Potrebbero piacerti anche
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (399)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- Dka ChartDocumento2 pagineDka Chartعمر احمد شاكرNessuna valutazione finora
- KadDocumento28 pagineKadhardiff12Nessuna valutazione finora
- DH VSCC Intern Manual 4th Edition - WEB PDFDocumento124 pagineDH VSCC Intern Manual 4th Edition - WEB PDFXyzNessuna valutazione finora
- Dka GuidelineDocumento16 pagineDka GuidelineGhada HusseinNessuna valutazione finora
- Nursing Care of Client With Endocrine DisorderDocumento93 pagineNursing Care of Client With Endocrine DisorderApril_Anne_Vel_343Nessuna valutazione finora
- Medical-Surgical Nursing Final Flashcards - QuizletDocumento22 pagineMedical-Surgical Nursing Final Flashcards - QuizletNursyNurseNessuna valutazione finora
- Endocrine Problems of The Adult ClientDocumento18 pagineEndocrine Problems of The Adult ClientMarylle AntonioNessuna valutazione finora
- Pimp QuestionsDocumento4 paginePimp QuestionsAmy Suzanne Bains0% (1)
- Diabetic Foot - Case PresentationDocumento54 pagineDiabetic Foot - Case PresentationMarlon Abad86% (7)
- ABG QuizDocumento12 pagineABG QuizParsaant SinghNessuna valutazione finora
- Pathophysiology of Carbohydrates MetabolismDocumento54 paginePathophysiology of Carbohydrates MetabolismMaui TingNessuna valutazione finora
- (OPTIMA) Pembahasan CBT To 2 Agustus 2020Documento1.906 pagine(OPTIMA) Pembahasan CBT To 2 Agustus 2020Rachel MadaiNessuna valutazione finora
- ABG's Clinical ScenariosDocumento18 pagineABG's Clinical ScenariosMuhammad Danish Hanif100% (1)
- Practice Test 1Documento10 paginePractice Test 1Riin IrasustaNessuna valutazione finora
- Ms Exam 500 Items - Answers With RatioDocumento61 pagineMs Exam 500 Items - Answers With RatioPrincessDiane'LouiseBautistaMartinNessuna valutazione finora
- Hyperglycaemic Emergencies Inpatient Draft-1-3Documento13 pagineHyperglycaemic Emergencies Inpatient Draft-1-3Cik JaaNessuna valutazione finora
- Quizlet EndoDocumento17 pagineQuizlet EndoemmaNessuna valutazione finora
- Paediatric DKA Integrated Care Pathway For CportalDocumento39 paginePaediatric DKA Integrated Care Pathway For Cportalteresita vargasNessuna valutazione finora
- Diabetic Ketoacidosis (DKA) VS. Hyperosmolar Hyperglycemic Syndrome (HHS)Documento5 pagineDiabetic Ketoacidosis (DKA) VS. Hyperosmolar Hyperglycemic Syndrome (HHS)MrRightNessuna valutazione finora
- Tacrolimus-Associated Diabetic Ketoacidosis A CaseDocumento6 pagineTacrolimus-Associated Diabetic Ketoacidosis A CaseSarah Gita SinagaNessuna valutazione finora
- Referral Letter To Specialist From GPDocumento74 pagineReferral Letter To Specialist From GPyazz80% (5)
- Unit 5 Part 2 InsulinDocumento68 pagineUnit 5 Part 2 InsulinKhairunnisa Loqman100% (1)
- Reviewer C AnswersDocumento39 pagineReviewer C AnswersDavis WhiteNessuna valutazione finora
- Chapter 17 - Diabetes Mellitus: The Two Key TasksDocumento20 pagineChapter 17 - Diabetes Mellitus: The Two Key Tasksprofarmah6150Nessuna valutazione finora
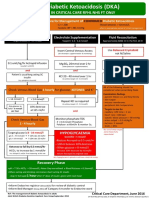
- Adult Diabetic Ketoacidosis (DKA) : For Use in Critical Care RFHL Nhs FT OnlyDocumento1 paginaAdult Diabetic Ketoacidosis (DKA) : For Use in Critical Care RFHL Nhs FT OnlyJung Bahadur SinghNessuna valutazione finora
- Diabetic Ketoacidosis Case StudyDocumento5 pagineDiabetic Ketoacidosis Case Studyjc_albano29100% (7)
- Case 3 Care of Client With GI, PUD, Cancer, Liver FailureDocumento33 pagineCase 3 Care of Client With GI, PUD, Cancer, Liver FailureNyeam NyeamNessuna valutazione finora
- PulmCrit - Four DKA PearlsDocumento12 paginePulmCrit - Four DKA PearlsStacey WoodsNessuna valutazione finora
- Ramadan and DiabetesDocumento14 pagineRamadan and DiabetesDitoLinggoNessuna valutazione finora
- DKA (Diabetic Ketoacidosis)Documento3 pagineDKA (Diabetic Ketoacidosis)Hassan.shehri83% (6)