineGrundmann O. & Yoon S.L. - Complementary and Alternative Medicines in IBS - An Integrative View (2014)Laura DecockNessuna valutazione finora
- Prevalence, Pattern and Perceptions of Self-Medication in Medical StudentsDocumento7 paginePrevalence, Pattern and Perceptions of Self-Medication in Medical StudentsMr AggarwalNessuna valutazione finora
- 9378 40654 1 PBDocumento8 pagine9378 40654 1 PBNabila ZainNessuna valutazione finora
- Journal Homepage: - : 61 YearsDocumento11 pagineJournal Homepage: - : 61 YearsIJAR JOURNALNessuna valutazione finora
- Complementary and Alternative Medical Lab Testing Part 5: GastrointestinalDa EverandComplementary and Alternative Medical Lab Testing Part 5: GastrointestinalNessuna valutazione finora
- Gastrointestinal and Liver Disorders in Women’s Health: A Point of Care Clinical GuideDa EverandGastrointestinal and Liver Disorders in Women’s Health: A Point of Care Clinical GuidePoonam Beniwal-PatelNessuna valutazione finora
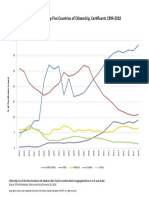
- Citizenship Stats USDocumento1 paginaCitizenship Stats USAbhilasha SharmaNessuna valutazione finora
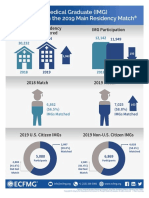
- Match 2019 Info GraphicDocumento1 paginaMatch 2019 Info GraphicUmaNessuna valutazione finora
- Circheartfailure 116 003415Documento7 pagineCircheartfailure 116 003415Abhilasha SharmaNessuna valutazione finora
- IndPsychiatryJ26171-3121189 084011Documento6 pagineIndPsychiatryJ26171-3121189 084011Abhilasha SharmaNessuna valutazione finora
- Step 1 TopicsDocumento2 pagineStep 1 TopicsTanveer AhamadNessuna valutazione finora
- Surge Arresters: Selection, Application and Testing: Pass YouDocumento30 pagineSurge Arresters: Selection, Application and Testing: Pass YouOoi Ban JuanNessuna valutazione finora
- Definitions - Topic 9 The Periodic Table - CAIE Chemistry IGCSE PDFDocumento1 paginaDefinitions - Topic 9 The Periodic Table - CAIE Chemistry IGCSE PDFAtif BakhshNessuna valutazione finora
- Spray-Agglomeration of NPK-fertilizer in A Rotating Drum Granulator PDFDocumento8 pagineSpray-Agglomeration of NPK-fertilizer in A Rotating Drum Granulator PDFKhoa TrầnNessuna valutazione finora
- Info Sphere Information Analyzer - Methodology and Best PracticesDocumento127 pagineInfo Sphere Information Analyzer - Methodology and Best PracticesRoshava KratunaNessuna valutazione finora
- S Bms ManualDocumento44 pagineS Bms ManualnathanaelorNessuna valutazione finora
- 88543-Activity Week 3 (Language of Mathematics)Documento2 pagine88543-Activity Week 3 (Language of Mathematics)Mylene L RimandoNessuna valutazione finora
- Complex Numbers SpreadsheetDocumento2 pagineComplex Numbers SpreadsheetrodwellheadNessuna valutazione finora
- Psychological, Social and Environmental BarriersDocumento12 paginePsychological, Social and Environmental BarrierssaifNessuna valutazione finora
- Automatic Mains Change Over Switch For Ups.Documento4 pagineAutomatic Mains Change Over Switch For Ups.Pooja BanNessuna valutazione finora
- ESDS312, ESDS314 Data-Line Surge and ESD Protection Diode ArrayDocumento20 pagineESDS312, ESDS314 Data-Line Surge and ESD Protection Diode ArrayBenNessuna valutazione finora
- 1 s2.0 S0960077922005665 MainDocumento8 pagine1 s2.0 S0960077922005665 MainSajjad AliNessuna valutazione finora
- 01 - Enhancing Power Density in SMPS With MasterganDocumento44 pagine01 - Enhancing Power Density in SMPS With MasterganNWorKNessuna valutazione finora
- ADAT Optical Audio Data Generator and Encoder V1401Documento8 pagineADAT Optical Audio Data Generator and Encoder V1401mylitalindaNessuna valutazione finora
- Oxygen Flak Combustion MethodDocumento2 pagineOxygen Flak Combustion MethodSandip Firke100% (2)
- AI CalculatorDocumento41 pagineAI CalculatorAneeza zafarNessuna valutazione finora
- 2-3 Histograms, Frequency Polygons, and Ogives: Chp.2 Page 1Documento2 pagine2-3 Histograms, Frequency Polygons, and Ogives: Chp.2 Page 1Suniel ChhetriNessuna valutazione finora
- Cam Less Engine.1Documento15 pagineCam Less Engine.1Pradeep KumarNessuna valutazione finora
- Ib8091en PDFDocumento1 paginaIb8091en PDFnicu secosanNessuna valutazione finora
- Lehmann Et Al 2013 PDFDocumento13 pagineLehmann Et Al 2013 PDFJack HamiltonNessuna valutazione finora
- IISER Aptitude Test 17th Sept 2021Documento22 pagineIISER Aptitude Test 17th Sept 2021Muskaan KathuriaNessuna valutazione finora
- Synchronous Generators - 2 Marks Questions and AnswersDocumento3 pagineSynchronous Generators - 2 Marks Questions and AnswersJoseph Harindranath67% (3)
- Click125 82K60H30Y 0Documento169 pagineClick125 82K60H30Y 0yeoj manaNessuna valutazione finora
- Q4 - WEEK 2 - MEASURES OF POSITION For GROUPED DATADocumento16 pagineQ4 - WEEK 2 - MEASURES OF POSITION For GROUPED DATAEllaineeeeNessuna valutazione finora
- Inorganic Chemistry 2 Main Exam (3) and MemoDocumento11 pagineInorganic Chemistry 2 Main Exam (3) and MemoKgasu MosaNessuna valutazione finora
- Autoclave CatalogueDocumento17 pagineAutoclave CatalogueUMARALEKSANA, CVNessuna valutazione finora
- Operational AmplifiersDocumento35 pagineOperational AmplifierskunwarNessuna valutazione finora