Potrebbero piacerti anche
- Practice Of Osteopathy - Its Practical Application To The Various Diseases Of The Human BodyDa EverandPractice Of Osteopathy - Its Practical Application To The Various Diseases Of The Human BodyValutazione: 5 su 5 stelle5/5 (1)
- Management and Rehabilitation of Spinal Cord InjuriesDa EverandManagement and Rehabilitation of Spinal Cord InjuriesNessuna valutazione finora
- Principles and Management of Acute Orthopaedic Trauma: Third EditionDa EverandPrinciples and Management of Acute Orthopaedic Trauma: Third EditionNessuna valutazione finora
- Art 3Documento17 pagineArt 3ALEJANDRA GARZÓN CUELLAR.Nessuna valutazione finora
- Hydrotherapy Intervention EssayDocumento7 pagineHydrotherapy Intervention EssaymchapeeNessuna valutazione finora
- InterDocumento17 pagineInterNita YulindaNessuna valutazione finora
- A Current Concept Review: Tuberculosis of HipDocumento10 pagineA Current Concept Review: Tuberculosis of HipAnonymous gvVAzlNessuna valutazione finora
- Design The Upper Limb Exoskeleton Arm For Reinforcement The Weakness in The Human MusclesDocumento8 pagineDesign The Upper Limb Exoskeleton Arm For Reinforcement The Weakness in The Human MusclesYASH SANJAY.INGLENessuna valutazione finora
- Releasing Cranial/Dural Strains, Eliminating the Mystique: A Simple, Concise, New TechniqueDa EverandReleasing Cranial/Dural Strains, Eliminating the Mystique: A Simple, Concise, New TechniqueValutazione: 5 su 5 stelle5/5 (1)
- Bhimani - Clinical Understanding of SpasticityDocumento10 pagineBhimani - Clinical Understanding of SpasticityFriendlymeNessuna valutazione finora
- Footsteps towards Mbbs and Higher in Md OphthalmologyDa EverandFootsteps towards Mbbs and Higher in Md OphthalmologyNessuna valutazione finora
- The Inverted Orthotic Technique: A Process of Foot Stabilization for Pronated FeetDa EverandThe Inverted Orthotic Technique: A Process of Foot Stabilization for Pronated FeetNessuna valutazione finora
- Ultrasound Guided Musculoskeletal Procedures in Sports Medicine: A Practical AtlasDa EverandUltrasound Guided Musculoskeletal Procedures in Sports Medicine: A Practical AtlasValutazione: 5 su 5 stelle5/5 (1)
- 173 184Documento12 pagine173 184yu prdnyaNessuna valutazione finora
- Proximal Hamstring Tears: From Endoscopic Repair to Open ReconstructionDa EverandProximal Hamstring Tears: From Endoscopic Repair to Open ReconstructionThomas YoumNessuna valutazione finora
- Hand Conditions and Examinations: a Rheumatologic and Orthopaedic ApproachDa EverandHand Conditions and Examinations: a Rheumatologic and Orthopaedic ApproachNessuna valutazione finora
- 1640954667jmpas November-December 2021Documento3 pagine1640954667jmpas November-December 2021asmaNessuna valutazione finora
- MRI of Degenerative Disease of the Spine: A Case-Based AtlasDa EverandMRI of Degenerative Disease of the Spine: A Case-Based AtlasNessuna valutazione finora
- Efficacy of Nerve Flossing Technique On Improving Sciatic Nerve Function in Patients With Sciatica - A Randomized Controlled TrialDocumento10 pagineEfficacy of Nerve Flossing Technique On Improving Sciatic Nerve Function in Patients With Sciatica - A Randomized Controlled Trialsphadungkit100% (1)
- IOT Based Wireless Monitoring Stroke Patient With Partial Paralysis AssistanceDocumento7 pagineIOT Based Wireless Monitoring Stroke Patient With Partial Paralysis AssistanceAzmi AbdulbaqiNessuna valutazione finora
- Jurnal 1Documento15 pagineJurnal 1Yusuf WildanNessuna valutazione finora
- Foot and Ankle Instability: A Clinical Guide to Diagnosis and Surgical ManagementDa EverandFoot and Ankle Instability: A Clinical Guide to Diagnosis and Surgical ManagementNessuna valutazione finora
- Removable Myofunctional Appliances: An OverviewDocumento20 pagineRemovable Myofunctional Appliances: An OverviewIJAR JOURNALNessuna valutazione finora
- Thesis About ArthritisDocumento5 pagineThesis About ArthritisVicki Cristol100% (2)
- RJMEarticolDocumento11 pagineRJMEarticolOvidiuNessuna valutazione finora
- Mastering Flexibility With Scientific Protocols - Based On The Teachings Of Dr. Andrew Huberman: Optimize Flexibility Using Evidence-Backed Stretching TechniquesDa EverandMastering Flexibility With Scientific Protocols - Based On The Teachings Of Dr. Andrew Huberman: Optimize Flexibility Using Evidence-Backed Stretching TechniquesNessuna valutazione finora
- Looking Back: Some Reflections on the Prevention and Treatment of Low Back PainDa EverandLooking Back: Some Reflections on the Prevention and Treatment of Low Back PainNessuna valutazione finora
- Physiotherapy Treatment in Plantar Fasciitis: A Case Report: January 2015Documento6 paginePhysiotherapy Treatment in Plantar Fasciitis: A Case Report: January 2015ayuNessuna valutazione finora
- Assessment of Rotator Cuff Muscle Strength and Shoulder Rotation Range of Motion in Subjects With Lateral EpicondylitisDocumento5 pagineAssessment of Rotator Cuff Muscle Strength and Shoulder Rotation Range of Motion in Subjects With Lateral Epicondylitispedrovsky702Nessuna valutazione finora
- Knee Meniscus (Cartilage) Tears: Everything You Need to Know to Make the Right Treatment Decision: - What the meniscus does and why it is so important - Treatment options for meniscus tears - Surgery: repair, removal, transplantation - How to prepare for surgery - What to do the first week after suDa EverandKnee Meniscus (Cartilage) Tears: Everything You Need to Know to Make the Right Treatment Decision: - What the meniscus does and why it is so important - Treatment options for meniscus tears - Surgery: repair, removal, transplantation - How to prepare for surgery - What to do the first week after suValutazione: 4 su 5 stelle4/5 (1)
- Arthritis and Society: The Impact of Musculoskeletal DiseasesDa EverandArthritis and Society: The Impact of Musculoskeletal DiseasesNessuna valutazione finora
- Subjective: The PatientDocumento2 pagineSubjective: The PatientRoscoe ParaanNessuna valutazione finora
- Ultrasound Anatomy of Lower Limb Muscles: A Practical GuideDa EverandUltrasound Anatomy of Lower Limb Muscles: A Practical GuideNessuna valutazione finora
- BartenDocumento178 pagineBartenAndreutza DeutzaNessuna valutazione finora
- Artikel 5 Siap TerbitDocumento11 pagineArtikel 5 Siap TerbitbintangmihanNessuna valutazione finora
- Anthony JP Mathes SJ: SourceDocumento4 pagineAnthony JP Mathes SJ: SourcekramierNessuna valutazione finora
- Everything You Ever Wanted to Know about Shoulder, Hip and Knee Arthritis, but Didn’t Know What to AskDa EverandEverything You Ever Wanted to Know about Shoulder, Hip and Knee Arthritis, but Didn’t Know What to AskNessuna valutazione finora
- Influence of Myofacial Release and Stretching To Relieve Spasticity in Patients With Stroke - A Systematic ReviewDocumento5 pagineInfluence of Myofacial Release and Stretching To Relieve Spasticity in Patients With Stroke - A Systematic ReviewInternational Journal of Innovative Science and Research TechnologyNessuna valutazione finora
- Ergonomics in Endodontics-A ReviewDocumento5 pagineErgonomics in Endodontics-A ReviewIJAR JOURNALNessuna valutazione finora
- 17 Kasimis Original 14 1Documento8 pagine17 Kasimis Original 14 1Maria Alejandra Garcia QuirogaNessuna valutazione finora
- Emergency Musculoskeletal Imaging in ChildrenDa EverandEmergency Musculoskeletal Imaging in ChildrenNessuna valutazione finora
- Hyun-Yoon Ko - Management and Rehabilitation of Spinal Cord Injuries-Springer (2022)Documento915 pagineHyun-Yoon Ko - Management and Rehabilitation of Spinal Cord Injuries-Springer (2022)JESSICA OQUENDO OROZCONessuna valutazione finora
- NMDs NCBIDocumento7 pagineNMDs NCBIFelicia PanditaNessuna valutazione finora
- Artikel 5 Siap TerbitDocumento11 pagineArtikel 5 Siap Terbithobi kitaNessuna valutazione finora
- Shull 2015Documento13 pagineShull 2015Fernando Mauricio GomezNessuna valutazione finora
- Dislocation of the Temporomandibular Joint: A Guide to Diagnosis and ManagementDa EverandDislocation of the Temporomandibular Joint: A Guide to Diagnosis and ManagementNigel Shaun MatthewsNessuna valutazione finora
- Entrapment Neuropathy of the Lumbar Spine and Lower LimbsDa EverandEntrapment Neuropathy of the Lumbar Spine and Lower LimbsToyohiko IsuNessuna valutazione finora
- Spinal Interneurons: Plasticity after Spinal Cord InjuryDa EverandSpinal Interneurons: Plasticity after Spinal Cord InjuryLyandysha Viktorovna ZholudevaNessuna valutazione finora
- Ojsadmin, 4Documento5 pagineOjsadmin, 4janeNessuna valutazione finora
- Congenital Swan Neck Deformity: A Case Report and Review of LiteratureDocumento4 pagineCongenital Swan Neck Deformity: A Case Report and Review of LiteratureIJAR JOURNALNessuna valutazione finora
- Rehabilitation ParesisDocumento12 pagineRehabilitation ParesisanjelikaNessuna valutazione finora
- Roods ApproachDocumento23 pagineRoods ApproachyigoNessuna valutazione finora
- Excessive Genu Valgum FINALDocumento13 pagineExcessive Genu Valgum FINALMeeraNessuna valutazione finora
- Achilles TendonDocumento30 pagineAchilles TendonBetoNessuna valutazione finora
- Types of StretchingDocumento7 pagineTypes of StretchingaaronmgriffinNessuna valutazione finora
- Femorals PDFDocumento145 pagineFemorals PDFnoronisa talusobNessuna valutazione finora
- Sex Differences in Muscle Morphology of The Knee Flexors and Knee ExtensorsDocumento15 pagineSex Differences in Muscle Morphology of The Knee Flexors and Knee ExtensorsGvidas MikalauskasNessuna valutazione finora
- Management of Bilateral Patellar Luxation in An AlpacaDocumento6 pagineManagement of Bilateral Patellar Luxation in An AlpacaCássia DepetrisNessuna valutazione finora
- PresjurDocumento18 paginePresjurIhsanNessuna valutazione finora
- Abductor Digiti Minimi KT MethodDocumento2 pagineAbductor Digiti Minimi KT MethodFlorin ArdeleanuNessuna valutazione finora
- Perineum: Dr. Edi Patmini SS, Spog/Dr. M. Nurhadi Rahman, SpogDocumento16 paginePerineum: Dr. Edi Patmini SS, Spog/Dr. M. Nurhadi Rahman, Spogpuskesmas gebangNessuna valutazione finora
- Stewart Ortho TractionDocumento99 pagineStewart Ortho TractionOliverNessuna valutazione finora
- Oia Rabbit PDFDocumento13 pagineOia Rabbit PDFJhoanna Rein DuzonNessuna valutazione finora
- Lumbar HyperlordosisDocumento13 pagineLumbar HyperlordosisAdriana Lucia Martinez CastillaNessuna valutazione finora
- Low Back Program ExercisesDocumento8 pagineLow Back Program ExercisesKarthik AnantharamuNessuna valutazione finora
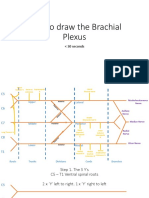
- How To Draw The Brachial PlexusDocumento16 pagineHow To Draw The Brachial PlexusHNessuna valutazione finora
- Śrī Devī Kha GamālārcanamDocumento8 pagineŚrī Devī Kha GamālārcanamnjaykumarNessuna valutazione finora
- Reviewing Your Knowledge - Ex14Documento3 pagineReviewing Your Knowledge - Ex14maydelin50% (2)
- 04.gluteal RegionDocumento47 pagine04.gluteal RegionLavanya SivakumarNessuna valutazione finora
- Splint Fabrication Evaluation FormDocumento14 pagineSplint Fabrication Evaluation FormJess QuickNessuna valutazione finora
- Done - EDITED-HOPE1 q1 Mod5 ObservesPersonalSafetyProtocolDocumento21 pagineDone - EDITED-HOPE1 q1 Mod5 ObservesPersonalSafetyProtocolVivencio Pascual JrNessuna valutazione finora
- Anatomy FlashcardsDocumento70 pagineAnatomy Flashcardskori holubNessuna valutazione finora
- Orthopedic History and Physical ExaminationDocumento5 pagineOrthopedic History and Physical Examinationati sulNessuna valutazione finora
- Peripheral Vascular AssessmentDocumento14 paginePeripheral Vascular AssessmentgireeshsachinNessuna valutazione finora
- 50 Easy Things: That Will Actually Improve Your PostureDocumento33 pagine50 Easy Things: That Will Actually Improve Your PostureSteven HowellNessuna valutazione finora
- Excellent Neck Exercises Are The Secret of Getting Neck Pain Relief - DR LumbagoDocumento5 pagineExcellent Neck Exercises Are The Secret of Getting Neck Pain Relief - DR LumbagoasfagahNessuna valutazione finora
- Kosti - Opći PojmoviDocumento1 paginaKosti - Opći Pojmovibotoks uwuNessuna valutazione finora
- Clinical Implications of Scapular Dyskinesis in Shoulder Injury - The 2013 Consensus Statement From The 'Scapular Summit'Documento13 pagineClinical Implications of Scapular Dyskinesis in Shoulder Injury - The 2013 Consensus Statement From The 'Scapular Summit'杨钦杰Nessuna valutazione finora
- Basic Taping GuideDocumento2 pagineBasic Taping GuideChirvas VeronicaNessuna valutazione finora
- Female Pelvis-Clinical AnatomyDocumento24 pagineFemale Pelvis-Clinical Anatomyshubha lNessuna valutazione finora
- Ejercicios Con Gomas Water PoloDocumento5 pagineEjercicios Con Gomas Water PoloEl Cuervo Waterpolo100% (1)
- Anatomy of KneeDocumento28 pagineAnatomy of KneeManish AdhikariNessuna valutazione finora