Potrebbero piacerti anche
- Cardiac Pacemakers A Basic ReviewDocumento11 pagineCardiac Pacemakers A Basic ReviewMuhammad Dilawar khanNessuna valutazione finora
- PacmakerDocumento37 paginePacmakerSalman HabeebNessuna valutazione finora
- Njihof 1996Documento13 pagineNjihof 1996api-366277227Nessuna valutazione finora
- COCHELEADocumento28 pagineCOCHELEABibin JoseNessuna valutazione finora
- Golden Accomplishments in Biomedical EngineeringDocumento31 pagineGolden Accomplishments in Biomedical EngineeringLLNessuna valutazione finora
- The Early History of The Cochlear Implant:: A RetrospectiveDocumento15 pagineThe Early History of The Cochlear Implant:: A RetrospectiveFacundo TorresNessuna valutazione finora
- Electrosurgery: History, Principles, and Current and Future UsesDocumento12 pagineElectrosurgery: History, Principles, and Current and Future Usesyacine tarikNessuna valutazione finora
- Ps 1009154 ElectrocauteryDocumento12 paginePs 1009154 ElectrocauteryWicara PutraNessuna valutazione finora
- We Almost Lost Detroit - John G. Fuller - 1975 - 363.4, 621.483Documento297 pagineWe Almost Lost Detroit - John G. Fuller - 1975 - 363.4, 621.483Jan SteinmanNessuna valutazione finora
- Computers and the General Practitioner: Proceedings of the GP-Info Symposium, London, 1980Da EverandComputers and the General Practitioner: Proceedings of the GP-Info Symposium, London, 1980Alastair MalcolmNessuna valutazione finora
- We Almost Lost DetroitDocumento297 pagineWe Almost Lost DetroitedoliscomNessuna valutazione finora
- Neurobionics: The Biomedical Engineering of Neural ProsthesesDa EverandNeurobionics: The Biomedical Engineering of Neural ProsthesesRobert K. ShepherdNessuna valutazione finora
- Reactor Safeguards: International Series of Monographs on Nuclear EnergyDa EverandReactor Safeguards: International Series of Monographs on Nuclear EnergyNessuna valutazione finora
- The Scientific Healing Method of Violet RayDocumento22 pagineThe Scientific Healing Method of Violet RayEric Van Der Worp100% (4)
- Mod RadDocumento8 pagineMod RadCherry Ann DomingoNessuna valutazione finora
- Draper Prize Program 4-24-12Documento10 pagineDraper Prize Program 4-24-12Camilo MartinezNessuna valutazione finora
- Health Concerns: History of Radiation 13Documento4 pagineHealth Concerns: History of Radiation 13CristinaNessuna valutazione finora
- Beck Protocol HandbookDocumento87 pagineBeck Protocol Handbooktejinders1125Nessuna valutazione finora
- EMR - Electro Magnetic Radiation: Update: 2009 - A Study On Cell PhonesDocumento24 pagineEMR - Electro Magnetic Radiation: Update: 2009 - A Study On Cell PhonessmsversuscptNessuna valutazione finora
- Galileo GalileiDocumento3 pagineGalileo GalileiAndrew Paya CañezalNessuna valutazione finora
- Video InglesDocumento2 pagineVideo InglesYeferson Javier Ruiz AriasNessuna valutazione finora
- Beck Protocol HandbookDocumento87 pagineBeck Protocol Handbookzx7blurr6239100% (1)
- Defect Control in SemiconductorsDa EverandDefect Control in SemiconductorsK. SuminoNessuna valutazione finora
- Mod RadDocumento14 pagineMod RadCherry Ann DomingoNessuna valutazione finora
- 1985 John Burnett'Documento24 pagine1985 John Burnett'MariaNessuna valutazione finora
- Robert C Kane Cellular Telephone Russian Roulette PDFDocumento247 pagineRobert C Kane Cellular Telephone Russian Roulette PDFBruno MorinNessuna valutazione finora
- Evolution of Surgical ValvesDocumento8 pagineEvolution of Surgical ValvesvamshidhNessuna valutazione finora
- Mosfet-Introductory Chapter Integrated Circuit ChipDocumento14 pagineMosfet-Introductory Chapter Integrated Circuit Chiphuang kqNessuna valutazione finora
- Lithium-Ion Batteries For Hearing Aid Applications. Part IDocumento12 pagineLithium-Ion Batteries For Hearing Aid Applications. Part ITUNessuna valutazione finora
- Presented By:: V.Sainadha A.SoujanyaDocumento21 paginePresented By:: V.Sainadha A.SoujanyaSadan KumarNessuna valutazione finora
- A First Aid Kit of The FutureDocumento91 pagineA First Aid Kit of The Futureacuario33Nessuna valutazione finora
- Paper Battery 10153 PV8YjqIDocumento17 paginePaper Battery 10153 PV8YjqIMuteeb BandayNessuna valutazione finora
- DR Beck01 PDFDocumento30 pagineDR Beck01 PDFgonzalez1Nessuna valutazione finora
- FAST Test-02 Management PakLearningSpotDocumento24 pagineFAST Test-02 Management PakLearningSpotcodingacademey1Nessuna valutazione finora
- Historia de La CápsulaDocumento9 pagineHistoria de La CápsulaLujan PilarNessuna valutazione finora
- 2012 & Beyond:State-of-the-Art Radiation Monitoring Systems For Nuclear Power Plants and Accelerators - White PaperDocumento14 pagine2012 & Beyond:State-of-the-Art Radiation Monitoring Systems For Nuclear Power Plants and Accelerators - White PaperPennyNessuna valutazione finora
- III-V Semiconductor Materials and DevicesDa EverandIII-V Semiconductor Materials and DevicesNessuna valutazione finora
- Pacemaker BatteriesDocumento12 paginePacemaker Batteriesrohit860Nessuna valutazione finora
- Radiation Physics and Chemistry: Dieter A.E. EhlermannDocumento3 pagineRadiation Physics and Chemistry: Dieter A.E. EhlermannJAIME MEQUIAS AGUILA CRISOLESNessuna valutazione finora
- Electronics: History of Electronics (Week 4)Documento12 pagineElectronics: History of Electronics (Week 4)Nicole Mediodia100% (1)
- Plasma Etching Processes for CMOS Devices RealizationDa EverandPlasma Etching Processes for CMOS Devices RealizationNicolas PossemeNessuna valutazione finora
- Fibre Optics Case ReportDocumento32 pagineFibre Optics Case ReportAman GoelNessuna valutazione finora
- Nanotechnology - TagleDocumento10 pagineNanotechnology - TagleJunary BalasabasNessuna valutazione finora
- Bio Electromagnetic Implications For Health and Healing - Valone 2010Documento6 pagineBio Electromagnetic Implications For Health and Healing - Valone 2010Thomas Valone100% (2)
- How and Why Transistor: Cell Phones ComputersDocumento3 pagineHow and Why Transistor: Cell Phones ComputersimtiazNessuna valutazione finora
- 30 Years - 30 Devices Mddi-10Documento1 pagina30 Years - 30 Devices Mddi-10titov pensezNessuna valutazione finora
- A Seminar Report On Paper BatteryDocumento17 pagineA Seminar Report On Paper BatteryAneeh VermaNessuna valutazione finora
- Band5 - History of EBweldingDocumento97 pagineBand5 - History of EBweldingpiratina33Nessuna valutazione finora
- 40 Years of IsfetDocumento6 pagine40 Years of Isfetsoumendu.bitspNessuna valutazione finora
- The Accelerator Facilities at the Paul Scherrer Institute PSIDa EverandThe Accelerator Facilities at the Paul Scherrer Institute PSINessuna valutazione finora
- Alarm TansistarDocumento18 pagineAlarm TansistarANIL KUMARNessuna valutazione finora
- Infinite Energy Magazine On Cold Fusion by Dr. Eugene MalloveDocumento5 pagineInfinite Energy Magazine On Cold Fusion by Dr. Eugene MalloveWilliam CoteNessuna valutazione finora
- Historical Perspectives of EMGDocumento36 pagineHistorical Perspectives of EMGJacob Tuna NguyenNessuna valutazione finora
- 1 Evaluate The Disclosures in The Notes That Accompany TheDocumento1 pagina1 Evaluate The Disclosures in The Notes That Accompany TheLet's Talk With HassanNessuna valutazione finora
- Discoveries That Would Not Survive The REF: Examples of Curiosity-Driven Discoveries in Different DisciplinesDocumento5 pagineDiscoveries That Would Not Survive The REF: Examples of Curiosity-Driven Discoveries in Different DisciplinesHairyhoundNessuna valutazione finora
- Lecture 2Documento76 pagineLecture 2Nati A. AlemuNessuna valutazione finora
- Our Father Our Father in Heaven, Holy Be Your Name, Your Kingdom Come, Your Will Be Done On Earth As in Heaven. Give Us Today (TDocumento1 paginaOur Father Our Father in Heaven, Holy Be Your Name, Your Kingdom Come, Your Will Be Done On Earth As in Heaven. Give Us Today (TDeepthy GsNessuna valutazione finora
- The MMT Advantage: Important InformationDocumento1 paginaThe MMT Advantage: Important InformationDeepthy GsNessuna valutazione finora
- Led and LaserDocumento60 pagineLed and LaserfiosureshNessuna valutazione finora
- Big Bazaar - Get Home Care & Food Items at Best PricesDocumento1 paginaBig Bazaar - Get Home Care & Food Items at Best PricesDeepthy GsNessuna valutazione finora
- What Are The CBSE Schools With Brilliant Pala - QuoraDocumento1 paginaWhat Are The CBSE Schools With Brilliant Pala - QuoraDeepthy GsNessuna valutazione finora
- Advanced Electronic Communications Systems Wayne Tomasi Sixth EditionDocumento37 pagineAdvanced Electronic Communications Systems Wayne Tomasi Sixth EditionDeepthy GsNessuna valutazione finora
- Frameless Eye Glasses Frames Elastic Mirror Legs For Men and Women - Su - SunglassesCraftDocumento1 paginaFrameless Eye Glasses Frames Elastic Mirror Legs For Men and Women - Su - SunglassesCraftDeepthy GsNessuna valutazione finora
- Frameless Eye Glasses Frames Elastic Mirror Legs For Men and Women - Su - SunglassesMartDocumento1 paginaFrameless Eye Glasses Frames Elastic Mirror Legs For Men and Women - Su - SunglassesMartDeepthy GsNessuna valutazione finora
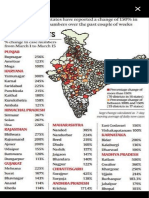
- Maharashtra, Punjab Coronavirus Lockdown News With High Covid-19 Death Rate, Punjab Is Facing A Serious ProblemDocumento1 paginaMaharashtra, Punjab Coronavirus Lockdown News With High Covid-19 Death Rate, Punjab Is Facing A Serious ProblemDeepthy GsNessuna valutazione finora
- Portable Folding Mobile Phone Bracket - MurielthingDocumento1 paginaPortable Folding Mobile Phone Bracket - MurielthingDeepthy GsNessuna valutazione finora
- EC 208 Mod4FMDocumento9 pagineEC 208 Mod4FMDeepthy GsNessuna valutazione finora
- Diode Clipper Circuit - Positive, Negative, Biased, Combination ClipperDocumento1 paginaDiode Clipper Circuit - Positive, Negative, Biased, Combination ClipperDeepthy GsNessuna valutazione finora
- EC 208 Mod4FMDocumento9 pagineEC 208 Mod4FMDeepthy GsNessuna valutazione finora
- Result RETresult RET S2M.Tech Dec2019 PDFDocumento1 paginaResult RETresult RET S2M.Tech Dec2019 PDFDeepthy GsNessuna valutazione finora
- Null PDFDocumento10 pagineNull PDFDeepthy GsNessuna valutazione finora
- Null PDFDocumento10 pagineNull PDFDeepthy GsNessuna valutazione finora
- User Manual 3544119Documento9 pagineUser Manual 3544119Pandit Ramlakhan SharmaNessuna valutazione finora
- Isolation in Electric Vehicle Systems: Quick Reference GuideDocumento12 pagineIsolation in Electric Vehicle Systems: Quick Reference GuideThien Dinh100% (1)
- 1 s2.0 S2352484721008143 MainDocumento9 pagine1 s2.0 S2352484721008143 MainlolNessuna valutazione finora
- Dynamic Model of A Vanadium Redox Flow Battery For System Performance ControlDocumento7 pagineDynamic Model of A Vanadium Redox Flow Battery For System Performance ControlLokesh BaviskarNessuna valutazione finora
- The Reading / Listening - Car Battery - : Paragraph 1Documento2 pagineThe Reading / Listening - Car Battery - : Paragraph 1pedroNessuna valutazione finora
- Tiger: Instrument User Manual V1.8RDocumento58 pagineTiger: Instrument User Manual V1.8RMariana BathistaNessuna valutazione finora
- A User Programmable Battery Charging SystemDocumento5 pagineA User Programmable Battery Charging SystemIonicNessuna valutazione finora
- Eotech Sight ManualDocumento4 pagineEotech Sight ManualArnaldo CentenoNessuna valutazione finora
- Motorola Talkabout Mr350 351 User GuideDocumento5 pagineMotorola Talkabout Mr350 351 User GuideClauLopez99Nessuna valutazione finora
- Manual Perkins 2800 SeriesDocumento122 pagineManual Perkins 2800 SeriesAnonymous tXzjQAJttH100% (1)
- Fluke+PM6685,+PM6685R+Prog +Frequency+Counter PDFDocumento94 pagineFluke+PM6685,+PM6685R+Prog +Frequency+Counter PDFtaryoNessuna valutazione finora
- SURFTEST SJ-301 Series: Portable Surface Roughness TesterDocumento12 pagineSURFTEST SJ-301 Series: Portable Surface Roughness TesterRayuth KEATNessuna valutazione finora
- Futaba 6Xas-6Xhs - Radio Controller User ManualDocumento64 pagineFutaba 6Xas-6Xhs - Radio Controller User Manualrhiu_Nessuna valutazione finora
- Megapack2 SpecificationDocumento20 pagineMegapack2 Specificationpsicodelia2507Nessuna valutazione finora
- Index: Hydraulic ExcavatorDocumento1.886 pagineIndex: Hydraulic ExcavatorChristian Rally Ramos Gonzalez100% (1)
- BT Forklift C3E150 C3E200 C4E150 C4E200 Repair Manual 036 0437 00 (001 250) (001 100)Documento100 pagineBT Forklift C3E150 C3E200 C4E150 C4E200 Repair Manual 036 0437 00 (001 250) (001 100)vladimirNessuna valutazione finora
- Am DDM Ups Rs Aa 0418Documento4 pagineAm DDM Ups Rs Aa 0418aldariz201181Nessuna valutazione finora
- TV0015C WiMon 100 DatasheetDocumento2 pagineTV0015C WiMon 100 DatasheetKonradNessuna valutazione finora
- Description Features: LTC1235 Microprocessor Supervisory CircuitDocumento17 pagineDescription Features: LTC1235 Microprocessor Supervisory Circuitkhawar mukhtarNessuna valutazione finora
- Mercedes Technical Training 318 Ho r230 Dual Battery System 11-28-02Documento3 pagineMercedes Technical Training 318 Ho r230 Dual Battery System 11-28-02gerald100% (34)
- STAGE II, UNIT # 2 (1X600MW) : ProjectDocumento14 pagineSTAGE II, UNIT # 2 (1X600MW) : ProjectRukma Goud ShakkariNessuna valutazione finora
- A World of Minerals in Your Mobile DeviceDocumento2 pagineA World of Minerals in Your Mobile DeviceGeorgeNessuna valutazione finora
- Topic 2-Safe Lab Procedures and Tool Use PDFDocumento24 pagineTopic 2-Safe Lab Procedures and Tool Use PDFPONDRICHE -TICIU CRISTIANNessuna valutazione finora
- Kelio Prio V2 Terminal: InstructionsDocumento20 pagineKelio Prio V2 Terminal: InstructionsdjaaaamNessuna valutazione finora
- MP2636 Datasheet PDFDocumento40 pagineMP2636 Datasheet PDFVinayak SudalaiNessuna valutazione finora
- GFM SeriesDocumento2 pagineGFM SerieswaqasNessuna valutazione finora
- Battery Charger BT-C3100 OPERATING INSTRUCTIONS: 2. Delivery ContentDocumento4 pagineBattery Charger BT-C3100 OPERATING INSTRUCTIONS: 2. Delivery Contentahmad akhyarNessuna valutazione finora
- 42PHW / 42PHQ 42PHQ... K: Owner'S ManualDocumento14 pagine42PHW / 42PHQ 42PHQ... K: Owner'S ManualaaaNessuna valutazione finora
- 2008 Catalog LOISIRS2000Documento24 pagine2008 Catalog LOISIRS20004gen_3Nessuna valutazione finora
- EEC DetroitDocumento92 pagineEEC DetroitRimbert100% (4)