Potrebbero piacerti anche
- Extra SpecForce Blue Jeans Butt SolutionDocumento9 pagineExtra SpecForce Blue Jeans Butt SolutionGilberto Solares100% (2)
- Target BodybuildingDocumento285 pagineTarget Bodybuildingdlsppp88% (8)
- Chiro HIODocumento18 pagineChiro HIOPierre SERPAGGINessuna valutazione finora
- Exercise Guide From Reader's DigestDocumento14 pagineExercise Guide From Reader's DigestAkoyaMNessuna valutazione finora
- Horizontal Alveolar Ridge Augmentation in Implant Dentistry: A Surgical ManualDa EverandHorizontal Alveolar Ridge Augmentation in Implant Dentistry: A Surgical ManualValutazione: 4.5 su 5 stelle4.5/5 (2)
- Joint Freeing Series PDFDocumento2 pagineJoint Freeing Series PDFDavid Goodwin100% (2)
- Top 5 Strength Exercises For RugbyDocumento4 pagineTop 5 Strength Exercises For RugbyPaul Tinashe KatuliibaNessuna valutazione finora
- CH 5 AnswersDocumento22 pagineCH 5 AnswersYhormmie Harjeinifujah100% (2)
- BBB Month 31 Workout PlanDocumento11 pagineBBB Month 31 Workout PlanluniblueNessuna valutazione finora
- Recent Advances in The Rehabilitation LCADocumento19 pagineRecent Advances in The Rehabilitation LCAMiguel Andres Sepulveda CastroNessuna valutazione finora
- 2016 The American Society of Shoulder and ElbowDocumento15 pagine2016 The American Society of Shoulder and ElbowDiego De Farias Diehl100% (1)
- 2016 The American Society of Shoulder and ElbowDocumento15 pagine2016 The American Society of Shoulder and ElbowDiego De Farias Diehl100% (1)
- Rehabilitacion LCADocumento44 pagineRehabilitacion LCAsebafigueroa94Nessuna valutazione finora
- The Bench Press PDFDocumento10 pagineThe Bench Press PDFMarco TorreNessuna valutazione finora
- Training Programme 2 WeeksDocumento20 pagineTraining Programme 2 Weeksbrotherbeyond1975Nessuna valutazione finora
- Su Jok and Moxa, A Self-Treatment Manual (PDFDrive) ExportDocumento7 pagineSu Jok and Moxa, A Self-Treatment Manual (PDFDrive) ExportJorin JorinNessuna valutazione finora
- Avances LCA WilkDocumento19 pagineAvances LCA WilkCarlos Martín De RosasNessuna valutazione finora
- PSR Module 2 - Web CourseDocumento101 paginePSR Module 2 - Web CourseAndrei R LupuNessuna valutazione finora
- 1 s2.0 S0030589819300811 MainDocumento8 pagine1 s2.0 S0030589819300811 MainAna Carolina SouzaNessuna valutazione finora
- Anterior Cruciate Ligament Reconstruction Rehabilitation: MOON GuidelinesDocumento5 pagineAnterior Cruciate Ligament Reconstruction Rehabilitation: MOON GuidelinesSilvy OktavianaNessuna valutazione finora
- Ijcem 0025116Documento11 pagineIjcem 0025116Eurovision RSNessuna valutazione finora
- Role of Physiotherapy in Repair ACLDocumento4 pagineRole of Physiotherapy in Repair ACLSri WidiatmiNessuna valutazione finora
- Post-Operative Criterion Based Rehabilitation of Acl Repairs: A Clinical CommentaryDocumento13 paginePost-Operative Criterion Based Rehabilitation of Acl Repairs: A Clinical CommentaryDeep ShreeNessuna valutazione finora
- Rehabilitation Program: Physical TherapyDocumento3 pagineRehabilitation Program: Physical TherapyEffendi UChinNessuna valutazione finora
- Return-to-Sport Testing After Medial Patellofemoral Ligament Reconstruction in Adolescent AthletesDocumento7 pagineReturn-to-Sport Testing After Medial Patellofemoral Ligament Reconstruction in Adolescent AthletesiwanNessuna valutazione finora
- Post-Operative Criterion Based Rehabilitation of Acl Repairs: A Clinical CommentaryDocumento14 paginePost-Operative Criterion Based Rehabilitation of Acl Repairs: A Clinical CommentaryferryNessuna valutazione finora
- Ebok Progam Acl2018Documento31 pagineEbok Progam Acl2018Tantia Dewi HariantoNessuna valutazione finora
- Bodkin - Time Between RTP Assessments To Achieve Strength Gains post-ACLR - 2019Documento8 pagineBodkin - Time Between RTP Assessments To Achieve Strength Gains post-ACLR - 2019krayfieldNessuna valutazione finora
- Artros Cadera Programa de EjercDocumento11 pagineArtros Cadera Programa de EjercgeorginaNessuna valutazione finora
- Hop Testing Provides A Reliable and Valid Outcome Measure During Rehabilitation After Anterior Cruciate Ligament Reconstruction PDFDocumento13 pagineHop Testing Provides A Reliable and Valid Outcome Measure During Rehabilitation After Anterior Cruciate Ligament Reconstruction PDFCleber PimentaNessuna valutazione finora
- Rehabilitation For Hip Arthros PDFDocumento4 pagineRehabilitation For Hip Arthros PDFMónica Sabogal JaramilloNessuna valutazione finora
- NIH Public AccessDocumento33 pagineNIH Public AccessAulida Arum MNessuna valutazione finora
- SH 1Documento10 pagineSH 1ع الNessuna valutazione finora
- Final Annotated Bib - Unhappy TriadDocumento21 pagineFinal Annotated Bib - Unhappy Triadapi-458073428Nessuna valutazione finora
- Rehabilitationafter Arthroscopic Decompressionfor Femoroacetabular ImpingementDocumento9 pagineRehabilitationafter Arthroscopic Decompressionfor Femoroacetabular ImpingementEricNessuna valutazione finora
- J CSM 2019 08 004Documento19 pagineJ CSM 2019 08 004Windu Airlangga EkacarakaNessuna valutazione finora
- Quadriceps Muscle Function After Rehabilitation With Cryotherapy in Patients With Anterior Cruciate Ligament ReconstructionDocumento7 pagineQuadriceps Muscle Function After Rehabilitation With Cryotherapy in Patients With Anterior Cruciate Ligament ReconstructionMarco Antonio Silva RiveraNessuna valutazione finora
- A Ten Task-Based Progression in Rehabilitation After Acl Reconstruction: From Post-Surgery To Return To Play - A Clinical CommentaryDocumento13 pagineA Ten Task-Based Progression in Rehabilitation After Acl Reconstruction: From Post-Surgery To Return To Play - A Clinical CommentaryyahoomenNessuna valutazione finora
- Chest Expander Spring A Low Cost Home Physiotherapybased Exercise Rehabilitation After Total Hip ArthroplastyDocumento11 pagineChest Expander Spring A Low Cost Home Physiotherapybased Exercise Rehabilitation After Total Hip ArthroplastyAmar DahmaniNessuna valutazione finora
- Recommendations For Plyometric Training After ACL Reconstruction - A Clinical CommentaryDocumento17 pagineRecommendations For Plyometric Training After ACL Reconstruction - A Clinical CommentarymeNessuna valutazione finora
- GR Up: SM Orthopedics & Muscular SystemDocumento6 pagineGR Up: SM Orthopedics & Muscular SystemValerie BpNessuna valutazione finora
- The Long-Term Effect of 2 PostoperativeDocumento9 pagineThe Long-Term Effect of 2 Postoperativeahmed K.Abd el SaterNessuna valutazione finora
- Commented (E1) : Include An Abstract in Your Final PaperDocumento8 pagineCommented (E1) : Include An Abstract in Your Final PaperAnonymous AY6XDZHBxPNessuna valutazione finora
- C Rioter ApyDocumento6 pagineC Rioter ApyDanNy ClaudiuNessuna valutazione finora
- Art - Equilibrio y PropiocepcionDocumento7 pagineArt - Equilibrio y PropiocepcionYuLyChNessuna valutazione finora
- Total Shoulder Arthroplasty GuidelineDocumento17 pagineTotal Shoulder Arthroplasty GuidelineMaria Luísa MirandaNessuna valutazione finora
- Rehabilitation and Return To Sports After Acl ReconstructionDocumento5 pagineRehabilitation and Return To Sports After Acl ReconstructionjasonoytumandukNessuna valutazione finora
- Effects of Running Retraining After Knee Anterior Cruciate Ligament ReconstructionDocumento12 pagineEffects of Running Retraining After Knee Anterior Cruciate Ligament Reconstructionguillaume BartheNessuna valutazione finora
- Exercise-Based ApproachDocumento4 pagineExercise-Based Approachfederico BiettiNessuna valutazione finora
- Brinlee Et Al ACL Guidelines Paper - SportsHealth - 2021Documento10 pagineBrinlee Et Al ACL Guidelines Paper - SportsHealth - 2021Antoine ClyNessuna valutazione finora
- 0269215511423557Documento10 pagine0269215511423557Jose Maria DominguezNessuna valutazione finora
- ACL BrotzmanDocumento7 pagineACL Brotzmankhushboopakhrani98Nessuna valutazione finora
- Treatment, Return To Play, and Performance Following Meniscus Surgery (Hanna 2022) FisioDocumento13 pagineTreatment, Return To Play, and Performance Following Meniscus Surgery (Hanna 2022) Fisiog.paffettiNessuna valutazione finora
- 10 1155@2019@1694695Documento8 pagine10 1155@2019@1694695DATO13Nessuna valutazione finora
- 1 s2.0 S0020138313005718 MainDocumento7 pagine1 s2.0 S0020138313005718 MainMutiara Rachmawati ViorhaNessuna valutazione finora
- Lca PDFDocumento6 pagineLca PDFPedro CespedesNessuna valutazione finora
- Effects On Lower Extremity Neuromuscular Control Exercises On Knee PDFDocumento7 pagineEffects On Lower Extremity Neuromuscular Control Exercises On Knee PDFEva MartinezNessuna valutazione finora
- Denis Et AlDocumento12 pagineDenis Et AlSruthi Nair HeblikarNessuna valutazione finora
- Postertemplate 36 X 24Documento1 paginaPostertemplate 36 X 24api-300747065Nessuna valutazione finora
- The Timing of Rehabilitation Commencement After Reconstruction of The Anterior Cruciate LigamentDocumento5 pagineThe Timing of Rehabilitation Commencement After Reconstruction of The Anterior Cruciate LigamentQuiroprácticaParaTodosNessuna valutazione finora
- Herrington 2004Documento4 pagineHerrington 2004Francisco Javier Medina CaballeroNessuna valutazione finora
- Penanganan Cedera Olahraga Pada Sendi Lutut DR Maria Eva Dana SPKFR PDFDocumento32 paginePenanganan Cedera Olahraga Pada Sendi Lutut DR Maria Eva Dana SPKFR PDFAmuba MaNessuna valutazione finora
- Esska Knee Munich Doc 18Documento16 pagineEsska Knee Munich Doc 18Avram GeorgievNessuna valutazione finora
- The Knee: Sean F. Scanlan, Joseph P. Donahue, Thomas P. AndriacchiDocumento6 pagineThe Knee: Sean F. Scanlan, Joseph P. Donahue, Thomas P. Andriacchihectorlekepi92Nessuna valutazione finora
- The New in Sport Medicine 2011Documento10 pagineThe New in Sport Medicine 2011Daniel G. A. C.Nessuna valutazione finora
- Ok An 2008Documento4 pagineOk An 2008Adrián García RamírezNessuna valutazione finora
- Guidelines Rotator Cuff InjuryDocumento5 pagineGuidelines Rotator Cuff InjuryAlberto GrpNessuna valutazione finora
- Colgan 2016Documento6 pagineColgan 2016Wahyu InsanNessuna valutazione finora
- Kell 2009Documento10 pagineKell 2009Luis MiguelNessuna valutazione finora
- Return Sport Post Atroskopi SholdrDocumento8 pagineReturn Sport Post Atroskopi SholdrFarhan JustisiaNessuna valutazione finora
- Acl N PilatesDocumento8 pagineAcl N PilatesDeva JCNessuna valutazione finora
- JSR Article p335Documento11 pagineJSR Article p335MarianoNessuna valutazione finora
- Engrossed ?? (Polished) My Theoretical Skills in Anatomy, Physiology and Biochemistry. in TheDocumento2 pagineEngrossed ?? (Polished) My Theoretical Skills in Anatomy, Physiology and Biochemistry. in ThealdaNessuna valutazione finora
- Engrossed ?? (Polished) My Theoretical Skills in Anatomy, Physiology and Biochemistry. in TheDocumento2 pagineEngrossed ?? (Polished) My Theoretical Skills in Anatomy, Physiology and Biochemistry. in ThealdaNessuna valutazione finora
- Rundown Alumni GatheringDocumento1 paginaRundown Alumni GatheringaldaNessuna valutazione finora
- Three Cases of Chronic Suppurative Otitis Media (CSOM) Caused by Kerstersia Gyiorum and A Review of The LiteratureDocumento6 pagineThree Cases of Chronic Suppurative Otitis Media (CSOM) Caused by Kerstersia Gyiorum and A Review of The LiteraturealdaNessuna valutazione finora
- Stetoskop PresentDocumento34 pagineStetoskop PresentSam 6928Nessuna valutazione finora
- Application Form: Cimsa National OfficialsDocumento2 pagineApplication Form: Cimsa National OfficialsaldaNessuna valutazione finora
- My Creative CVDocumento31 pagineMy Creative CVsumiyatiNessuna valutazione finora
- 1 s2.0 S1743919115002381 MainDocumento8 pagine1 s2.0 S1743919115002381 MainaldaNessuna valutazione finora
- Tugas Mikrobiologiku Mendekati SeleseDocumento5 pagineTugas Mikrobiologiku Mendekati SelesealdaNessuna valutazione finora
- 1Documento1 pagina1aldaNessuna valutazione finora
- Tugas Mikrobiologiku Mendekati SeleseDocumento5 pagineTugas Mikrobiologiku Mendekati SelesealdaNessuna valutazione finora
- Tugas Mikrobiologiku Mendekati SeleseDocumento5 pagineTugas Mikrobiologiku Mendekati SelesealdaNessuna valutazione finora
- Daftar Nama Anatomi Inggris-LatinDocumento58 pagineDaftar Nama Anatomi Inggris-LatinFelicia NikeNessuna valutazione finora
- Examen FisicoDocumento26 pagineExamen FisicoAmada Angel VillanuevaNessuna valutazione finora
- Beighton Hypermobility ScoreDocumento6 pagineBeighton Hypermobility ScoreluckyNessuna valutazione finora
- LECTURA 2. Developmental KinesiologyDocumento11 pagineLECTURA 2. Developmental KinesiologysaraNessuna valutazione finora
- Into To Kine & Anatomical Position New 2023Documento26 pagineInto To Kine & Anatomical Position New 2023Harshveer ThindNessuna valutazione finora
- Chapter 5 The Skeletal SystemDocumento47 pagineChapter 5 The Skeletal SystemOlalekan OyekunleNessuna valutazione finora
- Penatalaksanaan Fisioterapi Pada Kasus Low: Back Pain (LBP) Akibat Spondylosis DenganDocumento12 paginePenatalaksanaan Fisioterapi Pada Kasus Low: Back Pain (LBP) Akibat Spondylosis Denganhafshoh lylaNessuna valutazione finora
- Ulnar Tunnel Syndrome - Hand - OrthobulletsDocumento7 pagineUlnar Tunnel Syndrome - Hand - OrthobulletsSylvia GraceNessuna valutazione finora
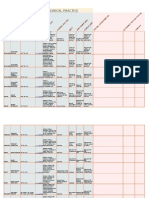
- Goniometry For Clinical PracticeDocumento7 pagineGoniometry For Clinical Practicedramitsaini33% (3)
- Articles by Dr. Nata ParnesDocumento19 pagineArticles by Dr. Nata ParnesWatertown Daily TimesNessuna valutazione finora
- Skin TractionDocumento14 pagineSkin TractionAnis IzzatiNessuna valutazione finora
- GRAVES EDITED IE 1 FinalDocumento11 pagineGRAVES EDITED IE 1 FinalasdNessuna valutazione finora
- ABDOMEN: Posterior Abdominal Region IDocumento19 pagineABDOMEN: Posterior Abdominal Region IElijah JeusNessuna valutazione finora
- IASTM - jOURNALDocumento12 pagineIASTM - jOURNALviorelNessuna valutazione finora
- Correction of Severe Crouch Gait in Patients With Spastic Diplegia With Use of Multilevel Orthopaedic SurgeryDocumento12 pagineCorrection of Severe Crouch Gait in Patients With Spastic Diplegia With Use of Multilevel Orthopaedic Surgeryyarimar hoyosNessuna valutazione finora
- PersistdeloadDocumento11 paginePersistdeloadPaulo Ariza AguasNessuna valutazione finora
- 3.1 Human Osteology HandoutDocumento3 pagine3.1 Human Osteology Handoutgriselpaulino100% (1)
- U10-Distal Radius FracturesDocumento121 pagineU10-Distal Radius Fracturesrajasekhar ANessuna valutazione finora