Potrebbero piacerti anche
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (399)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (73)
- 8-Hour Security Guard Training Course OverviewDocumento136 pagine8-Hour Security Guard Training Course OverviewRonald Aranha75% (4)
- DRM The MAKATI WAYDocumento44 pagineDRM The MAKATI WAYjoie gucci100% (1)
- On & Offsite Emergency Plans of FactoriesDocumento19 pagineOn & Offsite Emergency Plans of FactoriesTruth Seeker100% (1)
- Finals Lea4Documento13 pagineFinals Lea4Jennifer PadiernosNessuna valutazione finora
- Letter Invitation Mall Security Officers Table TopDocumento7 pagineLetter Invitation Mall Security Officers Table TopTsoko LeytNessuna valutazione finora
- Quiz Bee ReviewerDocumento1 paginaQuiz Bee Reviewersaquilayan07Nessuna valutazione finora
- Student-Led BRGDDocumento9 pagineStudent-Led BRGDLowel Inciso BorjaNessuna valutazione finora
- Forced Evacuation Plan for Sto. Tomas, PangasinanDocumento21 pagineForced Evacuation Plan for Sto. Tomas, PangasinanFaith Jorie Salinas Leaño-RingorNessuna valutazione finora
- BFP PlanningDocumento60 pagineBFP PlanningChristian Francis Arimado100% (2)
- Approved Manufacturers List - Fire FightingDocumento2 pagineApproved Manufacturers List - Fire FightingAdnan Ahmed KidwaiNessuna valutazione finora
- R04 V-PS Photoelectric Smoke Detector Installation SheetDocumento4 pagineR04 V-PS Photoelectric Smoke Detector Installation SheetDiegoNessuna valutazione finora
- Fire safety regulations and building classificationsDocumento23 pagineFire safety regulations and building classificationskareemulllahNessuna valutazione finora
- Full Download Emergency Care in Athletic Training 1st Edition Grose Test BankDocumento35 pagineFull Download Emergency Care in Athletic Training 1st Edition Grose Test Banksaabatmandearnestus100% (34)
- Abdiqani: Driven by A Vocation To Answer Calls of Distress in MogadishuDocumento3 pagineAbdiqani: Driven by A Vocation To Answer Calls of Distress in MogadishuUNSOM (The United Nations Assistance Mission in Somalia)Nessuna valutazione finora
- Exec. Order 03-19 - BDRRMCDocumento7 pagineExec. Order 03-19 - BDRRMCnorie garcesNessuna valutazione finora
- Blue Modern Geometric Trifold BrochureDocumento2 pagineBlue Modern Geometric Trifold BrochureRommel Coral MonforteNessuna valutazione finora
- Bailan Integrated SchoolDocumento41 pagineBailan Integrated SchoolHanah Joy SucgangNessuna valutazione finora
- FSP-01-FSP 1 PDFDocumento1 paginaFSP-01-FSP 1 PDFsureshkanuboyinaNessuna valutazione finora
- Basic Life Support BLS Acls AtlsDocumento24 pagineBasic Life Support BLS Acls AtlsCaptain AmericaNessuna valutazione finora
- Ayodhya Disaster Management PlanDocumento107 pagineAyodhya Disaster Management PlanHarshita MittalNessuna valutazione finora
- Topic 5. CHAp. 1 Disaster NursingDocumento67 pagineTopic 5. CHAp. 1 Disaster Nursingwinner lovemelovemeNessuna valutazione finora
- Storm Surges Contingency Plan 2022Documento46 pagineStorm Surges Contingency Plan 2022LGU GuimbalNessuna valutazione finora
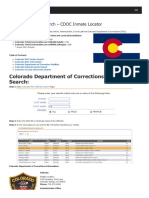
- Colorado Inmate Search Department of Corrections LookupDocumento9 pagineColorado Inmate Search Department of Corrections LookupinmatesearchinfoNessuna valutazione finora
- L.I. 2249 FIRE PRECAUTION (PREMISES) (AMENDMENT) REGULATIONS, 2016 5 Jun 2018Documento8 pagineL.I. 2249 FIRE PRECAUTION (PREMISES) (AMENDMENT) REGULATIONS, 2016 5 Jun 2018유승범Nessuna valutazione finora
- Disaster Laws in Pakistan - Nadeem Ahmed AbroDocumento50 pagineDisaster Laws in Pakistan - Nadeem Ahmed Abroamirbashir24Nessuna valutazione finora
- Fire Truck Inspection Sheet1Documento1 paginaFire Truck Inspection Sheet1Musharaf ShahNessuna valutazione finora
- Defense Support of Civil Authorities (Dsca) : This Briefing IsDocumento15 pagineDefense Support of Civil Authorities (Dsca) : This Briefing IsChris WhiteheadNessuna valutazione finora
- Emergency Fire Drill ScenerionDocumento4 pagineEmergency Fire Drill ScenerionRickz CabaloNessuna valutazione finora
- Key Roles and Responsibilities During Disaster ResponseDocumento10 pagineKey Roles and Responsibilities During Disaster Responserhoy villa bullecerNessuna valutazione finora
- Pinellas County Fire Department Standard Operating Procedures Wildland/urban Interface FiresDocumento46 paginePinellas County Fire Department Standard Operating Procedures Wildland/urban Interface Firesthomasmay1Nessuna valutazione finora