Documenti di Didattica
Documenti di Professioni
Documenti di Cultura
SC Ethiopia
Caricato da
simbiroTitolo originale
Copyright
Formati disponibili
Condividi questo documento
Condividi o incorpora il documento
Hai trovato utile questo documento?
Questo contenuto è inappropriato?
Segnala questo documentoCopyright:
Formati disponibili
SC Ethiopia
Caricato da
simbiroCopyright:
Formati disponibili
Request to USAID/OFDA for a
New Award or
Modification to an Existing Award (#_________)
Applicant Organization Name: Save the Children Federation, Inc.
Headquarters Contact Information Field Contact Information
Contact Person: Greg Ramm Ashebir Debebe
VP, Humanitarian Response Deputy Country Director, Program
Development & Quality
Mailing Address:
899 North Capitol Street, #900 P.O. Box 387
Washington, DC 20002 Addis Ababa
USA Ethiopia
Telephone: +1 (202) 794-1506 +251 (0) 113710972
Country/Region of Country: Ethiopia/Oromia and Somali Regions
Email: gramm@savechildren.org Ashebir.Debebe@savethechildren.org
Submission/Revision Date: 3 April 2019
Program Title: Emergency WASH and Nutrition response for conflict affected IDPs and host
communities in Dawa, Shebelle, Korahe Zones, of Somali and Bale Zone of Oromia Regions
Proposed Start Date: 1 March 2019
Proposed Program Duration: 10 months
Check boxes below if your proposal requests USAID/OFDA funding for procurement of the
following categories of restricted goods:
Restricted Goods
☐ Seeds*
☐ Livestock*
☐ Fertilizer
-1-
Save the Children | Emergency WASH and Nutrition response to conflict affected IDPs and host communities in
Dawa, Shebelle, Korahe Zones, of Somali and Bale Zone of Oromia Regions
Submission Date: 03 April 2019
☐ Pesticides and Pesticide-containing Materials, including LLINs, ITPSs**
☐ Pharmaceuticals: Human**
☐ Pharmaceuticals: Veterinary**
☒ Purchase of vehicles not manufactured in the U.S. or leases greater than 180 days
☐ Used Equipment
☐ USG-owned Excess Property
Dollar Amount Requested from USAID/OFDA $ 3,000,000
Dollar Amount from Other Sources: Not Applicable.
Dollar Value of In-kind Contributions: Not Applicable.
Total Dollar Amount of Program: $ 3,000,000
Program Goal: To save lives and prevent suffering of conflict affected internally displaced people
and host communities, children and their families in Oromia and Somali Regions.
Total Number of People Affected in the Target Area:
o Somali Region: 1,799,6791
o Oromia Region: 3,240,3852
Total Number of People Targeted (Individuals):
o Somali Region: 45,632
o Oromia Region: 10,919
Total Number of Internally Displaced Persons (IDP) Targeted (Individuals) as subset
of above: 30,000 (14,700 F: 15,300 M)
Executive Summary:
1 Figures taken from Mid-Year revised Humanitarian Disaster and Resilience Plan
2 Ibid
-2-
Save the Children | Emergency WASH and Nutrition response to conflict affected IDPs and host communities in
Dawa, Shebelle, Korahe Zones, of Somali and Bale Zone of Oromia Regions
Submission Date: 03 April 2019
Conflict, population displacement and natural disasters have resulted in a major humanitarian
crisis in Ethiopia. Close to 3 million people have fled inter-communal violence and conflict. In
addition, the country is recovering from two successive droughts, an estimated 7.8 million people
are in need of emergency food assistance, in addition to 7.9 million (41.6 Million MAM and
370,000 SAM cases) that are considered chronically vulnerable. The revised mid-year
Humanitarian Disaster and Resilience Plan (HDRP) projects that some 8 million people will
continue to receive humanitarian assistance in 2019, requiring US $1.2 billion. The proposed
project is planned to be implemented in 15 hot spot woredas (five woredas of Oromia Region and
ten woredas of Somali Region).
The primary objective of the program is to provide lifesaving emergency Water, Sanitation, and
Hygiene (WASH), and Nutrition assistance for vulnerable and critically affected IDP children and
families. The Nutrition component of the project will be implemented in all 15 priority one woredas
of Somali and Oromia region and will focus on: prevention and treatment of Severe Acute
Malnutrition (SAM) and Moderate Acute Malnutrition (MAM) in children under five and pregnant
and lactating women; improving Infant and Young Child Feeding in Emergencies (IYCF-E); and,
supporting sustained behaviour change. To respond to the WASH needs in Korahe zone of
Somali region, and Bale zone of Oromia region. WASH activities will focus on providing life-saving
and sustainable WASH support to the affected population in the proposed areas. Save the
Children (SC) will ensure children and families have increased access to safe water in terms of
quality and quantity and safe excretal disposal facilities in order to reduce the risks of water borne
diseases. Save the Children will also distribute hygiene kits to SAM children and vulnerable IDP
families. To strengthen and sustain the impact of WASH activities, SC will train volunteers and
WASH Committees (WASHCOs), and raise the targeted communities’ awareness of key risk
behaviors, through hygiene promotion awareness campaigns.
-3-
Save the Children | Emergency WASH and Nutrition response to conflict affected IDPs and host communities in
Dawa, Shebelle, Korahe Zones, of Somali and Bale Zone of Oromia Regions
Submission Date: 03 April 2019
Sector Table:
Sector Name: Water, Sanitation, and Hygiene (WASH)
To increase access to safe drinking water, sanitation and to
Objective: improve hygiene practices at health facilities, nutrition
centers and IDP sites
Dollar Amount Requested: $863,662 USD
Number of
52,500 (25,725 F, 26,775 M)
People Targeted:
Number of IDPs Targeted: 30,000 (14,700 F, 15,300 M)
8 woredas in Oromia and Somali Regions
Somali (3)– Shilabo, Dobowein and Kebridahar woredas in
Korahe zone
Geographic Area(s):
Oromia (5) – Sewena, Dawaketchen, Rayitu, Legahida and
Guradamole woredas in Bale zone
Keyword(s): WASH in Health Facilities
Sub-sector Name: Water supply
Number of people directly utilizing improved water services
Indicator 1:
provided with OFDA funding
Percent of households receiving point-of-use chlorine
Indicator 2: products whose water supplies have free residual chlorine
(FRC) present
Percent of water points repaired or rehabilitated with free
Indicator 3:
residual chlorine (FRC) > 0.2 mg/L
Custom Indicator (4): Number of water points repaired or rehabilitated
-4-
Save the Children | Emergency WASH and Nutrition response to conflict affected IDPs and host communities in
Dawa, Shebelle, Korahe Zones, of Somali and Bale Zone of Oromia Regions
Submission Date: 03 April 2019
Sub-sector Name: Sanitation
Number of people directly utilizing improved sanitation
Indicator 1:
services provided with OFDA funding
Percent of households targeted by latrine
Indicator 2: construction/promotion program whose latrines are
completed and clean
Indicator 3: Average number of users per functioning toilet
Number of Gender separated latrine with hand washing
Custom Indicator (4):
facility constructed
Sub-sector Name: Hygiene Promotion
Number of people receiving direct hygiene promotion
Indicator 1: (excluding mass media campaigns and without double-
counting)
Percent of households targeted by the hygiene promotion
Indicator 2: program who store their drinking water safely in clean
containers
Percent of people targeted by the hygiene promotion who
Indicator 3: know at least three (3) of the five (5) critical times to wash
hands
Custom Indicator (4): Number of health facilities received WASH cleaning supplies
Sub-sector Name: WASH Non-food Items
Total number of people receiving WASH NFIs assistance
Indicator 1:
through all modalities (without double-counting)
Percent of households reporting satisfaction with the
Indicator 2: contents of the WASH NFIs received through direct
distribution
Percent of households reporting satisfaction with the quantity
Indicator 3:
of WASH NFIs received through direct distribution
Custom Indicator (4): Number of WASH NFI kit distributed
-5-
Save the Children | Emergency WASH and Nutrition response to conflict affected IDPs and host communities in
Dawa, Shebelle, Korahe Zones, of Somali and Bale Zone of Oromia Regions
Submission Date: 03 April 2019
Sector Name: Nutrition
To provide curative and preventive nutrition interventions to
Objective: children under 5 years of age and pregnant and lactating
women (PLW), delivered through government systems
$2,136,339 USD
Dollar Amount Requested:
Number of 56,551 (36,685 U5, 19,866 PLW), Total SAM-2,402 (482 at
SC and 19,820 in OTPs), Total MAM – 56,551 (36,685 U5,
People Targeted: 19,866 PLW)
13,945 (9,204 U-5 and 4,741 PLW)
Number of IDPs Targeted:
Oromia (5) – Rayitu, Dawa Kechene, Legahida, Guradamole
and Sewena
Geographic Area(s):
Somali (10) – Moyale, Hudet, Kededum, Mubarek (Dawa
Zone), Keberidehar, Shilabo and Debiwoyen (Korahe Zone),
Kelafo, Mustahil and Ferfer (Shebelle Zone)
Keyword(s): Pastoralists
Sub-sector Name: Infant and Young Child Feeding in Emergencies (IYCF-E)
Proportion of infants 0-5 months of age who are fed
Indicator 1:
exclusively with breast milk
Proportion of children 6-23 months of age who receive foods
Indicator 2:
from 4 or more food groups
Number of people receiving behavior change interventions to
Indicator 3:
improve infant and young child feeding practices
-6-
Save the Children | Emergency WASH and Nutrition response to conflict affected IDPs and host communities in
Dawa, Shebelle, Korahe Zones, of Somali and Bale Zone of Oromia Regions
Submission Date: 03 April 2019
Number of mother to mother support groups (MtMSGs)
Custom Indicator (4):
established/strengthened and supported
Custom Indicator (5): Number of breastfeeding corners established and supported
Sub-sector Name: Management of Acute Malnutrition
Number of health care staff trained in the prevention and
Indicator 1:
management of acute malnutrition
Indicator 2: Number of supported sites managing acute malnutrition
Number of people admitted, rates of recovery, default, death,
Indicator 3: relapse, and average length of stay for people admitted to
Management of Acute Malnutrition sites
Number of people screened for malnutrition by community
Indicator 4:
outreach workers.
Number of woreda health offices supported with supply
Custom Indicator (5):
chain and nutrition information management
A. Justification
1. Problem Statement
Oromia Region
- Water Hygiene & Sanitation (WASH)
There are six zones of Oromia with high populations of IDPs (East Harerge, West Harerge, Bale,
Borena, Guji and West Guji) across the country. This intervention will focus on Bale zone which
is currently hosting a total of 22,670 displaced HHs. The five target woredas of Lega Hida,
Sawena, Rayitu, Gura Damole and Dawe Kachen are among the top conflict and drought affected
woredas, in which more than 50% (65,918) of all IDPs across 20 IDP sites/kebeles, are settled
in. Based on the 2018 hot spot prioritization, the five target Woredas are priority one woredas,
where rainfall distribution is below optimal and household food insecurity continues to be
challenging. The mid-year HDRP report indicates that about 4.09 million people in Oromia region
will require WASH assistance.
- Health and Nutrition
-7-
Save the Children | Emergency WASH and Nutrition response to conflict affected IDPs and host communities in
Dawa, Shebelle, Korahe Zones, of Somali and Bale Zone of Oromia Regions
Submission Date: 03 April 2019
Oromia is also one of the region with high projected SAM and MAM cases (139,000 and 1,329,995
respectively).3 Based on monitoring reports conducted by SC, in the target woredas of Bale Zone,
IDPs continue to experience limited access to health and nutrition services. In the target woredas,
malnutrition rates continue to be alarming, based on the recent screening data (Jun-Aug, 2018),
in the five target woredas among a total 9,579-screened (5,072 PLW, 4,507 children) 4,507 MAM
and 147 SAM cases were found. This translates to over 3% of the screened children being
severely malnourished, thus facing the highest risk of mortality. Irregular TSFP commodity
distribution by government (food distribution is currently conducted to IDP sites by Government
with frequent pipeline breaks from WFP), remoteness and poor road infrastructure, lack of
resettlement and limited government capacity to provide basic health and nutrition services at IDP
sites continues to be a major challenge demanding the continued support of partners to address
the immediate needs of IDPs in the woredas
Somali Region
According to Somali region DTM round 13, a total of 1,016,166 displaced individuals comprising
of 168,246 HHs in 388 displacement sites were identified in Somali region. A total of 59.54% of
the IDP sites were opened in 2017, and 13.14% were opened in 2018. Conflict was the primary
cause of displacement for an estimated 65.45% of the displaced population.
- Water Hygiene & Sanitation (WASH)
Only four sites meet SPHERE standards of access to over 15 liters of water per person per day
and 241 (62.11%) displacement sites reported having no latrines. The Gu assessment further
indicates high levels of food insecurity in rural areas, acute water shortage and loss of livelihoods.
Despite good performance of the Gu rains, water shortage continues to be a major problem in the
zones due to limited sustainable water sources. In the three target woredas in Korahe zones,
water and sanitation is below the national average.
- Health and Nutrition
Somali region is also one of the region with high projected SAM and MAM cases (99,000 and
901,145 respectively).4 According to the Dehre assessment report and field mission report
conducted by Save the Children (Sep, 2018), in Hudet and Moyale woredas, of a total of 13 health
facilities (eight in Hudet Woreda and five in Moyale woreda), 12 are non-functional, burnt and only
one health post is functional, providing basic health and nutrition services. The context is also
similar in Mubarek and Kededuma, in which the existing five functional but poorly resourced,
health centers are expected to deliver lifesaving health and nutrition services to nearly 200,000
IDP and host community members.
3 HDRP midyear report 2018.
4 HDRP Midyear Report 2018
-8-
Save the Children | Emergency WASH and Nutrition response to conflict affected IDPs and host communities in
Dawa, Shebelle, Korahe Zones, of Somali and Bale Zone of Oromia Regions
Submission Date: 03 April 2019
In addition, the routine screening report reveals that a nearly 10% increment was observed in
SAM admission in target woredas of Korhae and Shebelle as compared to the previous year. This
is due to the massive loss of animals during the last drought. The animal population has
significantly reduced leaving households with only a few heads that are not able to produce the
milk required by the family. With the current Deyr rains appearing to have totally failed, it is
expected that cases of malnutrition will rise in the coming couple of months due to the dry spell
ahead until the coming Gu rains that are expected in April 2019 and the decrease in the amount
of milk production of livestock which are a key source of food for pastoralist children. Based on
the report from regional health bureau, the political instability that occurred in August 2018 in the
Somali region has had a huge impact on the existing health system in terms of staffing. There has
been high turnover of non-Somali staffs who had been working in Shabele and Korahey zones
particularly the six target woredas (Kalafo, Mustahil, Ferfer, Kabridahar, Shilabo and Doboweyn).
A total of 47 health professionals including doctors, nurses and health officers have left these
woredas following the incident. This has further weakened the capacity of government to provide
health and nutrition services in the target woredas.
The political unrest and subsequent instability across Somali Region has significantly hampered
the emergency response, with high government turnover, NGO temporary withdrawal impacting
on the service provision for communities where acute malnutrition remains very high (HDRP,
2018). For instance, from the 296 health workforce in the proposed four woredas, more than 50
health professionals left the woredas due to insecurity caused by the recurrent conflict. For more
than one year, WFP did not manage to deliver needed food distributions to Dawa Zone due to an
unstable security situation and ongoing access challenges in the area. There was an interruption
of TSFP food supplies for treatment of MAM in Dawa zone for more than six months, which
contributed to a further deterioration of nutrition status among the most vulnerable children and
women, specifically in the proposed four woredas. As such, the trend of acute malnutrition is
sharply rising as compared to this time of year in 2017. From March to October 2018, SAM cases
increased by 41%, compared to 2017 (Mar-Oct, 2017).5 Inpatient (SC) and outpatient (OTP)
admission for SAM management also increased by 41% and 60% respectively comparing to 2017
in the same months. Based on the routine screening report in the last 8 months of 2018, the
nutritional status in the six target woredas of Korahe and Shebele Zones continues to be alarming,
the proxy GAM ranging from 21-29%. Recent OTP and SC admission data shows the trend of
acute malnutrition is expected to increase by 11% and will remain a major concern exacerbated
by ongoing measles outbreaks in nearly all of the target woredas.
Justification for Intervention and Needs Assessment Summary
Needs Assessment Summary – Oromia
Sector: WASH
5 SC’s assessment report finding conducted in October 2018
-9-
Save the Children | Emergency WASH and Nutrition response to conflict affected IDPs and host communities in
Dawa, Shebelle, Korahe Zones, of Somali and Bale Zone of Oromia Regions
Submission Date: 03 April 2019
Sub-sector: Water Supply
According to the WASH cluster, rainfall in Bale was lower than expected, with only rain showers
in some areas, with widespread fear of water shortage in the coming months in most lowland
woredas. A total of 22,670 displaced HHs living in eight woredas of Bale zone are receiving below
five liter/sec/person/day and predominantly relying on river water. In addition, a recent
assessment conducted by Save the Children shows that health facilities are located 2-5km from
available water sources. Some IDP sites also lack water and sanitation services. As per
International Rescue Committee’s (IRC) recent assessment in the majority of the targeted
woredas there is highly need in of water trucking specially at health facilities where there is no
reliable source. The Zonal water office also requested support from SC for water rationing for
emergency especially at Health institution. Moreover, a total of 1,608,501 individuals are affected
with 231,577 individuals at risk of WASH related emergency in the coming dry month in more than
845 kebeles of 53 woredas of the region.
The need for rehabilitating non-functional water supply systems including provision of water
trucking is critically needed in priority locations. Lack of potable water supply in majority of health
facilities that provide SC and OTP services had compromised and compounded the problem in
the zones. Moreover, during the kebele-level assessments held by IRC in the month of November
2018, WASH related disease such as diarrhea and pneumonia is the most common top five
disease in the assessed woredas. The report highlighted that the number of non-functional
borehole are aggravated by IDPs from the Somali border sharing the same water resource with
poor performance and inadequate amount. This affects the water availability for human and
livestock consumption in particular with limitation of the water sources obliged deployment of
water trucks serving IDPs 22,376 people in Dawe Serar, 7,286 in Rayitu, 26,530 in LegaHida and
10,834 in Sewena woredas. Currently IRC has deployed four water trucks in three intervention
woredas, two trucks in Dawe Serar, one truck in Legahida and one truck in Rayitu and serving
the IDPs but no partner is working for institutions including in health facilities and schools.
Sub-sector: Sanitation
The assessment also notes that open defecation is widely practiced, thereby increasing the risk
of diarrheal diseases. Moreover, in some IDP sites, scabies is reported, requiring immediate
intervention. Regarding sanitation support for IDPs in Bale, IRC in collaboration with a
Government partner have carried out latrine construction in all IPD sites in Sewena, Rayitu,
Legehida woredas, and the existing health facilities have latrine facilities.
Sub-sector: Hygiene Promotion
- 10 -
Save the Children | Emergency WASH and Nutrition response to conflict affected IDPs and host communities in
Dawa, Shebelle, Korahe Zones, of Somali and Bale Zone of Oromia Regions
Submission Date: 03 April 2019
According to SC’s assessment conducted in each of the targeted woredas, and focus group
discussion with the beneficiary communities, the need for continued hygiene promotion is clear.
Due to the practice of open defecation in the area, when the rainy season begins, excrement is
washed away and enters the water source (Adele stream), frequently causing diarrheal disease
among children, and itching while using the water for body washing. Hence, poor hygiene
practice, low latrine coverage and utilization, diarrheal diseases, and shortage or absences of
safe drinking water at IDPs site and local community are some of the major health concerns and
risk factors, which require awareness raising in the community.
Sub-sector: WASH NFI
According to IRC, no relevant programming related to WASH NFIs are currently ongoing in terms
of menstruation hygiene management for women, and provision of hygienic kit including water
treatment chemicals, especially for health institution is also identified gap during the assessment.
Sector: Nutrition
Sub-Sector: Infant and Young Child Feeding and Behavior Change
Based on the Last E-DHS 2016, the medial period for exclusive breastfeeding in Oromia region
is estimated to be 2.8 months. Household burdens on mothers, limited knowledge and practices
about the importance of breastfeeding are the top reasons for shorter period of breastfeeding
practice by mothers. In addition, the survey also indicated that only 16.9% children have the
minimum acceptable diversified meals and only 9.6% children have a minimum acceptable diets.
The long and sustained displacement in the region coupled with limited health and nutrition
services and unavailability of appropriate foods for infants and young children in the target
woredas has led to increased vulnerability to undernutrition, disease and death. Additionally, sub-
optimal care practices like mixed feeding; early introduction of complementary foods and poor
hygiene and sanitation has led to widespread inappropriate infant and young child feeding
practices in the target woredas. The risks associated with these practices further aggravates the
health and nutritional status of these communities, especially amongst the IDP population.
Sub-sector: Management of Acute Malnutrition
Based on monitoring reports conducted by SC, in the target woredas of Bale Zone, IDPs continue
to experience limited access to health and nutrition services. Based on the 2018 hot spot
prioritization, the five target woredas are priority are woredas and rainfall distribution is below
optimal while household food insecurity continuous to be challenging. In the target woredas,
malnutrition rates continue to be alarming; based on the recent screening data (Jun-Aug, 2018),
in the five target woredas among a total screened 9,579 (5,072 PLW, 4,507children) 4,507 MAM
and 147 SAM cases were found. This translates to over 3% of the screened children being
- 11 -
Save the Children | Emergency WASH and Nutrition response to conflict affected IDPs and host communities in
Dawa, Shebelle, Korahe Zones, of Somali and Bale Zone of Oromia Regions
Submission Date: 03 April 2019
severely malnourished, thus facing the highest risk of mortality. Irregular TSFP commodity
distribution by government (food distribution is currently conducted to IDP sites by Government
and there were frequent pipeline breaks from WFP’s side), remoteness and poor road
infrastructure, lack of resettlement and limited government capacity to provide basic health and
nutrition services at IDP sites continues to be a major challenge demanding the continued support
of partners to address the immediate needs of IDPs in the woredas.
Needs Assessment Summary – Somali
Sector: WASH
Sub-sector: Water Supply
According to the deyr assessment, deyr rainfall in the region was reported to have been
characterized by late onset, erratic, localized, low in amount and duration, low frequency, non-
uniform distribution and unsatisfactory across the region and the rain received was unable to
recover the required water intervention. The lack of access to safe drinking water is already
evident in most woredas across the zones, largely due to the poor rain performance, limited water
sources and non-functionality of water schemes. Most areas are already in a serious water stress
situation and require urgent water trucking interventions to alleviate suffering during the long and
hard dry season period and to avert the possibility of outbreak of communicable diseases such
as AWD. The findings by the assessment team following interviews and observations indicate
that a total of 1,328,586 people will face acute shortages of water from December 2018 through
April 2919 in 610 sites across 79 woreda in Somali region including Korahe zone. Of those facing
water shortages, 52% need urgent water trucking arrangements to alleviate suffering and
potential risk of immigration to other areas deemed having potential for good water availability. Of
major concerns and most vulnerable populations are in those Woredas inhabited by IDPs who
generally have very limited access to basic services and with limited options and hence less
chances for coping with water stress.
According to the Gu assessment, the population in Korahe zone facing water shortages as of
August 2018 is estimated at 206,500 persons located in 75 kebeles of Korahe zone. Waterborne
diseases could erupt again in Korahe zone at any time owing to low coverage of safe drinking
water. There are 30 motorized boreholes in Korahe zone of which six are currently nonfunctional.
Similarly, out of 22 earth dams only 11 are currently holding some water from the recent Gu rain.
The unavailability of permanent water supply system in Korahe zone to the level required makes
the area vulnerable to water shortages even after good rains are received. In terms of coverage,
the water coverage in Kebridehar woreda is estimated to be 30%, 31% in Shilabo, 29% in
Dobewain, from observations and discussions with local authorities and community elders. The
assessment concluded shows that some 206,500 persons in Korahe zone might face water
shortages before the next Dyer rain is received necessitating the need for considering water
- 12 -
Save the Children | Emergency WASH and Nutrition response to conflict affected IDPs and host communities in
Dawa, Shebelle, Korahe Zones, of Somali and Bale Zone of Oromia Regions
Submission Date: 03 April 2019
trucking to the most affected areas. The zonal water office has requested save the children to
provide water rationing to 120,901 individuals living in 32 IDP sites.
Sub-sector: Sanitation
According to DTM round 13, over 241 IDP sites (62.11%) displacement sites reported having no
latrines and in IDP camp settings, urgent sanitation support is required to prevent the spread of
diseases due to the absence of sanitation facilities. The zonal health office data base shows that
the latrine coverage is 25%, 17%, 15% in Kebridehar, Debewoyen and Shilabo woredas
respectively.
Sub-sector: Hygiene Promotion
The latrine coverage of the three woredas are very small ranging from 15 to 25 % and the majority
of the communities do not have reliable source of water for drinking, cooking and personal
hygiene. There is high risk for AWD and other veco-oral diseases and requires improving Water,
Sanitation and Hygiene (WASH) practices of the community and increasing awareness of the
community.
Sub-sector: WASH NFI
There are 35 IDP shelters in Korahe zone accommodating 3,639 households and the IDPs are in
all 10 woredas of Korahe zone. The majority are drought induced IDP pastoralist families (85%)
affected by the 2016/17 drought while the remaining 662 households constituting 17% are flood
displaced owing to the recent flooding caused by the torrential rains and the overflow of the joint
Jerrer/Fafen Rivers. There are also some 880 households in six woredas of Korahe zone who
were affected by the recent flooding. Kebridehar, Debewoyen and Shilabo are some of the worst-
affected woredas with serious concerns for disease outbreak from contaminated water and
overflowing latrines. The NDRMC has distributed incomplete emergency shelter and NFI for 750
households in five flood affected areas. However, the response is inadequate and the rest of the
household requires WASH NFI support.
Sector: Nutrition
Sub-Sector: Infant and Young Child Feeding and Behavior Change
As described in the Deher assessment, the effect of continued conflict especially in Dawa woreda
and the continued severe water shortage in the Wordas of Korahe and Shebelle, have severely
affected livestock production in which families are not able to feed their infants and young children.
The pre-existing chronic food insecurity situation in the target woredas and the recurrent drought
- 13 -
Save the Children | Emergency WASH and Nutrition response to conflict affected IDPs and host communities in
Dawa, Shebelle, Korahe Zones, of Somali and Bale Zone of Oromia Regions
Submission Date: 03 April 2019
over the past few years has exacerbated the community’s vulnerability to poor infant and young
child feeding practices, which then results to increases cases of malnutrition. Based on the last
E-DHS 2016, in Somali region among children age from 6-59 months, only 3.1% of children
receive minimum acceptable meals and the prevalence of anemia among under five children is
88%. Moreover, the communities inhabiting these woredas are known to believe in risky myths
and misconceptions associated with breastfeeding and complementary feeding. This has resulted
into inappropriate infant and young child feeding and care practices, which compromises the
health and nutrition wellbeing of these children and their caregivers.
Sub-sector: Management of Acute Malnutrition
For more than a year, WFP was not able to deliver needed food distributions to Dawa Zone due
to an unstable security situation and ongoing access challenges in the area. There was an
interruption of TSFP food supplies for treatment of MAM in Dawa zone for more than six months,
which contributed to a further deterioration of nutrition status among the most vulnerable children
and women, specifically in the proposed four woredas. As such, the trend of acute malnutrition is
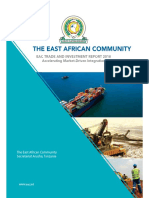
sharply rising as compared to this time of year in 2017. From March to October 2018, SAM cases
increased by 41%, compared to 2017 (Mar-Oct, 2017).6 Inpatient (SC) and outpatient (OTP)
admission for SAM management also increased by 41% and 60% respectively compared to 2017
in the same months.
SAM Trend in four Woredas of Dawa Zone in 2017 and
2018 Mar-Oct
1000 80.0% Year-2017
800
Case Count
60.0%
600 Year-2018
40.0%
400
20.0% % AVA
200
Increament
0 0.0%
Mar Apr May Jun Jul Aug Sep Oct
Months
6 SC’s assessment report finding conducted in October 2018
- 14 -
Save the Children | Emergency WASH and Nutrition response to conflict affected IDPs and host communities in
Dawa, Shebelle, Korahe Zones, of Somali and Bale Zone of Oromia Regions
Submission Date: 03 April 2019
From the routine screening report, it is observed that, nearly 10% increment was observed in
SAM admission in target woredas of Korhae and Shebella as compared to previous year. This is
due to the massive loss of animals during the last drought, animal population have significantly
reduced leaving households with only few heads that is not able to produce the milk required by
the family. With the current Deyr rains appearing to have totally failed, it is expected that cases of
malnutrition will rise in the coming couple of months due to the dry spell ahead until the coming
Gu rains, expected in April 2019, and the decrease in the amount of milk production of livestock
which is the
key SAM Trend in Six Target Woredas of Korahe and source
of food for
Shebelle Wordas, Jan-Nov, 2018
1500
1000
500
0
Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov
pastoralist children.
- 15 -
Save the Children | Emergency WASH and Nutrition response to conflict affected IDPs and host communities in
Dawa, Shebelle, Korahe Zones, of Somali and Bale Zone of Oromia Regions
Submission Date: 03 April 2019
Based on the report from regional health bureau, the August political instability that occurred in
Somali region have had huge impact on the existing health system in terms of staffing. There has
been high turnover of non-Somali staffs who had been working in Shabele and Korahey zones
particularly the six target woredas (Kalafo, Mustahil, Ferfer, Kabridahar, Shilabo and Doboweyn).
A total of 47 health professionals including doctors, nurses and health officers have left these
woredas following the incident. This have further weakened the capacity of government to provide
health and nutrition services in the target woredas.
Based on the routine screening report in the last eight months of 2018, the nutritional status in
the six target woredas of Korahe and Shebele Zones continues to be alarming the proxy GAM
ranging from 21-29%. Recent OTP and SC admission data shows the trend of acute malnutrition
is expected to increase by 11% and will remain a major concern exacerbated by ongoing measles
outbreaks in nearly all of the target woredas. Looking in to the ten proposed woredas in Somali
region, based on service and staff mapping assessment conducted by RHB, in the target nine
woredas of Somali region, 13 SAM management delivering facilities (12-OTPs and 1-SC)
becomes nonfunctional due to the recent and ongoing conflict. The assessment also showed in
the target woredas, there 106 health professionals and 46 health extension workers gap to
provide quality acute malnutrition management service, most of the gaps being at woredas of
Dawa Zone. The continued drought in woredas of Korahe and Shebelle also reduce the
production from livestock endangering the overall livelihood of the community, the overall trend
of SAM admission is summarized in the below to the right.
Justification for Intervention
Sector: WASH
Through its WASH intervention, Save the Children aims to increase access to clean and safe
drinking water, and to improve hygiene knowledge and promote the adoption of safe hygiene
practices among conflict-affected children and their families, contributing to a reduced risk of
outbreak of water related diseases. The WASH response will be implemented in three woredas
of Korahe zone, Somali region, and five woredas of Bale zone, Oromia region. The WASH
response in Bale will focus on institutional WASH support whereas the response in Korahe will
support flood and drought affected IDPs at community and household level.
Sub-sector: Water Supply
Availability of and access to safe water is closely tied to nutritional outcomes for children. The
severe drought has reduced access to water and increased the time and distance taken to collect
water. Breastmilk of lactating mothers has been reduced due to dehydration. Most health centers,
health posts and schools in the target areas are critically affected by the lack of water. The deyr
assessment teams identified a total of 6,934 water sources in the region. These sources include
- 16 -
Save the Children | Emergency WASH and Nutrition response to conflict affected IDPs and host communities in
Dawa, Shebelle, Korahe Zones, of Somali and Bale Zone of Oromia Regions
Submission Date: 03 April 2019
447 boreholes, 3,052 hand-dug wells, 3,168 birkas, 216 dams, 49 river intakes and 2 springs. In
addition to these, there are several multi-village water supply schemes that are being supported
by the Regional government. Overall, 32% of all existing water sources were not working by the
time of assessment and they need urgent rehabilitation to alleviate suffering and reduce risk of
over-stretching those functioning as well as the burden for water trucking needs, particularly in
Fafan, Jarar and Korahey zones. According to Korahe zonal water office, there is a need for
immediate water trucking support from December 2018 to April 2019 in 16 IDP sites of Kebridehar
woreda, nine IDP sites of Shilabo woreda, seven IDP sites of Debewoyen woreda to a total of
120,901 individuals (47,840 in Kebridehar, 41,961 In Shilabo, 31,100 in Debewoyen). According
to the IRC assessment 60,956 people in Sewina, Raytu, Legehida and Dawe Serar woredas of
Bale zone require urgent WASH assistance including water trucking. The Meher assessment also
highlighted that among human epidemic prone diseases in Bale Zones where the team has
engaged during the assessment, acute watery diarrhea (AWD), scabies, measles, moderate and
severe acute malnutrition are the most common public health emergency threats to the people in
the zones since the WASH coverage of those affected woredas in Zones are mostly vulnerable
for sanitation and hygiene concerns. AWD and scabies are an active public health in emergency
in the zones and remains the most likely anticipated risk because of low latrine coverage and
utilization and low access to safe and adequate water supply and shortage of household water
treatment chemicals in most woredas of the Zone.
The WASH Cluster and Regional Water Bureaus have determined a minimum of one month and
a maximum of three months as the appropriate period for water trucking activities. As part of its
exit strategy, Save the Children will construct roof water harvesting structure at institutional level
and rehabilitating nonfunctional water schemes to reduce the need for water trucking to lifesaving
facilities during drought shocks. Site identification will be carried out by the District Water Office
in collaboration with Save the Children.
Save the Children proposes the following activities:
Water trucking to health facilities and IDP sites as requested by Korahe and Bale zonal
water office. In line with zonal office priorities and requests, Save the Children will
implement water trucking in 25 health facilities where nutrition programs are operational
for a period of two months (60 days) from March 15 to May 15 2019 and 45 days for IDP’s
sites with high SAM caseload in Korahe zone from March 15 to April 30, 2019.
Rehabilitation of non-functional water schemes.
Construct roof water harvesting structure at health facilities
Procurement and distribution of water purification chemicals to ensure access to safe
drinking water for vulnerable communities.
- 17 -
Save the Children | Emergency WASH and Nutrition response to conflict affected IDPs and host communities in
Dawa, Shebelle, Korahe Zones, of Somali and Bale Zone of Oromia Regions
Submission Date: 03 April 2019
Daily testing of water quality to ensure free residual chlorine level in excess of 0.2-0.3 mg/l
as per government standards.
Regular monitoring at water storage tanks for health facilities and at household level.
Sub-sector: Sanitation
According to Somali region DTM round 13, 62.11% displacement sites reported having no
latrines, In IDP camp settings, urgent sanitation and hygiene support is required to prevent the
spread of diseases due to the absence of sanitation facilities. In response to the identified and
evolving needs, SC will construct sanitation facilities to the most vulnerable IDP living in target
operation areas.
Save the Children proposes the following activities:
Construction of Gender separated latrine
Install handwashing facilities for IDP’s.
Sub-sector: Hygiene Promotion
Many people in rural areas are not aware of the health hazards of inadequate sanitation and
hygiene practices and are unmoved to change their behavior. Therefore, it is essential to link
hygiene education with water supply and sanitation interventions to increase impact. Hygiene
promotion activities will be carried out to improve the health status of the targeted communities
and optimize the use of water and sanitation facilities provided, through addressing key hygiene
practices such as handwashing at critical times, proper handling of water, proper use of latrines,
safe disposal of solid waste, and other personal hygiene practices, in line with National
Emergency Task Force response plan and the activities will be developed in close collaboration
with the woreda water and health offices to ensure integration with nutrition activities.
Save the Children proposes the following activities:
Training on basic hygiene promotion tools for community hygiene volunteers to support
community-based hygiene promotion.
Hygiene promotion campaign and IEC material distribution. IEC material will be adapted
for children and all activities will have a child-focused approach. The WASH and Health
sectors have jointly developed materials clearly linking poor hygiene practices with
disease and malnutrition to expand and enhance traditional WASH messaging. Messages
will be disseminated during supplementary food distribution and OTP by the TSFP nurses
and by health workers as part of the health education component of the nutrition
interventions.
- 18 -
Save the Children | Emergency WASH and Nutrition response to conflict affected IDPs and host communities in
Dawa, Shebelle, Korahe Zones, of Somali and Bale Zone of Oromia Regions
Submission Date: 03 April 2019
Hygiene and sanitation campaigns will be organized to sensitize the affected communities
on AWD prevention and case management. Save the Children will also provide hygiene
kits to households and IDPs affected by AWD.
Provide WASH cleaning supplies and disinfectant to 25 health facilities.
Sub-sector: WASH Non-food Items
To support and enable water, sanitation, and hygiene related behaviors, Save the Children will
distribute WASH Non-food Items (NFIs) to SAM patients and their families at health facilities and
to households affected by flooding. In woredas directly impacted by flooding (Kebridehar, Shilabo,
Debewoyen), the National Flood Task Force has urged humanitarian response and early recovery
activities including distribution of WASH NFIs and health and hygiene education to prevent the
spread of water-borne diseases. The distribution of WASH NFI will complement other hygiene
promotion activities, such as hygiene sessions and household visits to disseminate hygiene-
related information and promote good hygiene practices. Prior to distribution, beneficiaries will be
sensitized on the contents of the kits and how to use them in order to improve hygiene practices
and reduce health risks.
Save the Children proposes the following activity:
Provision of WASH NFIs (jerry cans and buckets for safe collection and storage of
drinking water and soap to promote hand washing at critical times, dignity kit)
Sector: Nutrition
Save the Children will implement Nutrition programming in all of the fifteen woredas. The nutrition
program in the six woredas from Shebelle and Korahe zone will run for six months, while the
nutrition program in Dawa and Bale zones will run for ten months.7
Save the Children is proposing to implement a comprehensive nutrition response based on the
following observations and critical gaps:
In the absence of Mobile Health and Nutrition Teams (MHNTs), the respective WrHOs are
unable to organize regular outreach visits to IDPs, remote kebeles and/or areas with no
7Given the need to prioritize assistance, the CMAM program in Korahe and Shebelle will be implemented for six
months with lighter touch assistance as this project will be a continuation of the existing nutrition program. The
project in Bale and Dawa will be implemented for 10 months as the targets are critically affected by recent conflict
and the needs in the two locations require longer term support.
- 19 -
Save the Children | Emergency WASH and Nutrition response to conflict affected IDPs and host communities in
Dawa, Shebelle, Korahe Zones, of Somali and Bale Zone of Oromia Regions
Submission Date: 03 April 2019
health posts – leaving hard-to-reach communities with limited or no access to CMAM
services.
Limited local capacity of health workers, especially those newly recruited.
Limited capacity of the health system in addressing problems of acute malnutrition,
which is exacerbated by adverse effects of the current displacement.
The communities are also at an elevated risk of poor health because of potential disease outbreaks
and other childhood illness resulting from lowered immunity caused by poor nutrition status
WrHOs have limited capacity for supportive supervision and quality assurance, mainly due
to lack of vehicles, budget for fuel and per diem.
Transporting supplies from RHB to service delivery sites remains a challenge for WrHOs
due to poor logistics capacity.
Limited capacity of WrHOs to ensure timely and proper distribution of supplies and stock
management required for OTP/SC, especially for HCs and HPs.
Knowledge, attitude, and practice gaps of the community on proper use of CMAM products
and services, hygiene and sanitation, optimal IYCF practices and care of sick children.
Regular complete and accurate nutrition reporting has been a challenge in the target
woredas and a mechanism for verification of routine nutrition reports has not been
addressed by the WrHOs.
It is anticipated that the existing poor health and nutrition status of these communities is likely to
escalate in the next few months due to food insecurity, inadequate water supply and the low health
and nutrition service coverage. These are clear pointers that the region is still affected by acute
under-nutrition and hence continued support to the existing health system is urgently needed in
these Woredas. With the support of OFDA resources, Save the Children seeks to continue
emergency nutrition response in the target woredas using the IYCF-E/CMAM intervention
modalities along with capacity building efforts to sustain gains.
Sub-Sector: Infant and Young Child Feeding and Behavior Change
Support and promotion of IYCF is the mandate of the Ministry of Health, which is mostly facility-
based. However, the current staffing capacity does not have the time or resources to dedicate to
quality IYCF-E promotion. In this project, SC will support protection and promotion of optimal
IYCF-E practices for children 0 – 23 months and pregnant/lactating women, with a focus on
exclusive breastfeeding, appropriate complementary feeding and promotion of micronutrient
supplementation. This will be reinforced through behavior change communication and
- 20 -
Save the Children | Emergency WASH and Nutrition response to conflict affected IDPs and host communities in
Dawa, Shebelle, Korahe Zones, of Somali and Bale Zone of Oromia Regions
Submission Date: 03 April 2019
messaging. SC will conduct trainings for Health Workers (HWs)/HEWs on IYCF-E. In addition,
mother-to-mother support groups (MtMSGs) at OTP sites and in communities will be established
to encourage mothers to share experiences and provide support to overcome challenges. In
addition, behavioral change messages on IYCF-E will be communicated to community leaders.
At the beginning and end of the project, baseline and endline surveys will be carried out to
determine baseline data on current practices and to inform specific IYCF messaging and
activities.
Save the Children has been implementing IYCF-E include community level interventions such as
MtMSGs through previous emergency nutrition projects. To be resource efficient, ensure quality of
the intervention and considering the ongoing government effort on IYCF-E, SC proposes 45 MtMSGs
in the target woredas, prioritizing Kebeles/IDP sites based on the level of need and area which are
not addressed in previous projects. Like other activities selection of IDP sites/Kebeles, MtMSG
intervention will be coordinated with local authorities and as criteria, Kebeles/ IDP sites with poor
access to health facilities, continued higher levels of acute malnutrition rate (relative higher rate of
proxy GAM and SAM admission) that were not addressed in previous emergency projects will be
targeted. SC understands the importance of linkages between IYCF-E corners at health facilities and
MtMSGs. The MtMSGs session will be facilitated by the respective Kebele Health Extension Worker
and on the initial phase of the project HEWs will trained on IYCF-E (which is proposed in this
document) to help them facilitate the MtMSGs, identify and refer mothers with continued breast
feeding difficulties to health facilities with IYCF-E corners or nearby health facility for further
intervention. SC’s IYCF nurse within the catchment health center staffs will also provide continues
supportive supervision to monitor and support the routine activities of MtMSGs.
Sub-Sector: Management of Acute Malnutrition
Even though management of acute malnutrition in Ethiopia is implemented through the
government system, these target woredas are known to have limited number of health workers
due to high turnover, inadequate Community Management of Acute Malnutrition (CMAM)
equipment and protocols, and frequent gaps in CMAM supplies, especially TSFP commodities.
Through this funding, Save the Children will continue to implement CMAM activities in the targeted
locations, including supportive supervision, provision of supplies and materials, and capacity
building. Activities planned but not limited include supporting existing health facilities in availing
technical staff, logistics, and technical support to improve quality management of SAM and MAM
treatment. TSFP will be implemented in priority one woredas in collaboration with WFP and
RDPPB. Save the Children will also strengthen and establish new TSFP sites at health facilities
for proper linkage, and at the community level, provide CMAM training for HEWs/HWs, Food
Distribution Agents (FDA) and CHV to enhance proper coverage of MAM treatment. Furthermore,
SC will provide logistics support for transportation of supplies from regional warehouses to health
- 21 -
Save the Children | Emergency WASH and Nutrition response to conflict affected IDPs and host communities in
Dawa, Shebelle, Korahe Zones, of Somali and Bale Zone of Oromia Regions
Submission Date: 03 April 2019
facilities and strengthen the supply chain by training Zonal health department staff, and Woreda
Health Bureau (WHB) staff to improve efficiency in the supply handling.
Save the Children’s Capacity to Implement
With a presence in almost all of Ethiopia’s regions, Save the Children works towards giving
children a healthy start in life, the opportunity to learn and protection from harm. Our promise is
“we do whatever it takes to save children,” and we ensure we keep it through our strong
engagement in both humanitarian and development fronts. In 2017, our programs in health,
nutrition, education, WASH, child wellbeing, child friendly systems and structures, and
livelihoods/resilience benefited more than 9.8 million Ethiopians including 5.5 million children.
Moreover, SC also has a number of qualified and well-experienced technical advisors and
managers in all relevant sectors at the Country Office, Regional, and HQ levels. Through the
utilization of the well-developed tools and guidance from the well-trained and skillful personnel,
SC is able to ensure the high quality of implementing projects that are up to or above Save the
Children International’s minimum standards. In program operations, SC also has highly qualified
and well-trained staff who have had years of experience in program operations, administration,
and supervising multiple departments and teams to manage and implement large-scale and highly
complex programs. Through years of delivering impactful work in Ethiopia, SC continues to be
the leading humanitarian and development actor who promptly and effectively respond to
humanitarian crises in Ethiopia. Save the Children is currently implementing ECHO, IRC/OFDA,
UNOCHA funded WASH, Nutrition and protection programming in Somali and Oromia regions.
We also have OFDA funded life-saving multi-sectoral responses in seventeen woredas in Afar
and Somali regions. These current operations have placed SC strategically to implement the
proposed project in Somali and Oromia regions only with existent geographic presence but also
with extensive knowledge of OFDA regulations and requirements, reflection on areas of
improvement and key learnings from past implementation of OFDA and other donors funded
projects.
In terms of coordination, SC is a strong advocate of a broad programmatic approach employing
effective coordination with all relevant stakeholders in Ethiopia. To avoid duplication of effort, to
target the most vulnerable populations and to maximize existing resources, SC is actively and
closely coordinating with UN Agencies, International NGOs, local NGOs, and local Government
through the established Clusters. Save the Children is member of Child Protection, WASH and
Nutrition Sub-cluster. Through these forums, SC has been stressing priority needs for children in
the emergency context while supporting joint inter-agency rapid assessments, sharing information
about our own rapid assessment findings, coordinating with the other actors on activities they are
planning to undertake, advocating for the prioritization of children in the response, and also
ensuring that humanitarian standards are met across the response. Additionally, SC actively
engages with the Humanitarian Country Team (HCT) to provide inputs and updates towards the
strategic priorities outlined for the country-wide IDPs response.
- 22 -
Save the Children | Emergency WASH and Nutrition response to conflict affected IDPs and host communities in
Dawa, Shebelle, Korahe Zones, of Somali and Bale Zone of Oromia Regions
Submission Date: 03 April 2019
Realizing the synergies drawn from coordination across actors, SC continues not only to support
all relevant coordination efforts at all levels but also to advocate for an even stronger, closer and
more transparent coordination across and between actors in Ethiopia. Through this close
coordination with all key stakeholders, SC works towards eliminating any duplications in the
programs implementations from different stakeholders in order to ensure that all the resources
are utilized to maximize the humanitarian assistances, that will provide holistic support addressing
all basic needs, to as many vulnerable people as possible. Furthermore, where possible, as SC
recognizes the importance of coordination with local authorities and Government bodies, SC also
engages in communication with relevant government bodies and their line bureaus overseeing
those areas. By building upon these relationships, SC continues to seek areas for collaboration
with duty bearers both to ensure community acceptance and sustainability of the action.
Save the Children acknowledges that the situation in the targeted location is quite unstable and
there might be new or worsened humanitarian condition during the implementation period. For
this reason, SC is well prepared to scale up immediately by mobilizing internal and other sources
of external funding to cover the unmet needs of the affected population. Save the Children has
the capacity and the geographical presence throughout the country to quickly mobilize and
respond to new and emerging crisis in short period of time. If in future, during the implementation
period, the needs of the affected population significantly change and is outside the scope of this
project, SC will quickly mobilize funds from its internal pooled fund to cover the urgent and
lifesaving needs in and around the targeted locations to minimize loss of life and alleviate
sufferings. Save the Children is also regular recipient of rapid response mechanisms such as
RRM (where OFDA is a contributing donor), ERM (ECHO is the contributor) and START Fund to
quickly and efficiently respond to new and emerging humanitarian needs. Save the Children has
a positive track record in responding to new crisis and mobilizing funds in short periods of time
(such as in Gedio/Guji and Wolega response). If the situation requires, in consultation with OFDA,
SC will look into other ways where part of this funding can be re-allocated to address to meet new
needs in or adjacent to program areas.
Alignment of Proposed Intervention with OFDA’s Mandate
As the proposed intervention aims to save lives and provide basic assistance and services to the
conflict-affected children and their families, it is in line with OFDA’s mandate to save lives, alleviate
human suffering, and reduce the social and economic impact of disasters. This proposed
intervention aims to mitigate and alleviate IDPs and host communities’ suffering from the
displacement while reducing the relevant risks that both IDPs and host communities are exposed
to. These will subsequently lead to the long term lives saving. In addition, this proposed project
will contribute to the overall SC program in Oromia and Somali regions with the funding from
agencies, including UNOCHA, Save the Children Korea, OFDA and International Rescue
Committee.
- 23 -
Save the Children | Emergency WASH and Nutrition response to conflict affected IDPs and host communities in
Dawa, Shebelle, Korahe Zones, of Somali and Bale Zone of Oromia Regions
Submission Date: 03 April 2019
B. Program Description
1. Program Overview
a) Goal: To save lives and prevent suffering of conflict affected internally displaced people and
host communities, children and their families in Oromia and Somali Regions.
b) Beneficiary Numbers:
o Total Number of Beneficiaries Targeted (Individuals):
Somali Region: 45,632
Oromia Region: 10,919
Total Number of IDPs Targeted (Individuals): 30,000 (14,700 F; 15,300 M)
c) Critical Assumptions:
The followings are the assumptions critical to the success of the proposed program
Security situation does not deteriorate to a point that makes it impossible for Save the
Children to continue operations
Optimal coordination with and participation of the local government sector offices in
implementation of the program;
Program sites (water distribution centers, Child friendly spaces, food distribution sites,
SCs, OTP sites) will remain physically accessible during implementation;
Save the Children will obtain sufficient supply of essential supplementary and
therapeutic foodstuffs, in particular super cereals (CSB+++) or Ready to Use
Supplementary Food (RUSF) from WFP. Save the Children has submitted a field
level agreement (FLA) proposal to WFP to support the implementation of TSFP
from April-December, 2019 in both regions. The proposal is under revision and
SC expects the FLA to be approved by Mid-April 2019. Save the Children also
expects to receive therapeutic milk and Ready to Use Therapeutic Food (RUTF) from
UNICEF through RHB, and Emergency Health Kits from WHO for Mobile Health and
Nutrition Teams for priority one woredas.
Adequate number of staff and committed community volunteers are available to
ensure effective program implementation and outreach activities respectively;
- 24 -
Save the Children | Emergency WASH and Nutrition response to conflict affected IDPs and host communities in
Dawa, Shebelle, Korahe Zones, of Somali and Bale Zone of Oromia Regions
Submission Date: 03 April 2019
Memorandum of Understanding is promptly signed among stakeholders to initiate
implementation;
Water trucking contractors will be available and contract agreement signing process
finalized for timely delivery of water;
No uncertain political environment/civil unrest that prevents program from operation
d) Mitigation strategy
Regular monitoring of the security situation and five-level security plan will be in
place to reduce security-related risk.
Close follow up, early warning and emergency preparedness plans will be
developed ahead of the drought and timely communicated with concerned bodies.
Save the Children will further coordinate with local government and other
humanitarian organizations and agencies to utilize their existing facilities in areas
where Save the Children has limited operational presence.
Save the Children will set up a robust multi-layered monitoring system involving
local authorities and communities to manage this risk
d) Program Strategy:
Sectors:
Sector 1: WASH
The followings are the planned intervention under WASH program:
Somali Region/Korahe Oromia Region/Bale Zone
Zone
Sub-
sect Intervention Shila Dobow Kebrida Sewe Dawaketc Rayi Legahi Guradom
or bo ein har na hen tu da ole
Water
Sup
Wat
Y Y Y Y Y Y Y Y
ply
er
Trucking
- 25 -
Save the Children | Emergency WASH and Nutrition response to conflict affected IDPs and host communities in
Dawa, Shebelle, Korahe Zones, of Somali and Bale Zone of Oromia Regions
Submission Date: 03 April 2019
Rehabilitation
of non-
functional Y Y Y
water
schemes
Distribute
chlorine to
woreda water
office to Y Y Y Y Y Y Y Y
conduct
chlorination
test
Water
Purification
Y Y Y Y Y Y Y Y
Chemical
Provision
Water
Management Y Y Y
Committees
Hygiene
Promotion Y Y Y Y Y Y Y Y
Campaign
Construct
gender
separated
Y Y Y
semi-
Sanitation
permanent
latrines
Install hand
washing Y Y Y
facilities
Decommissio
ning of Y Y Y
latrines
Hygiene Kit
Hygiene Promotion
Y Y Y Y Y Y Y Y
Distribution
Provide
WASH
cleaning Y Y Y Y Y
supplies and
disinfectants
- 26 -
Save the Children | Emergency WASH and Nutrition response to conflict affected IDPs and host communities in
Dawa, Shebelle, Korahe Zones, of Somali and Bale Zone of Oromia Regions
Submission Date: 03 April 2019
a) Sector Objective: To increase access to safe drinking water, sanitation and to improve
hygiene practices at health facilities, nutrition centers and IDP sites.
b) Dollar amount: $863,662 USD
Total Number of people targeted: 52,500 Individuals
Total Number of IDPs targeted: 30,000 Individuals (14,700 F; 15,300 M)
c) Geographic Areas
Country Admin. Level 1: Admin. Level 2: Admin. Level 3: Woreda
Region Zone
Ethiopia Oromia Bale Sewena,Dawaketchen,Rayitu,
Legahida and Guradamole
Somali Korahe Shilabo
Debewoyen
Kebridehar
d) Sector-level Coordination
Save the Children’s WASH team will continue to coordinate closely with the National Emergency
Task Force on drought response along with the WASH cluster, led by the Ministry of Water
Resources in collaboration with UNICEF. Coordination will be optimized through linkages to the
WASH Task Force, at both zonal and regional levels. Task Force meetings take place on a bi-
weekly/monthly basis, however during an emergency they can be called as needed. Save the
Children’s WASH team will work closely with the zonal/woreda WASH member offices (water,
health, and education) and other NGO and UN partners to ensure quality targeting and prevent
duplication of activities.
Keywords: Pastoralists, WASH in health facilities
Keyword Integration: Please see the Nutrition Sector for details on ‘pastoralists’. The WASH
and Nutrition components of this project are designed to complement one another to enhance
and sustain nutrition gains and prevent the outbreak and spread of disease. Under the Water
Supply sub-sector, integration will be achieved through water trucking to health facilities, Hygiene
- 27 -
Save the Children | Emergency WASH and Nutrition response to conflict affected IDPs and host communities in
Dawa, Shebelle, Korahe Zones, of Somali and Bale Zone of Oromia Regions
Submission Date: 03 April 2019
Promotion sub-sector activities will be conducted at health facilities targeting SAM and MAM
patients, and WASH Non-food Items will be provided to Nutrition Sector beneficiaries.
e) Technical Design
Save the Children is using an integrated approach to address the underlying causes of
malnutrition. The project will provide a holistic response to ensure affected families and their
children have access to necessary WASH services to maintain good health and prevent water
related disease outbreaks in the target location. WASH sub-sector approaches are designed to
be implemented at household and institution levels. The household level approach will target
families affected by malnutrition, including households with members treated for malnutrition,
through either OTP or TSPF, or otherwise identified by emergency nutrition programming. The
health facilities level approach will supply water through water trucking via vouchers as required
and connect the roof and the storage via pipe. The community will have access to safe water
supply through the rehabilitation of water points, boreholes and pipelines and water trucking. For
sanitation, SC proposes construction of semi-permanent gender separated latrines to IDP sites;
both approaches include hygiene promotion activities that will focus on community involvement
in hygiene sessions, household visits and community awareness campaigns and provision of
hygiene kits. Additionally, the project will build community resilience and increase sustainability
of WASH services by enhancing the capacity of village level water and sanitation management
committees to manage operate and maintain water and sanitation facilities. The project uses a
community-based approach – forming WASH committees and community mobilization teams and
providing trainings – to ensure community ownership and sustainability of interventions. Save the
Children will implement the WASH project in eight woredas (five woredas in Bale zone, and
three woredas in Korahe zone). Of the total seven non-OFDA WASH woredas, Save the
Children currently has a WASH project in four woredas of Dawa zone funded by IRC (OFDA
is the original donor). This project will come to an end on 27 April 2019. The proposed
OFDA project was designed with the assumption that the current WASH project will
complement the proposed nutrition program for some months. In addition, Save the
Children secured a new grant from UNOCHA to implement WASH projects in Dawa zone.
The project was approved on 18th of March and will run for 12 months. For the three
remaining non-OFDA WASH woredas in Shebelle zone, the woredas are prioritized for
funding for the upcoming UNOCHA call. Save the Children will submit proposal to
UNOCHA as soon as the call is released. In the meantime, Save the Children is looking at
other options to support the woredas, including provision of NFI support.
Sub-sector 1: Water Supply
Technical description: To increase access to safe water and availability of water throughout the
day to the most affected groups, including those affected by displacements and/or drought, SC
will rehabilitate existing water supply schemes, establish and/or strengthen capacities of Water
Management Committees (WMCs), enhance access to and use of household water treatment
chemicals for families who fetch water in unimproved water sources, and conduct emergency
water trucking service (WT) to health care facilities (average 60 days of service) and IDP
- 28 -
Save the Children | Emergency WASH and Nutrition response to conflict affected IDPs and host communities in
Dawa, Shebelle, Korahe Zones, of Somali and Bale Zone of Oromia Regions
Submission Date: 03 April 2019
communities (average 45 days of service). For IDP’s sites with high SAM caseload in Korahe
water will be trucked for 45 days as durable solutions are sought. The proposed WASH
rehabilitation activities in Korahe zone are minor and it is expected that construction will
be completed in 45 days. Beneficiaries therefore will be able to be supplied with water right
after the completion of the rehabilitation activities. Where as in Bale zone, the roof water
harvesting planned to be installed in 25 health facilities will take 60 days to complete
(transportation, installation and connecting with the roof) as target locations are scattered.
Save the Children will therefore truck water to the health facilities for 60 days until durable
solutions are in place.
Water trucking is only required for sites where vulnerable populations are unable to access any
type of water points, or lack support from the government or other agencies (in line with the WASH
Cluster response strategy), with populations provided with an allocation of water necessary for
survival. The Zonal Water Office, the MoH and Save the Children will intensively work with each
facility and community on water rationing modalities and an exit plan by exploring water supply
alternatives. Save the Children will also install basic equipment for rainwater harvesting and safe
storage in HCF, and provide them with technical information on possibilities for upgrading the
water system in order to be less dependent in WT services in future. The WT has been explicitly
requested by the Oromia and Somali Regional Governments, prioritized by the WASH Cluster,
while the duration of water trucking services was decided by the Zonal Water Offices.
Rehabilitation of water schemes: Save the Children will rehabilitate an estimated six water
supply schemes (hand dug well or shallow well) within or adjacent to IDP sites and health facilities;
thereby providing support for long-term safe water access for communities, health facilities and
CMAM services in Shilabo, Debewoyn and Kebridehar woredas.
The Zonal Water Office requested support to rehabilitate hand dug wells and pumping systems,
replace hand pumps that cannot be repaired, and repair of superstructures to reduce risk of
contamination (apron, drainage). Where unprotected hand dug wells are the water source, SC
will protect the wells. In the event that a hand-dug well platform needs to be rehabilitated, SC will
include a manhole in the cover slab to facilitate alternative access in the event that the pump fails.
In circumstances where deep boreholes are the only groundwater sources available, SC will
repair existing structures (pumps, electric panel boards, reservoirs, water pipeline, and distribution
tap stands). Finally, a shock chlorination (disinfection) will be conducted before the handover to
the community. A detailed technical assessment will be conducted in partnership with the Water
Office elaborating a detailed rehabilitation intervention plan and BOQ for each scheme.
- 29 -
Save the Children | Emergency WASH and Nutrition response to conflict affected IDPs and host communities in
Dawa, Shebelle, Korahe Zones, of Somali and Bale Zone of Oromia Regions
Submission Date: 03 April 2019
Save the Children will ensure that the WASH committees are formed (or resumed) at the
beginning of the project and participate effectively along the project cycle (please refer to section:
WASH Committees). Save the Children engineers will be accompanied as much as possible by
Zonal Water Officers who will regularly monitor and supervise the activities to ensure the quality
of construction is in line with SC’s Construction Policy.
Water trucking services to most-at-risk HCF and IDP communities: Save the Children will
initially provide water through trucking to nine IDP sites (30,000 individuals) in Korahe zone of
Somali region for 45 days and 22,500 SAM children and their families in 25 health facilities of
Bale zone for 60 days (20 SC and five OTP).
Water trucking rationale
For IDP’s deprived of easy access to a nearby water source (protected or unprotected), the option
of household water purification is discarded and the only temporary solution is short-term
emergency water supply through water trucking until more reliable water systems is rehabilitated
or built. Water trucking to HCF is the final mechanism utilized for maintaining the minimum quality
of care and avoiding the facility to close temporarily. The health facilities are unequally equipped
to face water shortages, but all have their coping mechanism to ensure availability of water for
the functioning of the facility. These coping mechanisms include access to a nearby water well or
well in the premises, stored rainwater in the premises, use of donkey water-carts from unprotected
water sources, support from the local Water Bureau with water trucking service, etc, unfortunately,
some of the most water deprived facilities may exhaust their coping mechanism in extreme
situation and require humanitarian water supply at the pick of the water shortage. OFDA project
will support this critical water gap with water trucking, while analysing case-by-case a more
sustainable solution with the HCF and local authorities, and the population served by the HCF.
Water trucking description
Save the Children will use a voucher-based system for distribution as required, with vouchers
distributed to beneficiaries, health facilities and then exchanged with water trucking contractors
upon receipt of water. Implementation of water trucking interventions is typically outsourced to
two or more contractors to supply health facilities with agreed quantities over the specified period.
Water sources approved by the Regional Water Bureau Communal are used as water trucking
filling point. When needed, storage at point of deliver will be ensured through the installation of
10mᶟ polyethylene tanks with tap stands. The volume of 10mᶟ was decided based on past
experiences, since it is the typical capacity available and because the volume will not require
refilling on consecutive days. In exceptional cases we may install 2 tanks per community or very
- 30 -
Save the Children | Emergency WASH and Nutrition response to conflict affected IDPs and host communities in
Dawa, Shebelle, Korahe Zones, of Somali and Bale Zone of Oromia Regions
Submission Date: 03 April 2019
large HCF. In HCF we will connect the tank to gutters in order to make the facility less dependent
to water trucking. The rationale for this option is explained in a following section.
With regards to water quality, this project will provide barrels of chlorine powder to the woreda
water offices with instructions on chlorination of water truck tanks at the filling points. Pool testers
and reagents as well as training sessions for FRC testing will be provided to all government water
offices as well as health center staff. Water quality will be tested upon arrival of the trucks to the
facilities and camps by trained water operators of the Water Office or SC staff: they will make sure
the free residual chlorine level is above 0.4 mg/l at point of delivery as per government standards.
Regular monitoring will be carried out at health facility and household levels by water operators.
If the water at the household level is nil or below 0.2 mg/l, the chlorine concentration will be
adjusted in the storage tanks. Monthly reports on the quantity and quality of water delivered will
be provided to woreda water offices by the Save the Children WASH staff. Save the Children will
design water trucking interventions to meet the standard as set in the government water trucking
guidelines. This is just enough at household level for drinking, cooking and very limited hygiene
(however, some communities may have access to surface water for hygiene –this will need to be
confirmed).
Save the Children will ensure that water supplied to health facilities, IDP’s, flood or water
born disease, and drought affected populations through pipe water system and water
trucking are chlorinated to the WHO standard. And percentage of rehabilitated water
schemes with FRC greater 0.2mg/l will be measured and reported to take immediate action.
SC will carry out water quality tests in all target water source and storage facilities based
on specific physical and biological parameters (PH, turbidity, e-coli and total coliform). The
project will use the WHO water quality test protocol to ensure the distributed water is safe.
Testing will be undertaken at source, storage and tanks and homes and where quality is
not acceptable, relevant solutions will be applied such as source chlorination, bulk
chlorination or bucket chlorination. Shallow wells and boreholes will be treated through
chlorination and households will be supplied with aqua tabs to provide a second barrier
to ensure provision of safe water.The treated water sources will be monitored daily in order
to ensure that free residual chlorine (FRC), at point of use, is within recommended
standards (greater than 0.2 mg/l). If the water at the household level is not reaching the
standard of greater than 0.2 mg/l, SC will act accordingly and increase the level of chlorine
in the storage tanks respecting the national and WHO limits. All water quality testing and
treatment will be done in coordination with the woreda water office, WASH committees,
project WASH officers. SC will provide Pool tester and reagents as well as training
sessions for FRC monitoring to WASHCO’s, volunteers and testing will be conducted on a
weekly bases.
- 31 -
Save the Children | Emergency WASH and Nutrition response to conflict affected IDPs and host communities in
Dawa, Shebelle, Korahe Zones, of Somali and Bale Zone of Oromia Regions
Submission Date: 03 April 2019
Save the Children will meet minimum drinking water quality standards (in accordance with
WHO/national Drinking Water Quality Guidelines). Depending on technical feasibility, a
range of chlorination options at source will be carried out. These include (a) Water source
shock chlorination of wells (b) bulk chlorination, particularly at water storage points in
nutrition centers and IDP sites and in locations where a centralized water storage tank is
provided at distribution points. Residual chlorine levels will be monitored at the source. In
order to ensure that there is chlorine residual at household level, the project team will
distribute household water purification chemicals. If the water to be treated is turbid with
a Nephelometric Turbidity Unit (NTU) greater than 20, then PUR, a disinfectant with
combined flocculent water treatment chemical will be distributed. However, if the water to
be treated has turbidity factor less than 20 NTU, a simple disinfection such as Aqua Tab
will be used. Pool tester and reagents will be provided for volunteers to check chlorine
residual level at HH level.
Water trucking triggering mechanism and survival allocation: The sites selected and prioritized for
water-trucking follow these triggering criteria:
Communities: per capita consumption drops below 5 l/c/d or forced migration due to lack
of water is reported; the government does not have the capacity to respond (already
engaged in other communities; there is no alternative source of water than can be
rehabilitated in emergency; a high SAM and MAM caseloads are reported or there is an
abnormally high reported cases of diarrhea and scabies (a water-washed diseases). The
WT service will aim at distributing a survival allocation of 5 l/c/d, equitably through a
voucher mechanism.
HCF and Nutrition care facilities: according to MoH, an average of 150 patients on average
(10 in-patients and 140 out-patients) visit health facilities per day. The quantity of water
required for inpatient per day is 40 liters and 5 liters of water per out-patient per
day. Therefore the total water requirements per each HF per day is be 40x10+140x5=
1,100 liters per day. Another 900 liters are necessary for the staff, the cleaning and
disinfecting, and contingency in case of a sudden increase of number of patients. If the
existing water supply or coping mechanism (donkey carts, etc…) cannot reach 2 m3 per
facility per day, the WT service will be triggered. The actual triggering volumes vary and
will be calculated for each facility, in line with SPHERE 2018 recommendations.
Rationale for enhancing water security in the HCF through rainwater harvesting and safe storage
systems: The annual rain fall of Bale zone where the roof water harvesting intervention sites
located ranges from 900 to 1,400m (over the last decades the average rainfall is 1,272 mm) and
there are only 4 months will less than 60 mm/month –source: GoE and climate-data.org. In future
it is uncertain whether rainfall will increase or decrease, but precipitations are already erratic (they
- 32 -
Save the Children | Emergency WASH and Nutrition response to conflict affected IDPs and host communities in
Dawa, Shebelle, Korahe Zones, of Somali and Bale Zone of Oromia Regions
Submission Date: 03 April 2019
changed pattern) and the change will be exacerbated by the climate change (Climate change risk
profile for Ethiopia, USAID Factsheet 2016). With regards to harvested rainwater in the worst case
scenario -small roof area catchment and low yearly precipitation- the potential for RWH system is
good: 60 to 120 m3 of rainfall could be harvested annually. We will provide each HCF with 1/ an
orientation on how to better manage water demand, water conservation and water quality, and 2/
a RWHS technical sheet containing the following information: monthly harvested rainwater taking
into account all parameters (surface, coefficient efficiency, annual run off), the tank overflow with
the provided 10 m3 tank and the tank overflow with a maximum rainwater catchment area and an
optimum tank size that would ensure close to 100% efficiency. This means that the overflow will
be limited to the minimum and the reliability of supply to satisfy the demand close to the maximum.
We also can provide an investment cost estimate, an estimated water delivered by the RWHS
and a payback time. As a result the HCF and local MoH will be enabled to approach institutions
for upgrading the system (more gutters, a new ferrocement tank with the optimum size) and
thus improving sustainably the quality of care. This is the concept of climate resilient institutions
–schools and HCF- Save the Children is promoting in the ESA region.
The emergency 10m3 tank is considered as a transition towards a more advanced RWHS. With
regards to cost, the 10m3 storage tanks are already in the budget. The equipment of the roofs
with gutters adapted to the 10m3 tank is not significant compared to the water trucking cost.
Finally we will ensure water safety risks are mitigated through low-cost water treatment systems:
leaves and other debris are prevented to enter in the system with a coarse mesh filtering at the
mouth of inflow pipe. All the debris, dirt and other contaminants especially bird dropping etc.
accumulated on the roof during dry season will be disposed of by a simple first-rain flushing
diversion system.
The proposed roof water harvesting is an option, which can be, augment the water demand
of health institutions during the dry season. There are two rainy season in Bale zone
woredas and rainwater harvesting can be possible twice in a year. As the proposed
woredas are located in a similar rainfall distribution and amount the average monthly
rainfall of the proposed location is 150 mm/ month. According to the Ministry of health
WASH in health facility manual, the standard roofing area for Health posts is 73 M2,
therefore the volume of water harvested from corrugated iron roofing (c=0.8) is equal to
73*150*8=8760 litter/month, The volume of water tank is supposed to fulfill all the health
facility water demand. However, as per the government standard and cost effectiveness,
we are planning to install 10000-liter plastic fiber tank. The average monthly requirement
of water per health facility is 22500 litter /month
- 33 -
Save the Children | Emergency WASH and Nutrition response to conflict affected IDPs and host communities in
Dawa, Shebelle, Korahe Zones, of Somali and Bale Zone of Oromia Regions
Submission Date: 03 April 2019
Though the design criteria was set deliberately considering only the water usage for
drinking purposes, there is still a deficit of 12500 litter of water to satisfy the requirements
of the beneficiaries. However, it is important to bear in mind that the scheme is intended
to supplement the usual water shortage occurring during the dry seasons from ponds, and
hence, improve the health condition of the beneficiaries to a certain level. Moreover, it is
believed that the roof water harvesting will have a great impact and role on community
awareness towards the use of other alternative water sources such as rainwater other than
the traditional ponds and may encourage the beneficiaries to similar replication of the roof
water harvesting individually or on group basis. Therefore, rather than abandoning the
installation of water tank, it is recommended to connect the system with a very cheap cost
pipe work to collect the roof water.
At health facilities where we do water harvesting, Save the Children will respective
minimum drinking water quality standards (in accordance with WHO/national Drinking
Water Quality Guidelines) are to be delivered, wherever possible and technically feasible,
the chlorination of water will be centralized at the water tank level. Pool testers and
reagents as well as training sessions for FRC testing will be provided to all government
water offices as well as health center staff. Regular monitoring will be carried out at health
facility by health center staff. If the water at the health facility level is below 0.2 mg/l, the
chlorine concentration will be adjusted in the storage tanks.
Water purification chemical provision: The national WASH cluster encourages partners to
procure water treatment chemicals, the availability of UNICEF warehouse are not adequate and
there will not be any overlapping in the target areas proposed by SC and therefore, Save the
Children will distribute point-of-use (POU) water treatment products including PUR or Bishangary
and Aqua tab to control against contamination.8 Household water treatment chemicals will be
distributed based on need and according to the following criteria: the community is utilizing
untreated surface water sources; SAM and MAM case load to avoid the possibilities of relapse
after children discharged from health facilities, WASH-related disease outbreaks are affecting the
community; IDP sites without access to safe water. An estimated 587,160.00 sachets of PURE
or Bishangari, and 1,174,320 tablets of Aqua tab will be provided for 45 days, based on one tablet
of Aquatab or two sachets of PUR per household per day, for households not receiving water
trucking. Turbid water with a Nephelometric Turbidity Unit (NTU) greater than 20, will be treated
with PUR, a disinfectant with combined flocculent water treatment chemical. For water with a
turbidity factor less than 20 NTU, Aquatab or WaterGuard will be distributed. Correct use of the
chemicals and promoting locally produced water treatment products such as commercial bleach
or local filters will be demonstrated during hygiene promotion activities conducted by both WASH
Officers and Health Hygiene Promotors. Unimproved Water sources will be treated through
8Save the Children will adhere to the recommendations stipulated in the POU water treatment chemical guidelines
developed by the Emergency WASH Cluster.
- 34 -
Save the Children | Emergency WASH and Nutrition response to conflict affected IDPs and host communities in
Dawa, Shebelle, Korahe Zones, of Somali and Bale Zone of Oromia Regions
Submission Date: 03 April 2019
bulk or bucket chlorination as required. However, households will be supplied with water
treatment chemicals to provide a second barrier to ensure provision of safe water.
Establishment and Training of Water Management Committees (WMCs): In locations where
WASHCO’s already exist, Save the Children will work with the respective woreda water offices to
select water schemes serving the IDP communities for rehabilitation. SC will revitalize WASHCO’s
and conduct training in the area of scheme management, administration, operation and
maintenance, sanitation and hygiene issues. The programme will be adapted by our trainers to
the knowledge and skill level of each WASHCO (we may spend more time and effort with the
weakest WASHCO). Ultimately these committees will be made responsible for the operation,
maintenance and management of water supply infrastructure, specifically sanitation and hygiene
promotion, and also play an important role during planning and construction phases. WASHCOs
will be elected by the IDP and host communities democratically and the participation of women
and men will be encouraged. Save the children in collaboration with the district, water office will
be involved in facilitation of committee selection to ensure that there is no exclusion from the IDP
communities. The WASHCO members will mobilize IDP and host communities to participate in
design and implementation of the WASH infrastructure. Each WASHCO will have seven
members: out of seven members, at least three should be female. WASHCO members will be
trained for 3 days on basic hygiene promotion, cost recovery mechanisms, water scheme
management, maintenance, including how to troubleshoot and fix simple defect, change simple
spare parts, conduction of monthly inspections for preventive maintenance.
Indicator Type Target Remark
Male Female Total
Mandatory Indicators
Number of people directly utilizing 26,775 25,725 52,500 30,000 in IDP sites
improved water services provided with and 22,500 at
OFDA funding health facility
Percent of households receiving point- - - 100%
of-use chlorine products whose water
supplies have free residual chlorine
(FRC) present
- 35 -
Save the Children | Emergency WASH and Nutrition response to conflict affected IDPs and host communities in
Dawa, Shebelle, Korahe Zones, of Somali and Bale Zone of Oromia Regions
Submission Date: 03 April 2019
Percent of water points developed, - - 100%
repaired, or rehabilitated with free
residual chlorine (FRC) > 0.2 mg/L
Custom Indicator
Number of water points repaired and - - 6 Determined by
rehabilitated feasibility study to
be carried out by
Save the Children
and the Woreda
Water Office
% of people who have access to 90%
improved safe drinking water
Gender Analysis and Mainstreaming: Much of the differences in vulnerabilities in disaster
situations in the Oromiya and Somali regions can be attributed to the division of labor and
discriminatory social norms based on gender in the geographical area. Girls and women
are the most affected by the reduced access to water and other WASH services as it
increased their burden at the household level to collect water. Displaced women and girls
are also more vulnerable to violence (including sexual violence) from other IDPs and host
communities. Additionally, displaced women and girls are also the main victims of conflict
between IDP and host communities as a result of limited resources. More critically, the few
number of latrines in the IDP camps has not been sex-disaggregated and has not provided
the privacy and safety that women and girls require. Moreover, menstrual hygiene
management services for adolescent girls and women are non-existent.
Compounding these gender-based inequalities, women and girls often are inhibited from
voicing their views in public to articulate their specific interests and needs to improve their
access to WASH services. As a result, their WASH needs and related safety concerns
remain unaddressed.
The proposed action is designed to address the above gaps by targeting the most
vulnerable gender and age groups through lifesaving emergency water, sanitation and
hygiene (WASH) services. In its WASH activities, the intervention will take into account
distance of transporting water, which is usually the responsibility of girls and women. The
location of all water points and systems will be situated in places that do not increase the
- 36 -
Save the Children | Emergency WASH and Nutrition response to conflict affected IDPs and host communities in
Dawa, Shebelle, Korahe Zones, of Somali and Bale Zone of Oromia Regions
Submission Date: 03 April 2019
risk of violence of harm while accessing these facilities. The safety and privacy of girls,
women and other vulnerable groups will also be taken into consideration in the
construction of gender-segregated latrine with hand washing facilities. Moreover, the
participation and leadership of IDP and host community women in WASH Committees will
be ensured by ensuring at least 50% of the members are women.
SC will work with communities to articulate our planned interventions and mission with an emphasis
on gender inclusive programming. SC will work to ensure that the participation of all community
groups in general cleaning campaigns are in line with the local context and cultural acceptance, and
both women and men will be involved equally in committees. SC will consult project beneficiaries
about proper time for meetings and cleaning campaign days to reduce the burden on community and
ensure maximum participation. Through WASH, Nutrition and Protection clusters, we will
advocate with other agencies for a coordinated approach with regard to preventing IDPs from
risk.
Inclusion of Persons with Disabilities and Older People: SC will ensure that vulnerable
groups are included in project design and implementation, and that older persons and persons
living with disabilities are able to receive assistance at a location and distance that is convenient
and safe for them. SC will conduct regular monitoring of program implementation and will
ensure that timely and appropriate actions are taken where needed. This project will ensure all
infrastructures built or rehabilitated will be accessible to those living with disabilities.
Community-based targeting of beneficiaries will be carried out to ensure vulnerable households
are given priority in assistance.
Protection Mainstreaming in Sector Activities: In Somali and Oromia region, women and girls
are most affected by limited access to safe water sources, as they are the main water collectors
in the household. Drought conditions exacerbate the risk of gender based of violence and other
protection concerns as women and girls are forced to walk further distances to collect water. The
provision of water directly to communities aims to reduce the protection concerns associated with
water collection during drought. Staff involved in water trucking and water infrastructure activities
will be familiarized with child safeguarding policies. Staff and volunteers will be trained on Child
Safeguarding and how to identify vulnerable/at risk children in need of Child Protection
interventions.
Exit Strategy: A phasing out plan that will look at all sustainable water supply options will be
drafted at the beginning of the project with the communities, the local MoH, and local water offices.
It will consider adaptation measures to the climate change and growing water demand. Save the
- 37 -
Save the Children | Emergency WASH and Nutrition response to conflict affected IDPs and host communities in
Dawa, Shebelle, Korahe Zones, of Somali and Bale Zone of Oromia Regions
Submission Date: 03 April 2019
Children will actively advocate with government stakeholders to prioritize health facilities for water
provision and improved water storage and treatment supplies following the completion of the
project.
Exit strategy for rehabilitated water schemes: SC will work closely with the Local Water Office and
the WASHCO along the project cycle (as described in section above) with the aim of making the
system more sustainable. The training and accompanying activities will focus on identification and
management of the preventable problems (preventive maintenance) and simple repairs, financial
sustainability through cost recovery (for operation and preventive maintenance) and financial
management. The WASHCO will be enabled to access the market of spare parts and have a
contact at the Water Office for any issue beyond their capacity. We will ensure Regional and Local
Water Offices are making the possible to replenish their chlorine stock with their own budget
(water purification chemicals for supporting both systems -bulk chlorination- and households in
case of AWD or diarrheal disease outbreak).
Exit strategy for water trucking services to IDP locations: the exit plan will be discussed at the
early stage of the project with the primary stakeholders –local authorities, and partners. The
rehabilitation of water systems will be implemented in priority for the usage of water trucking
beneficiaries –within or in the vicinity of the community. Save the Children will systematically
implement all activities together with local stakeholders, particularly with the local government
structures, build their capacity. Towards the end of the response period, Save the Children will
hold a specific workshop for handover and develop a plan that will take into consideration the
specific context and availability of resources including the capacity of local systems and/or other
stakeholders also working in the affected location(s), and continued needs. An exit workshop at
the end of the project period will be held to present and hand-over project activities and
achievements, and discuss ways forward and follow-up action required to sustain gains. SC will
work closely with the regional Clusters, the respective government water offices and the
WASHCOs on elements of sustainability and quality of the system.
Exit strategy for water trucking to HCF: SC will be analysing on case-by-case a more sustainable
solution with the HCF team, local authorities, and the population served by the HCF as a local
solution could be possible. A decision-assisting tool (a decision tree) will be designed and used
for each health facility to make sure WT service is not triggered without robust evidence that all
other options are exhausted. The 60 days of duration was defined based on experience from
previous projects, and may vary from one HCF to another one from IDP to IDP. A weekly
monitoring will inform on the need for the following week, and on other water supply option that
could be resumed to the supply the facility. We will work with the HCF staff: make sure the HCF
director and nurses prioritize the search for water supply solution, but also encourage them to be
- 38 -
Save the Children | Emergency WASH and Nutrition response to conflict affected IDPs and host communities in
Dawa, Shebelle, Korahe Zones, of Somali and Bale Zone of Oromia Regions
Submission Date: 03 April 2019
a model to their staff and patients with regards to handwashing with soap and infection prevention
& control; we will train the janitor(s) and the identified water operator on basic water quality
treatment and surveillance (and other hygiene & IPC related topics). In collaboration with Health
and Nutrition stakeholders and colleagues, the priority facilities will be supported for case-by-case
water supply solutions in the exit stage –looking at all options including reliability of a nearby water
source and the potential for upgrading basic RWHS as above described- and we will advocate
and fund-raise to support them to be more climate resilient.
Exit strategy for household water chemical distribution: as the rehabilitation of water systems will
be implemented in priority for the usage of beneficiaries of the HH water chemicals (within the
community or in the vicinity), it is expected that this group will have resumed access to a protected
water point. Moreover, the project will explore the availability of local bleach for the purification of
non-turbid water. Finally, in the case the situation cannot be improved for some communities –
meaning the community still rely on turbid water and need PUR sachets- SC will intensively
advocate for this group to find a solution with local and regional stakeholders.
Exit strategy for the capacity building of WASH Committees: Establishing and strengthening
community-level ownership of and responsibility for the program and its interventions is essential
to long-term sustainability of water supply systems. Communities, local authorities and leaders
will be involved in the design and planning of activities to address the needs/gaps considered to
be prioritized. This will enhance buy-in to the interventions and increase understanding of the
value of the investment in both physical system and system strengthening, and the importance to
adhere and sustain the processes (cost recovery, adherence to the operation and preventive
maintenance plan, ask support to authorities when there are signs of major failures). SC will
clearly communicate the scale and scope of the proposed program with all stakeholders, including
the timeframe, to manage expectations. Roles and responsibilities during and after the project will
be also defined together with beneficiaries, authorities and leaders. The exit process will be
shared in advance to facilitate a gradual handover of program components to community
structures and partners. In order to sustain their activities, the existing and new WASHCO will be
informed on the role of their Woreda Water Office, which is responsible for managing and advising
WASHCOs. We will enhance the links between WASHCO members and Water Office officers.
The committees will be expected to report heavy repairs to government institutions for adequate
response.
Sub-sector 2: Sanitation
Technical description: This intervention aims to address the acute emergency needs regarding
sanitation facilities in the target areas, and thereby reduce exposure of communities to health
risks. SC will focus on mobilization of communities to ensure proper latrine use, which will be
- 39 -
Save the Children | Emergency WASH and Nutrition response to conflict affected IDPs and host communities in
Dawa, Shebelle, Korahe Zones, of Somali and Bale Zone of Oromia Regions
Submission Date: 03 April 2019
carried-out by the trained community hygiene volunteers. SC will construct 14 gender-separated
latrines. The target beneficiaries will be women and children headed households, poor
households and households including people with disabilities. The beneficiaries will be selected
thorough assessment, in consultation with local community members, community-based
volunteers, and gender-balanced WASH committees, to identify the most vulnerable people.
Selection criteria will be driven by vulnerability criteria.
For enhancement in protection and dignity, sanitation facilities will be located in close proximity
to households, with each household accessing a designated, yet shared latrines. Latrines will
have lockable doors (inside), a long-lasting superstructure (starting at 3m x 3m x 2.95m
height), vent pipe with fly screen, and a slab with sewer type slanting towards the pit.
Communal latrines will be shared by a maximum of four households, depending on the
household size (with one toilet being shared by maximum of 20 people in line with SPHERE
standards). Latrines will be constructed at least 30 meters away from any groundwater
source, and the bottom of any latrine will be at least 1.5 meters above the water table. The
design of the latrine is meant to reduce the risk of SGBV incidents, as it is lockable and
close to the households that will use it. The construction sites of the latrines will be
selected in collaboration with the community representatives, especially those with
mobility restrictions, and women and children who are typically the most at risk of SGBV
when using communal latrines, as well as in collaboration with the local authorities.
Building on learning from our experience providing WASH services in Somali region, Save
the Children will establish a separate volunteer hygiene and sanitation group who will be
in charge of daily maintenance of the sanitation facilities as well as disseminating hygiene
promotion messages within the community. The community volunteers in charge of
cleaning the latrines will be members of the already formed hygiene promotion team and
as an exit strategy; the WASH team will encourage full ownership of the facility by the
community members and ensure that the constant cleaning continues overtime.
The proposed latrines are semi-permanent communal latrines. The semi-permanent
latrines are chosen because of the government plan to resettle the IDPs to their place of
origin. Therefore, temporary solution is planned until the resettlement of the IDPs. The
semi-permanent latrines are more appropriate to the emergency context because of their
simplicity, quick/easy to construct by local people, and generally are inexpensive. It is not
feasible to provide individual household latrines due to cost, settlement pattern, and land
availability for latrines construction. From past experience in the region, the semi-
permanent communal latrines is expected to serve the community for one year, with one
block of 4 seat toilet for 80 individuals as per SPHERE standard (1:20); SC assumes the
IDPs will resettle to their original place after a year. If the communities are expected to stay
more than a year, SC will try to extend the lifespan of the toilet by emptying the latrines
with mechanical desludging. Save the Children will advocate the municipality or other
partner to do the desludging work. In an event where desludging is unforeseeable,
- 40 -
Save the Children | Emergency WASH and Nutrition response to conflict affected IDPs and host communities in
Dawa, Shebelle, Korahe Zones, of Somali and Bale Zone of Oromia Regions
Submission Date: 03 April 2019
decommissioning of all site infrastructures will be carried out and plans to construct new
permanent latrines will be established in order to prevent unauthorized removal of
reusable and valuable resources and minimize public health associated risks to the host
population and hosting environment. Latrines will be decommissioned / backfilled in a safe
and effective manner, by chlorinated lime then fill the entire surface of the pit with soil and
sand. The trained volunteers will be involved in the whole process through mobilizing
communities. Save the Children will not promote or carry out manual desludging of the
pits.
Latrine designs will also take account of easy access for children and people with disabilities,
through provision of entrances that are not high off the ground, and provision of accessible ramp
and hand washing facilities etc.
The beneficiaries will take responsibility for operation and maintenance of the latrines, which will
help the program to have a smooth exit and contribute to sustainability. In order to enhance
community ownership, beneficiaries will be mobilized to handle the decommissioning work. When
latrines are full, latrines will be decommissioned / backfilled in a safe and effective manner, by
chlorinated lime then fill the entire surface of the pit with soil and sand.
Construction of gender separated latrine: To ensure access to safe excreta disposal facilities,
Save the Children will construct 14 blocks of semi-permanent, gender-segregated latrines
equipped with hand washing facilities in the target IDP sites. Each block will have 4 seats and
each seat will serve 20 people, thus 80 people will benefit per block.9 Latrines will be equipped
with ramps to ensure accessibility for people with disabilities. Save the Children will conduct site
selection with the full participation women and girls to ensure access, safety and protection
concerns are adequately considered. During the construction phase, the Save the Children
WASH Officer and Coordinator will regularly supervise the work to ensure proper execution.
Indicator Type Target Remark
Male Female Total
Mandatory Indicators
Number of people directly utilizing 571 549 1,120 Sphere standard for
improved water services provided with one toilet for 20
OFDA funding people
9 20 people per seat is compliant with SPHERE standard.
- 41 -
Save the Children | Emergency WASH and Nutrition response to conflict affected IDPs and host communities in
Dawa, Shebelle, Korahe Zones, of Somali and Bale Zone of Oromia Regions
Submission Date: 03 April 2019
Percent of households targeted by - - 100
latrine construction/promotion program
whose latrines are completed and
clean
Average number of users per 20 Sphere standard for
functioning toilet one toilet for 20
people
Custom Indicator
Number of Gender separated latrine - - 14
with hand washing facility constructed
% of target beneficiaries who report 90%
improved sanitation practice
Gender Analysis and Mainstreaming: Save the Children will consider the needs of girls, boys,
women and men in the designs and site selection for latrines. Save the Children will
install/construct communal latrines segregated by gender and installed in sites close to
tents/shelter to reduce the risk of protection issues such as gender-based violence. For communal
latrines, clear signs for men and women will be placed and users will be informed about location
of the gender specific latrines.
Inclusion of Persons with Disabilities and Older People: The construction of latrine will take
account of easy access for children and people with disabilities, through provision of entrances
that are not high off the ground, and provision of accessible ramp and hand washing facilities etc.
Protection Mainstreaming in Sector Activities: Save the Children will ensure that women and
girls participate in needs assessments and that their risks and needs are clearly captured and
subsequently addressed. Save the Children will provide gender -segregated latrines and the sites
of latrines will be carefully selected so as to reduce women and girls’ vulnerability and prevent
protection and safety related issues. Save the Children will consider the needs of girls, boys,
women and men in the designs and site selection for latrines. Save the Children will construct
communal latrines segregated by gender and installed in sites close to tents/shelter to reduce the
risk of protection issues such as gender based violence.
Exit Strategy: Save the Children will establish a volunteer hygiene and sanitation group who will
be in charge of daily maintenance of the sanitation facilities as well as disseminating hygiene
promotion messages within the community. The community volunteers in charge of cleaning the
latrines will be members of the already formed hygiene promotion team and as an exit strategy;
- 42 -
Save the Children | Emergency WASH and Nutrition response to conflict affected IDPs and host communities in
Dawa, Shebelle, Korahe Zones, of Somali and Bale Zone of Oromia Regions
Submission Date: 03 April 2019
the WASH team will encourage full ownership of the facility by the community members and
ensure that the constant cleaning continues overtime.
Sub-sector 3: Hygiene Promotion
As poor sanitation leads to the potential contamination of water sources and spread of water-
borne diseases, it is essential to link hygiene education with both water supply and sanitation
interventions to increase the impact of each activity. Save the Children’s hygiene promotion,
response focuses predominantly on the three key hygiene practices (safe excreta disposal,
handwashing at critical times, house hold safe water storage and treatments) throughout the
project period. Community Hygiene Promoters will carry out regular hygiene promotion in the
target communities with supervision from Save the Children WASH staff and woreda health
offices. Hygiene promotion activities will utilize communication materials jointly developed by
WASH and Nutrition sectors, which clearly link poor hygiene practices with disease and
malnutrition. Hygiene promotion activities will be designed in-line with the National Emergency
Task Force’s response plan, and will be developed in close collaboration with the woreda water
and health offices to ensure an integrated approach. To complement health workers (and/or
supplement, where necessary), Save the Children will select and train additional volunteers in
each affected kebele to support community-based hygiene promotion activities, utilizing existing
WASH committees and other community groups (including women’s groups) where appropriate.
The Knowledge, Attitude and Practice (KAP) survey at the beginning and the end of the project
will measure behavior change as a result of the interventions. In order to eliminate bias, prudent
actions will be undertaken regarding designing the survey and questions to be
administered. Specifically, a well‐designed and compressive questionnaire will be
prepared in addition to the Knowledge, attitude and practices that verifies presence of
hand washing facilities in the house, Uncontaminated or chlorinated water in HH
storage. Besides, technical team (both WASH and MEAL team) from Country office will
lead and guide the survey process which in turn augments the quality of the survey.
Campaign Event: SC will undertake a mass hygiene and sanitation campaign for target
beneficiaries and health facilities, focusing on key hygiene messages including environmental
cleanliness and handwashing at critical times. WASH committees, trained volunteers, janitors,
and local community groups will be mobilized to conduct this campaign with participation of
communities including vulnerable groups. Traditional and folk media methods will help reach
worst-affected households with key and lifesaving health and sanitation messaging. Health
Facilities staff will be engaged to ensure the cleanliness and routine maintenance of latrines. To
ensure the effectiveness of key messages, at least four events will be organized in each target
kebele during the project period along with confirming all health facility latrines have adequate
cleaning supplies and disinfectant. SC will work closely with the Woreda Health Bureaus on this
component to ensure its sensitivity to the local context.
- 43 -
Save the Children | Emergency WASH and Nutrition response to conflict affected IDPs and host communities in
Dawa, Shebelle, Korahe Zones, of Somali and Bale Zone of Oromia Regions
Submission Date: 03 April 2019
IEC Material printing and Distribution: IEC materials will be distributed to target households to
ensure information is disseminated in an effective and targeted manner. The materials will be
accessible, combining imagery and local language to address key points of health education,
(posters focusing on the three key hygiene practices developed and distributed to households).
Indicator Type Target Remark
Male Female Total
Mandatory Indicators
Number of people receiving direct 26,775 25,725 52,500
hygiene promotion (excluding mass
media campaigns and without
double-counting)
Percent of households targeted by 65%
the hygiene promotion program who
store their drinking water safely in
clean containers
Percent of people targeted by the 65%
hygiene promotion who know at least
three (3) of the five (5) critical times
to wash hands
Custom indicator
Number of health facilities received 25
WASH cleaning supplies
% of targeted community who 65%
practice handwashing at critical
times
Gender Analysis and Mainstreaming: SC will ensure that both men and women are represented
on Community Hygiene Volunteers teams. The hygiene and sanitation promotion activities are
designed to address the specific needs of women and girls, including menstrual hygiene.
- 44 -
Save the Children | Emergency WASH and Nutrition response to conflict affected IDPs and host communities in
Dawa, Shebelle, Korahe Zones, of Somali and Bale Zone of Oromia Regions
Submission Date: 03 April 2019
Inclusion of Persons with Disabilities and Older People: Hygiene promotion activities will be
accessible and relevant to all community members, including persons living with disabilities and
the elderly. IEC materials will be developed in both visual representations and in text, in addition
to being expressed verbally to ensure persons with seeing, hearing or learning difficulties are able
to understand. Where possible, persons living with a disability will be encouraged to participate in
Community Hygiene Volunteer teams and/or Health Development Armies to promote
empowerment, increase acceptance, and address the unique needs of persons with
vulnerabilities.
Protection Mainstreaming in Sector Activities: Public hygiene promotion sessions will be
designed to take place at a time and location accessible to and safe for all members of the
community. All community mobilisers undergo background checks and child safeguarding
sensitization. Staff and volunteers will be trained on Child Safeguarding and how to identify
vulnerable/at risk children in need of Child Protection interventions. Community feedback
mechanisms are designed to allow for anonymous feedback and reporting of any issues, which
are then followed up on a case-by-case basis.
Exit Strategy: This project is designed to address critical, immediate and short-term needs, but
also to build the resilience of the affected population to better cope with water and nutrition crises
in the future. Awareness raising will contribute to improved nutrition and hygiene practices, and
prevent malnutrition and fecal-oral diseases, a key aggravating factor of malnutrition.
Sub-sector 4: WASH Non-food Items
Technical description: Save the Children will distribute 2180 hygiene kits (WASH NFIs) to SAM
patients and IDP sites to encourage and facilitate improved hygiene practices and reduce the
likelihood of diarrhea and subsequent malnutrition. WASH NFIs will be provided according to
WASH cluster guidelines and SHERE Minimum Standards, and will contain jerry cans for safe
collection and storage of drinking water, water treatment chemicals for treating drinking water,
and soap to promote hand washing at critical times and dignity kit. WASH NFIs will last for 2
months. Each household will receive 1 jerry can and 1 bucket and each family member10 will
receive two bars of soap per month (four total).
In line with the WASH in Nutrition 3-pillar strategy (facility, household, community), we will
provide special WASH attention to families with SAM treated children through distribution
of hygiene kits and household hygiene promotion. Save the Children will distribute a total
of 2180 hygiene kits (WASH NFIs) with 1880 to SAM patients enrolled in nutrition program
and 300 to IDP sites, 250 SAM children and 50 people affected by flood to encourage and
facilitate improved hygiene practices and reduce the likelihood of diarrhea and subsequent
malnutrition.
10 Based on an average family size of 6 members.
- 45 -
Save the Children | Emergency WASH and Nutrition response to conflict affected IDPs and host communities in
Dawa, Shebelle, Korahe Zones, of Somali and Bale Zone of Oromia Regions
Submission Date: 03 April 2019
At IDP site, the most at risk of WASH facility collapse are reached and provided hygiene
kit. In this process, community leaders, kebele leaders, and local development committee
members will be involved. WASH sector offices play key roles and technical backstopping
while project staff will facilitate the process. To the extent, possible targeting processes
will be quite transparent and those most needy are screened in reference to the set criteria
for each of the activities to be implemented. The following beneficiaries’ selection criteria
are proposed to be considered.
Site selection:
Community size: larger communities deprived of water and/or sanitation functional
facilities/services will be prioritized.
Unassisted IDP communities: IDPs who did not receive any assistance or are newly
/ secondarily displaced.
Communities with disrupted access to WASH markets (for soap, jerrycans, etc…)
Beneficiary selection:
among the priority communities, the priority households are: female-headed households,
Child headed households, large families with more than 5 children (under 18 years old),
Households with at least one disabled or chronical acutely ill person, Households with at
least one elderly person, Households that include pregnant or lactating women and
malnourished children, Household with children have contracted AWD frequently.
Moreover IDP families unable to access to basic WASH NFI due to high poverty will also
be considered. Following on from these criteria, the identified communities will select a
targeting committee and appeal Committee at kebele level, If there is any dissatisfaction
and/or exclusion among the community/individuals, a complaint can be brought to the
appeal committee for verification and adjustment; if the appeal is legitimate, the appealing
person / family will be included where possible.
Distribution of hygiene items will be undertaken according to the AWD seasonality calendar to
prevent outbreaks. In the event of an AWD outbreak, the project team will access prepositioned
supplies from Regional Supply hub and will coordinate with other WASH partners to ensure
effective response. Save the Children will conduct practical demonstrations for all beneficiaries
on use of distributed hygiene items. A post-distribution monitoring survey will be carried out
following distribution to evaluate beneficiary satisfaction and the appropriateness of hygiene
items. Complaint Reporting Mechanisms will be established prior to distribution to monitor
beneficiary satisfaction.
Indicator Type Target Remark
- 46 -
Save the Children | Emergency WASH and Nutrition response to conflict affected IDPs and host communities in
Dawa, Shebelle, Korahe Zones, of Somali and Bale Zone of Oromia Regions
Submission Date: 03 April 2019
Male Female Total
Mandatory Indicators
Total number of people receiving 13,080
WASH NFIs assistance through all
modalities (without double-counting)
Percent of households reporting 70%
satisfaction with the contents of the
WASH NFIs received through direct
distribution
Percent of households reporting 70%
satisfaction with the quantity of WASH
NFIs received through direct
distribution
Number of WASH NFI kits distributed 2,180
Custom indicator
% of targeted beneficiairies who 90%
report the quality of WASH NFI
distributed
Gender Analysis and Mainstreaming: Save the Children acknowledges the different roles and
responsibilities played by children, women, and men in the target areas. Typically, men are
responsible for the provision and allocation of resources in the household; however, men, women,
and children will attend NFI distributions. Save the Children, staff will ensure that beneficiaries
will not experience any discrimination at distribution sites and that the needs of women and
children are accounted for beneficiary selection criteria are based on levels of vulnerability as
identified through partners.
Inclusion of Persons with Disabilities and Older People: Save the Children and its partners
have strict policies of non-discrimination including against older people or persons with disabilities
and will strive to provide equal access to services. Appropriate assistance will be given to people
with disabilities and the elderly who may not be able to easily carry distributed goods.
- 47 -
Save the Children | Emergency WASH and Nutrition response to conflict affected IDPs and host communities in
Dawa, Shebelle, Korahe Zones, of Somali and Bale Zone of Oromia Regions
Submission Date: 03 April 2019
Protection Mainstreaming in Sector Activities: Save the Children will distribute WASH NFIs to
SAM children and their families to avoid the possibilities of relapse. As much as possible,
distribution sites will be accessible and appropriate for children, girls to protect them from all
hazards.
Sector 2: Nutrition
a) Sector Objective: Sustainable preventive and curative services in the management of
acute malnutrition are delivered through government systems.
b) Dollar Amount: $2,136,339 USD
c) Beneficiary Numbers: 56,551 (36,685 U5, 19,866 PLW), Total SAM-2,402 (482 at SC and
19,820 in OTPs), Total MAM – 56,551 (36,685 U5, 19,866 PLW)
Total Number of people targeted: 56,551
d) Geographic Area: Dawa (4 Woredas), Korahe (3 woredas), Shebelle (3 Woredas) Zones of
Somali Region and Bale (5 IDP Woredas) of Oromia region, Ethiopia
e) Sector Level Coordination: The project activities will be planned and implemented in
collaboration with the respective RHBs, WrHOs, DPPBs, Women and Children Bureaus, and
UN agencies (UNICEF, WHO, and WFP). Save the Children have submitted letter of interest
to WFP for 2019 new Field Level Agreement (FLA) for TSF commodity for the target woredas
in Somali and Oromia regions. Project staff will actively participate and share updates on
woreda and zonal level coordination meetings and share meeting notes and concerns with
project leads at regional levels. Nutrition program coordinators based in Bale (Oromia) and
Doloado and Gode (Somali) will participate in regional level Nutrition Cluster meetings in
Oromia and Somali regions, respectively. They will regularly update the Cluster on SC
progress, share best practices, lessons, and challenges contributing to regional level learning
and supporting coordination efforts. Minutes from Cluster meetings will be shared with the
nutrition team in Addis Ababa for guidance and technical support to ensure quality of services.
Nutrition experts who represent SC at Multi-Agency Nutrition Task Force (MANTF)
coordination meetings will continue to use the forum to exchange information from the field
on the progress, challenges and lessons learned from this project. They will also keep the
field staff informed of MANTF’s decisions and guidance, if any, related to the respective
regions in general and/or the specific project in particular.
f) Keyword: Pastoralists
- 48 -
Save the Children | Emergency WASH and Nutrition response to conflict affected IDPs and host communities in
Dawa, Shebelle, Korahe Zones, of Somali and Bale Zone of Oromia Regions
Submission Date: 03 April 2019
Keyword Integration: Pastoralists and agro-pastoralists are core beneficiary groups for the
proposed nutrition intervention
g) Technical Design:
Sub-sector 1: Infant and Young Child Feeding in Emergencies
Technical description: Infant and Young Child Feeding in Emergencies (IYCF-E) safeguards
the health and wellbeing of children under two years. This project will support mothers and
caretakers to protect and improve breastfeeding practices in the current drought and
displacement emergency, and enhance knowledge on key infant and young child feeding and
caring practices. SC will support six breastfeeding corners (three in Shebelle and three in Korahe)
to create a safe and private environment for breastfeeding and also provide support to mothers
with breastfeeding difficulties and individualized counseling by trained health workers. There are
already breastfeeding corners established in Dawa (through IRC/OFDA funding) and Bale zones
(through UNOCHA funding) and thus, SC will only be supporting breastfeeding corners that are
not supported by other projects. Save the Children will support 45 mother-to-mother support
groups (MtMSGs) through provision of meeting refreshments and guidance on discussion topics
to encourage the sharing of best practices. Groups will be formed within the first weeks of project
implementation and 8-week sessions on optimal IYCF-E practices will be provided. Save the
Children will establish or strengthen 45 mother-to-mother support groups (MtMSG) (an
estimated 15 mothers per group) to promote optimal infant and young child feeding (IYCF).
The mother-to-mother support groups will be established 1 per selected Kebele in the
target 15 woredas. In close coordination with local HEWs, one IYCF-E officer will be
deployed per woreda to establish, support and monitor the MtMSG. The IYCF-E officer has
a responsibility to follow and support the routine activities of MtMSG and ensure MtMSG
session are conducted as planned. In addition, the CMAM program coordinators at woreda
level will monitor the implementation of the MtMSGs during the periodic woreda and SCI-
integrated supportive supervision visits.
Save the Children has been implementing IYCF-E include community level interventions such as
MtMSGs through previous emergency nutrition projects. To be resource efficient and ensure the
quality of the intervention adding up the ongoing government effort on IYCF-E, SC proposed to
support 45 MtMSGs in the target Woredas, prioritizing Kebeles/IDP sites based on the level of
need and locations, which were not prioritized in previous projects. Like other activities, selection
of IDP sites/Kebeles for MtMSG intervention will be coordinated with local authorities and as
criteria, Kebeles/ IDP sites with poor access to health facilities, continued higher level of acute
malnutrition rates (relative higher rate of proxy GAM and SAM admission) and sub-optimal IYCF
practices will be considered. SC understand the importance of linkage between IYCF-E
(breastfeeding) corners at health facilities and MtMSGs. The MtMSGs session will be facilitated
- 49 -
Save the Children | Emergency WASH and Nutrition response to conflict affected IDPs and host communities in
Dawa, Shebelle, Korahe Zones, of Somali and Bale Zone of Oromia Regions
Submission Date: 03 April 2019
by the respective Kebele Health Extension Worker and on the initial phase of the project HEWs
will be trained on IYCF-E (which is proposed in this document) to help them facilitate the MtMSGs,
identify and refer mothers with breast feeding difficulties to health facilities with IYCF-E corners
or nearby health facility for further intervention. SC IYCF nurse with the catchment health center
staff will also provide regular supportive supervision to ensure quality in the implementation of
routine activities of MtMSGs.
Promotion of optimal IYCF and proper hygiene and sanitation practices will be integrated into all
CMAM activities (OTP, tSFP, and SC) at all service sites with behavior change messages using
nationally accepted and culturally appropriate tools. Existing IEC/BCC materials from previous
projects will be distributed to service sites. The promotional activities and materials will target
PLWs, caretakers of children with SAM/MAM, and other influential community members.
Community volunteers will be trained and equipped to facilitate messaging and promotion of
optimal practices and healthy behaviors, while SC’s IYCF officers will supervise and support the
work of volunteers to ensure the quality of the promotional sessions. Messages will primarily focus
on IYCF practices including optimal breastfeeding, appropriate complementary feeding, proper
personal hygiene, and prevention of common childhood illnesses. Since the proposed WASH
interventions will only be implemented in 8 out of the 15 woredas, Save the Children will leverage
on the other existing funding streams to ensure a comprehensive WASH-in-nutrition support in
the remaining 7 woredas.
Indicators
Indicator Type Baseline Target Remark
Mandatory Indicators
Proportion of infants 0-5 months of age who 45.1% 54%
are fed exclusively with breast milk
Proportion of children 6-23 months of age 9.95 11.5%
who receive foods from 4 or more food
groups
Number of people receiving behavior change 76,639
interventions to improve infant and young individuals
child feeding practices
Custom Indicators
Number of mother to mother support groups 45
established/strengthened and supported
Number of breastfeeding corners established 30
and supported
- 50 -
Save the Children | Emergency WASH and Nutrition response to conflict affected IDPs and host communities in
Dawa, Shebelle, Korahe Zones, of Somali and Bale Zone of Oromia Regions
Submission Date: 03 April 2019
Sub-sector 2: Management of Acute Malnutrition
Technical description: Routine medication and treatment of acute malnutrition will be provided
to children under the age of five with severe and moderate acute malnutrition (SAM and MAM) in
line with the national guidelines for the community management of acute malnutrition (CMAM).
The CMAM package includes a therapeutic feeding program (TFP) consisting of a stabilization
center (SC) and an outpatient therapeutic program (OTP), and a targeted supplementary feeding
program (tSFP). This service package is accompanied by capacity building and community
mobilization activities to enhance quality and coverage. Below is a technical description of the
approach, processes, and criteria for CMAM.
Therapeutic Feeding Program: Stabilization Centers (SC)
This component will support children with SAM and medical complications, poor appetite, and/or
bilateral pitting edema. Based on recent operational experience, Save the Children anticipates
12% of children with SAM will require admission to stabilization centers for 24-hour care until their
condition is stabilized. These children are expected to stay in the SCs for 5-8 days before they
are discharged for follow-up at the nearest OTP site. SCs are located in health centers (and
hospitals) and the WrHOs will be responsible for assigning health workers and support staff for
24-hour care of children. The project will deploy an SC nurse who will provide on-job training and
technical support for proper care according to national protocol.
Cooked meals will be provided to caretakers of children admitted to SCs to ensure that they stay
with their children for the duration of treatment so as to prevent defaulting. SC will ensure food for
caretakers of children admitted to SCs is cooked food, prepared from locally available food
commodities certified by the Ministry of Health for use in the facility; and in adherence with ADS
312. This has proven to reduce default rates as mothers and caretakers will not have to walk back
home to feed themselves, thus they’ll be able to provide 24 hour-care to their malnourished
children. Save the Children will ensure the highest hygiene standards in food preparation, similar
to the preparation of F-75, F-100 and appetite test within the Stabilization Center. The provision
of cooked meals to caretakers also provides an opportunity to practically demonstrate
handwashing, safe food handling, preparation and feeding practices to caretakers, which they
can apply at home upon discharge from the SC. Three cooked meals will be provided per day to
caretakers. The number of meals provided will be verified by the Health Center Medical Director
and the Save the Children SC Nurse based on the registration log at the Health Center. Storage
and disposal will be in accordance with the existing health facility waste disposal practices. Based
on the guidance from regional ENCU, the price for meals is calculated at $7/day.
SC admission criteria:
Children U5 with SAM: MUAC <11 cm and/or WFH <70% and/or bilateral pitting Oedema
(++ or +++) and with medical complications and poor appetite.
- 51 -
Save the Children | Emergency WASH and Nutrition response to conflict affected IDPs and host communities in
Dawa, Shebelle, Korahe Zones, of Somali and Bale Zone of Oromia Regions
Submission Date: 03 April 2019
Mothers unable to lactate or infants that are too weak to suckle (for infants <6 months of
age irrespective of nutrition status)
SC Discharge Criteria:
Weight for length >85% is used as a discharging criteria for infants <6 months (for non-
breastfed)
No medical complications
Good appetite
Transfer to OTP criteria:
As soon as appetite returns, oedema starts to decrease, all medical complications resolve
Therapeutic Feeding Program: Outpatient Therapeutic Program (OTP)
The OTP component will provide medical and nutritional treatment for children with SAM with
good appetite, and no medical complications. Services are provided through weekly visits to
decentralized OTP sites located at health facilities (health posts and health centers). OTP
services are typically provided by health extension workers based at the health posts, but health
workers also provide the service in health centers. A CMAM officer and an OTP nurse deployed
by the project will be responsible for ensuring program quality, availability of supplies, reporting,
and joint supportive supervision with region/zonal woreda officials. Children admitted to the
program will undergo a thorough clinical examination by HEWs (or HWs) and will start the
standard systematic medical and nutritional treatment based on national protocol. Basic primary
care services, provided by the government with logical and technical support from Save the
Children, will also be provided routinely as part of the protocol.
OTP Admission Criteria:
Children with SAM: MUAC <11cm and/or WFH <70% and/or bilateral pitting Oedema (+
or ++) and NO medical complications and good appetite
OTP Discharge Criteria
Target weight gain reached (15% weight gain) for two consecutive visits
No oedema for 14 days
OTP to SC Transfer criteria:
Children who develop medical complications in the course of OTP treatment or who failed
the appetite test during any follow up visit
- 52 -
Save the Children | Emergency WASH and Nutrition response to conflict affected IDPs and host communities in
Dawa, Shebelle, Korahe Zones, of Somali and Bale Zone of Oromia Regions
Submission Date: 03 April 2019
Those who either lose weight in 2 consecutive OTP visits or fail to document weight gain
over 3 consecutive follow up visits;
Children who develop oedema while enrolled; and, those whose oedema grade worsens
Management of MAM: targeted Supplementary Feeding Program (TSFP)
The targeted supplementary feeding program (TSFP) will support children under five with
moderate acute malnutrition and PLWs. The project will use RUSF (Plumpy Sup) and CSB++
sourced from WFP as part of the national arrangement for TSFP programs. SC will strengthen
and actively support smooth referral linkages among TSFP, OTP, SC and community mobilization
activities through continuous technical and supervisory support. Save the Children will also
ensure quality beneficiary targeting through systematic and continuous monitoring of
measurements of weight, height, MUAC, and assessment of edema to maximize efficient use of
limited resources by minimizing inclusion and exclusion errors. Selection of TSFP sites will be
conducted in consultation with respective WrHOs, DPPOs, Women and Children Affairs Offices,
and the community to minimize risks associated with long distance walking to service sites11. The
TSFP sites will ideally be based in or nearby a health facility if distance and other protection
considerations are not an issue. The project will support mass screening jointly-conducted by
DPPB, RHB and WrHOs every three months to increase access and coverage services. SC will
facilitate joint supportive supervision by providing transport and per diem for relevant government
officials/experts from the region/zone/woreda.12 Moreover, SC will also be directly involved in
supporting the WrHO in documentation, compiling, and reporting of program activities from each
woreda.
SC will ensure that they are accessing services through continuous and systematic collection of
data, disaggregated by age and disability status, as a part of its program monitoring. Community
mobilization efforts will also ensure that this forms part of the awareness messages.
TSFP admission criteria:
Children with MUAC 11-12.5cm OR WFH ≥70% - <80%
Pregnant and lactating women with MUAC <23 cm
Children discharged from OTP
11
2018 Sphere standard: 90% of the target population takes less than a one-day’s return walk (including time for
treatment) to the program site.
12In principle, UNICEF has allocated funds to cover per diem and transport for government officials for routine
nutrition screenings. However, in practice, at the woreda level Save the Children and other partners are still receiving
requests from the government to cover these costs and without them government participation will drop.
- 53 -
Save the Children | Emergency WASH and Nutrition response to conflict affected IDPs and host communities in
Dawa, Shebelle, Korahe Zones, of Somali and Bale Zone of Oromia Regions
Submission Date: 03 April 2019
TSFP discharge criteria
Target weight reached (Weight gain of 13%) and MUAC ≥12.5cm in two consecutive visits
PLWs with MUAC ≥ 23 cm OR at 6 months post delivery
Children transferred from OTP will be discharged after 2 months
Linkages between tSFP, OTP and SC: Children discharged from SC will be transferred to the
nearest OTP using transfer forms established for the purpose. Similarly, children whose condition
warrant in-patient treatment while on OTP follow-up will be referred to nearby SC sites. Children
discharged from OTP will be linked to tSFP for consolidating their recovery. Similarly, children
whose nutritional status deteriorates while in tSFP will be referred to OTP. To facilitate these
linkages, tSFP and OTP sites will be established in close proximity to each other. Supplementary
food will be distributed adjacent to the target population to reduce risks and costs associated with
travelling long distance with young children and to reduce the number of children defaulting from
the program.
Community Mobilization: Community mobilization will raise awareness on the availability of
TFP/tSFP services and implementation modalities. Communities will be made aware of the
services available through community sensitization on the availability and benefits of nutrition
treatment services. This activity will be implemented through existing community communication
channels and volunteers. With technical support from the project, HEWs are expected to
coordinate and assist community volunteers to carry out community mobilization (sensitization,
active case-finding, defaulter tracing, and follow-up). Pastoralist communities will be reached by
increasing communication between service providers and community volunteers, and service
users will be properly transferred to other service sites adjacent to their new locations.
Capacity Building: Building local government capacity to plan, implement, and monitor
emergency nutrition services using the CMAM approach is a key focus area of this project. SC
will employ a combination of formal and on-the-job training approaches using the nationally
accepted training manual on CMAM and IYCF-E. The formal training will focus on health workers
and health extension workers that were not trained under the previous project and high number
of new staffs in the area due to rapid turnover. High turnover and low availability of staff is
one of the expected risks for this project, especially in Somali region. To reduce the impact
of the high turnover and build the capacity of the recently deployed new health
professionals, SCI will deliver continuous onsite CMAM mentorship and coaching at TFUs.
In areas where there is a severe shortage of health workforce, SCI OTP, SC and TSFP
nurses can directly support the provision of the routine services. In areas where there are
no HEWs, SC, in coordination with respective Woreda Health Offices, will select volunteer
community health workers and food distribution agents and provide them training on key
MAM management and IYCF-E messaging; these volunteers will support IYCF-E
promotion, screening and TSFP services. SC will use key performance indicators established
by the government and the Sphere Project to ensure quality of services.
- 54 -
Save the Children | Emergency WASH and Nutrition response to conflict affected IDPs and host communities in
Dawa, Shebelle, Korahe Zones, of Somali and Bale Zone of Oromia Regions
Submission Date: 03 April 2019
Community volunteers will be instrumental in improving coverage and utilization of services. SC
will re-train and deploy new and existing community volunteers on active case finding, defaulter
tracing, community mobilization, as well as promotion of optimal infant and young child feeding
practices to work along with and supported by the HEWs. Gender considerations will be included
as part of the selection criteria for identification, training and deployment of the volunteers.
IYCF-E and CMAM: To ensure integration of IYCF-E into CMAM, Save the Children will identify
appropriate and strategic contact points within the SCs, OTPs, TSFPs and community
mobilization activities to deliver key IYCF messages and identify mother-baby pairs who require
additional basic and/or skilled IYCF-E support.
Indicators
Indicator Type Category Target Remark
Male Female Total
Mandatory Indicators
Number of health care staff trained HWs 30 45 75
in the prevention and management
of acute malnutrition disaggregated HEWs 150 150
by sex
Number of supported sites SC 32 Somali:
managing acute malnutrition 28 OTP,
OTP 38 22 SC,
tSFP 219 TSF 175
Oromia
10 OTP,
10 SC,
and 44
TSF
Number of people admitted, rates of
recovery, default, death, relapse,
and average length of stay for
people admitted to Management of
Acute Malnutrition sites
Number of people admitted to TFP 10,354 9,948, 20,302
TFP (SC and OTP)
disaggregated by sex
- 55 -
Save the Children | Emergency WASH and Nutrition response to conflict affected IDPs and host communities in
Dawa, Shebelle, Korahe Zones, of Somali and Bale Zone of Oromia Regions
Submission Date: 03 April 2019
Indicator Type Category Target Remark
Male Female Total
TFP performance indicators: recovery >75% Sphere
rates of recovery, default, death, targets
relapse, and average length of default <15%
stay (ALS) death <3%
relapse
ALS SC= 5-
7days
OTP= <60
days
Number of people admitted to tSFP U5 18,709 19976 36,685
tSFP (U5, PLWs) disaggregated
by sex as appropriate tSFP - 19866 19,866
PLW
tSFP performance indicators: recovery >75% Sphere
rates of recovery, default, death, targets
and average length of stay default <15%
death <3%
ALS 3 months
Number of people screened PLWs 82,075
for malnutrition by
community outreach workers Children 140,780
U5
Custom indicators
Number of woreda health offices Supply 15
supported with supply chain and chain
nutrition information management
Nut info 15
Mgt
Gender Analysis and Mainstreaming: Internally displaced persons in the Somali and
Ormoiya regions are considered amongst most vulnerable population groups due to their
limited access to health services and food. Even though all IDP girls, boys, women and
- 56 -
Save the Children | Emergency WASH and Nutrition response to conflict affected IDPs and host communities in
Dawa, Shebelle, Korahe Zones, of Somali and Bale Zone of Oromia Regions
Submission Date: 03 April 2019
men are vulnerable to health risks and nutrition deficiencies, women and girls are
disproportionately affected by the persistent shortage of resources and lack of proper
health facilities as a result of their gender roles and responsibilities.
Moreover, increasing work burdens and discriminatory gender norms limit women and
girls’ mobility while increasing their dependency on aid. Discriminatory norms in both
regions deprioritize women and girls for access food, which lowers in availability in
emergency contexts.13 Lack of nutritional assistance and health services also adversely
affects children under five and pregnant and breast-feeding women.
The proposed disaster nutritional assistance targets pregnant and lactating women
(PLWs) and children under five in view of their special vulnerabilities. In doing so, the
proposed action strives to reduce existing inequalities in food and nutrition consumption
to the most vulnerable gender (PLWs) and age (children under five) groups. Moreover,
the proposed action works to bring change in discriminatory social norms regarding
breastfeeding and complementary feeding through behavioral change communication
targeting community girls, boys, women and men. The project also seeks to empower
women in community leadership and strengthen their social alliances by
establishing/strengthening mother-to-mother support groups.
Protection Mainstreaming: Save the Children will exercise the utmost care and ensure that
existing service sites do not pose risks to women and girls. Selection of new sites will be
conducted in consultation with the WrHOs, Woreda Women and Children Affairs offices, and
community leaders. Distance of the site from the village/community will be a key consideration.
Staff and volunteers will be trained on Save the Children’s Child Safeguarding policy to ensure
that the project does no harm to intended beneficiaries. As indicated in the project description,
beneficiary selection in CMAM programming is based on national guidelines. SC will employ a
confidential complaint system and actively encourage reporting of offenses as they occur.
Exit Strategy: Inherent within the design of this project are system strengthening and capacity
building efforts including trainings to be provided for HWs/HEWs, supportive supervision and
mentoring activities, and system strengthening of supply chain management and local data
management. These efforts are geared towards ensuring that the WrHOs (and the local system
overall) are capable of continued provision of life-saving services beyond the duration of the
project. A detailed exit plan will be presented and discussed with the RHB, Zonal and respective
WrHOs during the start-up workshop to ensure these entities are informed and engaged. An exit
workshop at the end of the project period will hand-over project activities and achievements, and
discuss ways forward and follow-up action required to sustain key program components. Save
the Children will work closely with the regional Clusters and the respective government offices to
analyze monitoring data (admission trends), the prevailing humanitarian situation, and forecasts
13(Oxfam International (July 2016) CONSOLIDATED GENDER ANALYSIS FOR THE ETHIOPIAN DROUGHT
RESPONSE: https://www.humanitarianresponse.info/sites/www.humanitarianresponse.info/files/documents/files/rr-
ethiopia-gender-echo-160916-en.pdf
- 57 -
Save the Children | Emergency WASH and Nutrition response to conflict affected IDPs and host communities in
Dawa, Shebelle, Korahe Zones, of Somali and Bale Zone of Oromia Regions
Submission Date: 03 April 2019
to justify its exit from these woredas. In the event exit is not justified, Save the Children, dictated
by the Humanitarian Imperative, may have to continue providing relief assistance conditional on
the availability of resources.
Transition and Exit Strategy
While this project responds to the immediate WASH and Nutrition, needs of conflict-affected
children and their families, it also provides the foundation for longer-term sustainable protective
and preventative measures by improving infrastructure, providing hygiene-related education and
promotion, and building the capacity of community-based mechanisms, caregivers and children.
The project will work closely with national partners and local communities to ensure long-term
sustainability and community ownership of the proposed interventions. Through working with local
government bureaus, SC will be able to rehabilitate existing infrastructure and build the capacity
of partners who will be able to, through community-based approach promote ownership.
Community volunteers, for example, ensure that the impact of this project lasts beyond the scope
of this timeline. Through the transfer of knowledge and tools, linkages to government structures,
and community training on how and why to adopt hygienic behaviors and how to prevent and
protect children from violence. Community members will be empowered to minimize WASH-
related health risks. SC prioritizes the capacity building of national staff, partners, and
stakeholders to ensure the sustainability of our program activities.
- 58 -
Save the Children | Emergency WASH and Nutrition response to conflict affected IDPs and host communities in
Dawa, Shebelle, Korahe Zones, of Somali and Bale Zone of Oromia Regions
Submission Date: 03 April 2019
Potrebbero piacerti anche
- Project Proposal On Water DR FinalDocumento50 pagineProject Proposal On Water DR FinalTesfaye DegefaNessuna valutazione finora
- Oil Seed ProjectDocumento40 pagineOil Seed ProjectJemal100% (1)
- International Finance Term Paper Roll 22 & 29 (44E)Documento17 pagineInternational Finance Term Paper Roll 22 & 29 (44E)Ahmed ZaheerNessuna valutazione finora
- Melkamu 1Documento53 pagineMelkamu 1melkamu meleseNessuna valutazione finora
- Strategic Plan - DFPCDocumento10 pagineStrategic Plan - DFPCJelly TineNessuna valutazione finora
- THE IMPACT OF REMITTANCES ON EthiopiaDocumento16 pagineTHE IMPACT OF REMITTANCES ON EthiopiaTariku WorkuNessuna valutazione finora
- Commented Ahmed Yaqob Research ProposalDocumento22 pagineCommented Ahmed Yaqob Research ProposalAbdusalam IdirisNessuna valutazione finora
- Chall Shamble Proposal EdditedDocumento22 pagineChall Shamble Proposal Edditedshegaw manNessuna valutazione finora
- GROUP-II ON METALS AND MINERALS - STRATEGY BASED UPON THE DEMAND AND ... (PDFDrive)Documento423 pagineGROUP-II ON METALS AND MINERALS - STRATEGY BASED UPON THE DEMAND AND ... (PDFDrive)jinan sahiraNessuna valutazione finora
- Private Enterprise For Public Health - Guide 2012Documento44 paginePrivate Enterprise For Public Health - Guide 2012ippfwhrresmobNessuna valutazione finora
- Economic Development and Post Covid-19: Reflections On The Global SouthDocumento7 pagineEconomic Development and Post Covid-19: Reflections On The Global SouthUnity HumanityNessuna valutazione finora
- AlfalfaDocumento7 pagineAlfalfaEvan Fred CagampangNessuna valutazione finora
- Chakatsva The Role of Microfinance Institutions in Poverty Alleviation in Developing EconomiesDocumento134 pagineChakatsva The Role of Microfinance Institutions in Poverty Alleviation in Developing EconomiesDenzel GotoNessuna valutazione finora
- Miyar Ahmed ProposalDocumento26 pagineMiyar Ahmed ProposalLeul100% (1)
- JAMIGA GLOBAL LTD - Furniture Business PlanDocumento36 pagineJAMIGA GLOBAL LTD - Furniture Business PlanfrankNessuna valutazione finora
- Ethnomedicinal Survey of Plant Used in TreatmentDocumento59 pagineEthnomedicinal Survey of Plant Used in TreatmentODUNTAN SULAIMONNessuna valutazione finora
- Low Cost Country SourcingDocumento31 pagineLow Cost Country SourcingDhaval DhruvNessuna valutazione finora
- Bio-Degradable Plastics-Proposal For Green TechnologyDocumento12 pagineBio-Degradable Plastics-Proposal For Green TechnologySudhakar PradhanNessuna valutazione finora
- Profile On KindergartenDocumento22 pagineProfile On KindergartenFikirie MogesNessuna valutazione finora
- Flood Risk Maps To Cultural Heritage Measures and Process - 2015 - Journal of Cultural Heritage PDFDocumento11 pagineFlood Risk Maps To Cultural Heritage Measures and Process - 2015 - Journal of Cultural Heritage PDFJosé BritesNessuna valutazione finora
- Corrugated Iron SheetDocumento28 pagineCorrugated Iron Sheetabebech arNessuna valutazione finora
- Briquette From Coffee Husk: Meharu KDocumento9 pagineBriquette From Coffee Husk: Meharu KMeharu100% (1)
- Fruits and VegitableDocumento18 pagineFruits and VegitableJemalNessuna valutazione finora
- Food Hygiene (PDFDrive)Documento122 pagineFood Hygiene (PDFDrive)GANIZANI MUMBANessuna valutazione finora
- Woven Label Feasibility StudyDocumento51 pagineWoven Label Feasibility StudySamwovenNessuna valutazione finora
- Ene Ato Eliyas PaperDocumento47 pagineEne Ato Eliyas PaperDegearege AndualemNessuna valutazione finora
- Seminar GDocumento22 pagineSeminar GMrku HyleNessuna valutazione finora
- AregaDocumento25 pagineAregaMelese FirdisaNessuna valutazione finora
- Coffee Supply Chain Planning Under Climate ChangeDocumento16 pagineCoffee Supply Chain Planning Under Climate Changerusman714Nessuna valutazione finora
- EAC Trade and Investment Report 2018 WEBDocumento520 pagineEAC Trade and Investment Report 2018 WEBShamone JNessuna valutazione finora
- Kindergarten Business Plan: 1. EXECUTIVE SUMMARY........................................................ 1Documento27 pagineKindergarten Business Plan: 1. EXECUTIVE SUMMARY........................................................ 1Tesfayé HailuNessuna valutazione finora
- Final BUSINESS PLAN FOR CONNS LIMITEDDocumento66 pagineFinal BUSINESS PLAN FOR CONNS LIMITEDOwunari Adaye-Orugbani100% (1)
- Ethiopia - Agro-ProcessingDocumento9 pagineEthiopia - Agro-ProcessingAfeworkNessuna valutazione finora
- Heavy Industries (Environmental Impact Assessment)Documento11 pagineHeavy Industries (Environmental Impact Assessment)RICAMAE DUBRIA100% (1)
- Business Plan For Benishangul Indigenious Handicraft Manufacturing EnterpriseDocumento17 pagineBusiness Plan For Benishangul Indigenious Handicraft Manufacturing Enterprisemadawe adem100% (2)
- The Great Savings and Loan Debacle PDFDocumento179 pagineThe Great Savings and Loan Debacle PDFhaginileNessuna valutazione finora
- Project Profile FinalDocumento183 pagineProject Profile Finalvenkateswaran.M venkateswaran.MNessuna valutazione finora
- Project Report On Dairy Farm: Shri. Taichat Biham (Pan-Ccspb0082R)Documento10 pagineProject Report On Dairy Farm: Shri. Taichat Biham (Pan-Ccspb0082R)CA Devangaraj GogoiNessuna valutazione finora
- The Impact of Ogbomoso Migrants On The Socio Political Development of Ogbomoso From 1969-2010Documento40 pagineThe Impact of Ogbomoso Migrants On The Socio Political Development of Ogbomoso From 1969-2010Oladipo EmmanuelNessuna valutazione finora
- Wheat Supply Chain Issues in EthiopiaDocumento24 pagineWheat Supply Chain Issues in EthiopiaAbbee TerefeNessuna valutazione finora
- Atoro ProposalDocumento38 pagineAtoro ProposalDessalegn GaminiNessuna valutazione finora
- Trade Report: Advancing Canada's Interests in Global MarketsDocumento64 pagineTrade Report: Advancing Canada's Interests in Global MarketsSiyabonga NyeziNessuna valutazione finora
- Tafesse YuaDocumento11 pagineTafesse Yuaalemayehu tarikuNessuna valutazione finora
- Emission Policy MalaysiaDocumento12 pagineEmission Policy Malaysiafaridmd84Nessuna valutazione finora
- SSG Agro: Dry Fish Market AssessmentDocumento26 pagineSSG Agro: Dry Fish Market AssessmentmasudNessuna valutazione finora
- 4 - 5796607318607006691 PDocumento33 pagine4 - 5796607318607006691 Pselome NegatuNessuna valutazione finora
- Boilers Making PLantDocumento26 pagineBoilers Making PLantEsayas Mekonnen100% (1)
- Electric Mobility For Sustainable TourismDocumento13 pagineElectric Mobility For Sustainable TourismВікторія ПоловкоNessuna valutazione finora
- Hawassa University Awada Business and Economics CollegeDocumento9 pagineHawassa University Awada Business and Economics CollegeAmir sabirNessuna valutazione finora
- Ojtbook Janine LatestDocumento80 pagineOjtbook Janine LatestJanine Grace LilanNessuna valutazione finora
- Milion - ProposalDocumento34 pagineMilion - Proposalzelalem adaneNessuna valutazione finora
- My Business PlanDocumento7 pagineMy Business Planadeoye sheyiNessuna valutazione finora
- Global Agro Distributors Goat Farming Business Plan 4/5/2023Documento44 pagineGlobal Agro Distributors Goat Farming Business Plan 4/5/2023Tafadzwa MvulaNessuna valutazione finora
- Jamie Oliver Restaurant ChainDocumento6 pagineJamie Oliver Restaurant Chaintran quoc vietNessuna valutazione finora
- ESMF IQ-P171446 Advance VersionDocumento131 pagineESMF IQ-P171446 Advance VersionsuhailNessuna valutazione finora
- Sea Pride LLCDocumento6 pagineSea Pride LLCakmohideenNessuna valutazione finora
- MANTO Industrial PLCDocumento55 pagineMANTO Industrial PLCTeshome AbebeNessuna valutazione finora
- Proposal On Spring WaterDocumento48 pagineProposal On Spring WaterTesfaye DegefaNessuna valutazione finora
- Baseline Survey Report On Seaweed Cultivation, Processing, and Marketing For Employment Generation in Bangladesh's Coastal Poor CommunitiesDocumento9 pagineBaseline Survey Report On Seaweed Cultivation, Processing, and Marketing For Employment Generation in Bangladesh's Coastal Poor CommunitiesInternational Journal of Innovative Science and Research TechnologyNessuna valutazione finora
- Proposed Indicators For Peace Corps Water, Sanitation, and Hygiene Education ProjectsDocumento3 pagineProposed Indicators For Peace Corps Water, Sanitation, and Hygiene Education ProjectsDar Al KhairNessuna valutazione finora
- DSGEDocumento10 pagineDSGEsimbiroNessuna valutazione finora
- PAMSpyDocumento13 paginePAMSpysimbiroNessuna valutazione finora
- Decision Making Through Simulation in Public Policy Management FieldDocumento10 pagineDecision Making Through Simulation in Public Policy Management FieldsimbiroNessuna valutazione finora
- Innovation4resilience - Guidelines For Applicants Component 1Documento10 pagineInnovation4resilience - Guidelines For Applicants Component 1simbiroNessuna valutazione finora
- GAMSReader April 2009Documento85 pagineGAMSReader April 2009simbiroNessuna valutazione finora
- Foreign Exchange Regulations and Directives in EthiopiaDocumento6 pagineForeign Exchange Regulations and Directives in EthiopiasimbiroNessuna valutazione finora
- Full PromulgationDocumento17 pagineFull PromulgationsimbiroNessuna valutazione finora
- Aaccsa Draft Part IIDocumento4 pagineAaccsa Draft Part IIsimbiroNessuna valutazione finora
- National Bank of Ethiopia (NBE) Directive Amendments On Foreign Exchange (2016/2017)Documento3 pagineNational Bank of Ethiopia (NBE) Directive Amendments On Foreign Exchange (2016/2017)simbiroNessuna valutazione finora
- Innovation4resilience - Concept Note Template Component 1Documento4 pagineInnovation4resilience - Concept Note Template Component 1simbiroNessuna valutazione finora
- Unicef TechnicalDocumento7 pagineUnicef TechnicalsimbiroNessuna valutazione finora
- Fat FileDocumento2 pagineFat FilesimbiroNessuna valutazione finora
- Fund For Local Cooperation (FLC) : Application FormDocumento9 pagineFund For Local Cooperation (FLC) : Application FormsimbiroNessuna valutazione finora
- WGF SAIP Self AssessmentDocumento8 pagineWGF SAIP Self AssessmentsimbiroNessuna valutazione finora
- Grand Challenges Explorations Application Form: Section I. What Is Your Idea?Documento1 paginaGrand Challenges Explorations Application Form: Section I. What Is Your Idea?simbiroNessuna valutazione finora
- Aaccsa FinalDocumento29 pagineAaccsa FinalsimbiroNessuna valutazione finora
- Panafrican ConsDocumento5 paginePanafrican ConssimbiroNessuna valutazione finora
- Extract SixDocumento50 pagineExtract Sixsimbiro100% (1)
- Ministry of EnvironmentDocumento14 pagineMinistry of EnvironmentsimbiroNessuna valutazione finora
- Hossana NoteDocumento2 pagineHossana NotesimbiroNessuna valutazione finora
- Introduction and BackgroundDocumento2 pagineIntroduction and BackgroundsimbiroNessuna valutazione finora
- Invitation For Consultancy Service To Produce Training Manual, Field Guide and Provide TOT On Selected DFSA Crop Value Chain CommoditiesDocumento5 pagineInvitation For Consultancy Service To Produce Training Manual, Field Guide and Provide TOT On Selected DFSA Crop Value Chain CommoditiessimbiroNessuna valutazione finora
- Technical Proposal To Produce Training Manual, Field Guide and Provide TOT On Selected DFSA Crop Value Chain CommoditiesDocumento7 pagineTechnical Proposal To Produce Training Manual, Field Guide and Provide TOT On Selected DFSA Crop Value Chain CommoditiessimbiroNessuna valutazione finora
- Methods For ConsiderationsDocumento10 pagineMethods For ConsiderationssimbiroNessuna valutazione finora
- February 2019 Addis Ababa: Project BackgroundDocumento8 pagineFebruary 2019 Addis Ababa: Project BackgroundsimbiroNessuna valutazione finora
- Experience and StaffDocumento2 pagineExperience and StaffsimbiroNessuna valutazione finora
- Unicef TechnicalDocumento7 pagineUnicef TechnicalsimbiroNessuna valutazione finora
- Fallow OnDocumento6 pagineFallow OnsimbiroNessuna valutazione finora
- Feyera CVDocumento8 pagineFeyera CVsimbiroNessuna valutazione finora
- Adane Produced PropDocumento12 pagineAdane Produced PropsimbiroNessuna valutazione finora
- M C M C M C: Unit 11 Let's Hear ! Unit 13 Zure Is Sick Unit 12 My Best Friend Claire Unit 14 The Mermaid's TailDocumento16 pagineM C M C M C: Unit 11 Let's Hear ! Unit 13 Zure Is Sick Unit 12 My Best Friend Claire Unit 14 The Mermaid's TailNurHamizahNessuna valutazione finora
- Sohrabudin Encounter CaseDocumento9 pagineSohrabudin Encounter CaseNDTVNessuna valutazione finora
- A Situational and Strategic Analysis of Ikea and The Future (Circulated Copy)Documento31 pagineA Situational and Strategic Analysis of Ikea and The Future (Circulated Copy)chandro2007100% (1)
- Professional Profile:: Dr. C.V. Ananda BoseDocumento7 pagineProfessional Profile:: Dr. C.V. Ananda BoseGokul KrishnanNessuna valutazione finora
- More About MeDocumento3 pagineMore About Meapi-459464616Nessuna valutazione finora
- Peoples Aircargo v. CADocumento2 paginePeoples Aircargo v. CAVince MontealtoNessuna valutazione finora
- Public Private Initiatives in Hydropower Projects in Nepal-Opportunities and ChallangesDocumento61 paginePublic Private Initiatives in Hydropower Projects in Nepal-Opportunities and ChallangesNef Urja ChautariNessuna valutazione finora
- Overview of Electronic Signature Law in The EUDocumento3 pagineOverview of Electronic Signature Law in The EUHamed RokniNessuna valutazione finora
- The Frontier Post 25 Dec 2023Documento13 pagineThe Frontier Post 25 Dec 2023Muhammad WaseemNessuna valutazione finora
- Challenges To Democracy in Pakistan EssayDocumento2 pagineChallenges To Democracy in Pakistan EssayZubair Burki50% (2)
- E-Government and ManagerialismDocumento19 pagineE-Government and ManagerialismLucilaNessuna valutazione finora
- Newslore Contemporary Folklore OnDocumento279 pagineNewslore Contemporary Folklore OnpanosNessuna valutazione finora
- Story of Noynoy AquinoDocumento2 pagineStory of Noynoy AquinoRENGIE GALONessuna valutazione finora
- Climate VariabilityDocumento4 pagineClimate VariabilityFaiz M TaimurNessuna valutazione finora
- Literatur Review: Bentuk - Bentuk Cyberbullying Pada Anak SMADocumento12 pagineLiteratur Review: Bentuk - Bentuk Cyberbullying Pada Anak SMAAninta IngelyaNessuna valutazione finora
- Santhal UprisingDocumento4 pagineSanthal UprisingAmit KumarNessuna valutazione finora
- Español vs. Toledo-Mupas (Digest)Documento2 pagineEspañol vs. Toledo-Mupas (Digest)Tini GuanioNessuna valutazione finora
- დემოკრატიული სახელმწიფო & კანონის მნიშვნელობაDocumento12 pagineდემოკრატიული სახელმწიფო & კანონის მნიშვნელობაScmopocNessuna valutazione finora
- Associate Com. Vs DumlaoDocumento7 pagineAssociate Com. Vs DumlaoJuvy Ann IringanNessuna valutazione finora
- 1892 Merrill Law of MandamusDocumento554 pagine1892 Merrill Law of MandamusEdward kabunduNessuna valutazione finora
- 28 San Roque Realty Vs Republic DigestDocumento3 pagine28 San Roque Realty Vs Republic Digestjimart10Nessuna valutazione finora
- Falklands Wars - The History of The Falk PDFDocumento124 pagineFalklands Wars - The History of The Falk PDFanascopelNessuna valutazione finora
- Project Proposal: School: Sta. Justina National High School Municipality: Buhi Congressional District: 5thDocumento3 pagineProject Proposal: School: Sta. Justina National High School Municipality: Buhi Congressional District: 5thMary Jean C. BorjaNessuna valutazione finora
- The Judiciary - ReviewerDocumento16 pagineThe Judiciary - ReviewerKarlo KapunanNessuna valutazione finora
- Sojourner Truth Ain't I A Woman (U.S. National Park Service)Documento5 pagineSojourner Truth Ain't I A Woman (U.S. National Park Service)Brianna ReyesNessuna valutazione finora
- Gender and Society 1Documento79 pagineGender and Society 1J Pao Bayro LacanilaoNessuna valutazione finora
- ICESCRDocumento10 pagineICESCRTaaNessuna valutazione finora
- Prof. Vlado Šakić - Rat U BiH 1991. - 1995.Documento241 pagineProf. Vlado Šakić - Rat U BiH 1991. - 1995.Bistrica87Nessuna valutazione finora
- Executive Secretary vs. Southwing Heavy Industries, Inc., 482 SCRA 673, G.R. No. 164171, G.R. No. 164172, G.R. No. 168741 February 20, 2006Documento52 pagineExecutive Secretary vs. Southwing Heavy Industries, Inc., 482 SCRA 673, G.R. No. 164171, G.R. No. 164172, G.R. No. 168741 February 20, 2006Lester AgoncilloNessuna valutazione finora
- Speech Susan B Anthony 2Documento1 paginaSpeech Susan B Anthony 2kathleen_faasNessuna valutazione finora