Potrebbero piacerti anche
- Nectural EnuresisDocumento47 pagineNectural EnuresisalhassanmohamedNessuna valutazione finora
- Across The Red Line: Stories From The Surgical LifeDa EverandAcross The Red Line: Stories From The Surgical LifeValutazione: 2.5 su 5 stelle2.5/5 (2)
- The Kidney: Quicktime™ and A Tiff (Uncompressed) Decompressor Are Needed To See This PictureDocumento36 pagineThe Kidney: Quicktime™ and A Tiff (Uncompressed) Decompressor Are Needed To See This PictureSohaire Imtiaz100% (1)
- Karl Stroz Urology CatalogueDocumento388 pagineKarl Stroz Urology CatalogueSalam KamilNessuna valutazione finora
- Anatomy ShortcutDocumento73 pagineAnatomy ShortcutHARSHNessuna valutazione finora
- Anatomy QBank EMRCSDocumento117 pagineAnatomy QBank EMRCSTowhid HasanNessuna valutazione finora
- Approach To ShockDocumento19 pagineApproach To Shocksarath100% (1)
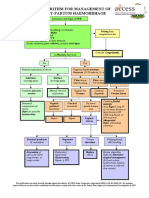
- 15 NG - PPH Algorithm-Aug08Documento2 pagine15 NG - PPH Algorithm-Aug08abdelhamed aliNessuna valutazione finora
- Hiv in Pregnancy FinalDocumento22 pagineHiv in Pregnancy FinalMoin PandithNessuna valutazione finora
- (Anterior Lobe) (Posterior Lobe) : FocusDocumento8 pagine(Anterior Lobe) (Posterior Lobe) : FocusVicviclookThekingNessuna valutazione finora
- Dr. Osama Mahmoud (Endocrinology)Documento253 pagineDr. Osama Mahmoud (Endocrinology)Mohammad Abd-AlhafezNessuna valutazione finora
- 2018 Edition of The European Association of Urology (EAU) GuidelinesDocumento415 pagine2018 Edition of The European Association of Urology (EAU) Guidelinessiraj hadi93% (15)
- Abdominal: Al HerniaDocumento3 pagineAbdominal: Al HerniaVon Hippo100% (1)
- Multidisciplinary Management of Prostate CancerDocumento158 pagineMultidisciplinary Management of Prostate CancersuckafuckNessuna valutazione finora
- Obituary From ANZCADocumento1 paginaObituary From ANZCAPippa NewsteadNessuna valutazione finora
- Fogsi ChecklistDocumento131 pagineFogsi ChecklistParimi VinodNessuna valutazione finora
- 2017 BMA Medical Book AwardsDocumento45 pagine2017 BMA Medical Book AwardsFerdinand Sta Ana Jr.Nessuna valutazione finora
- Plastic Surgery Training in SaudiDocumento22 paginePlastic Surgery Training in SaudiAnonymous 8hVpaQdCtrNessuna valutazione finora
- UROLOGY Surgical Pathology & X-RaysDocumento107 pagineUROLOGY Surgical Pathology & X-RaysKay BristolNessuna valutazione finora
- TourniquetDocumento17 pagineTourniquetkapilmalik2007Nessuna valutazione finora
- O&G CompendiumDocumento676 pagineO&G Compendiumwalefamous100% (1)
- Clinical Review - Full PDFDocumento6 pagineClinical Review - Full PDFDewi WulansariNessuna valutazione finora
- Revised Rate List of Hospital Charges, AIIMS, New Delhi, India PDFDocumento30 pagineRevised Rate List of Hospital Charges, AIIMS, New Delhi, India PDFInder67% (3)
- Artery-First Approaches To Pancreatoduodenectomy BJS 2011Documento9 pagineArtery-First Approaches To Pancreatoduodenectomy BJS 2011Roberto Hernandez100% (1)
- General Surgery Logbook Survey - Royal College of Surgeons of England - BulletinDocumento6 pagineGeneral Surgery Logbook Survey - Royal College of Surgeons of England - BulletinEd FitzgeraldNessuna valutazione finora
- 22 Shock Classifi Cation, Pathophysiology, and Approach To Management PDFDocumento44 pagine22 Shock Classifi Cation, Pathophysiology, and Approach To Management PDFismi latifahNessuna valutazione finora
- By C. Michael Samson, M.D.: Ocular TuberculosisDocumento7 pagineBy C. Michael Samson, M.D.: Ocular TuberculosisgigibesiNessuna valutazione finora
- Med PolicyDocumento191 pagineMed PolicyManoj Raghav100% (1)
- Medanta List Rate Card 2018Documento169 pagineMedanta List Rate Card 2018Udayan AwasthiNessuna valutazione finora
- IDSA-ATS - Consensus Guidelines On The Management of CAP in AdultsDocumento46 pagineIDSA-ATS - Consensus Guidelines On The Management of CAP in AdultscharliedelNessuna valutazione finora
- Introducing Fundamentals of Endoscopic Surgery (FES) From SAGESDocumento1 paginaIntroducing Fundamentals of Endoscopic Surgery (FES) From SAGESEndoscopicSurgeryNessuna valutazione finora
- Physiology of Erection and EjaculationDocumento1 paginaPhysiology of Erection and EjaculationricohutabaratNessuna valutazione finora
- Viva Practice The FRCS (Urol) and Postgraduate Urology Examinations 2018Documento79 pagineViva Practice The FRCS (Urol) and Postgraduate Urology Examinations 2018Sufi KhanNessuna valutazione finora
- Principles of Bariatric and Metabolic SurgeryDocumento51 paginePrinciples of Bariatric and Metabolic SurgeryDr Shahzad Alam ShahNessuna valutazione finora
- Reproductive EndocrinologyDocumento18 pagineReproductive EndocrinologyAnonymous hkWIKjoXFVNessuna valutazione finora
- Pass Critical Care Endocrine Frcem ResourcesDocumento41 paginePass Critical Care Endocrine Frcem ResourcesYoussef SaadNessuna valutazione finora
- CGHS Bengaluru Rates List As On NOv.2014Documento53 pagineCGHS Bengaluru Rates List As On NOv.2014mamuhydNessuna valutazione finora
- KASP Package RateDocumento502 pagineKASP Package RateAnoop VijayakumarNessuna valutazione finora
- North East London Mangement of Infection GuideDocumento52 pagineNorth East London Mangement of Infection GuideEGirayGuvenNessuna valutazione finora
- MDH Dissertations 2016 2019Documento10 pagineMDH Dissertations 2016 2019Masuri VarshaNessuna valutazione finora
- Jmir V14i3e85 App1Documento4 pagineJmir V14i3e85 App1joselyn sandovalNessuna valutazione finora
- Sanofi 2017 JPM PresentationDocumento24 pagineSanofi 2017 JPM PresentationmedtechyNessuna valutazione finora
- NTD Stag Report 2011Documento10 pagineNTD Stag Report 2011pmonesNessuna valutazione finora
- Global Tuberculosis Control 2008Documento304 pagineGlobal Tuberculosis Control 2008herylinotNessuna valutazione finora
- ECCO GuidelinesDocumento2 pagineECCO GuidelinesaljNessuna valutazione finora
- Mehu131 - U1 - T4 - Corticoesteroides en Meningitis TuberculosaDocumento3 pagineMehu131 - U1 - T4 - Corticoesteroides en Meningitis TuberculosalizdanNessuna valutazione finora
- Ageing of Hazardous InstallationsDocumento34 pagineAgeing of Hazardous InstallationsnmosilvaNessuna valutazione finora
- Env JM Mono (2020) 4.enDocumento77 pagineEnv JM Mono (2020) 4.endamien.ngo.beNessuna valutazione finora
- Guidlane TB 2020Documento42 pagineGuidlane TB 2020Marfu'ah Mar'ahNessuna valutazione finora
- OecdDocumento32 pagineOecdVivek SagayarajNessuna valutazione finora
- The Selection and Use of Essential MedicinesDocumento604 pagineThe Selection and Use of Essential MedicinesStephanie GarciaNessuna valutazione finora
- Therapeutic Strategy For Severe COVID 19 Pneumonia From Clinical ExperienceDocumento10 pagineTherapeutic Strategy For Severe COVID 19 Pneumonia From Clinical ExperienceHenrie Angelie TamNessuna valutazione finora
- Clinical Practice Guidelines For The Management of Non-Specific Low Back Pain in Primary Care - An Updated OverviewDocumento14 pagineClinical Practice Guidelines For The Management of Non-Specific Low Back Pain in Primary Care - An Updated OverviewCambriaChicoNessuna valutazione finora
- Consensus Recommendations On The Prevention and Management of Surgical Site Infections (SSI) in The Philippine SettingDocumento15 pagineConsensus Recommendations On The Prevention and Management of Surgical Site Infections (SSI) in The Philippine SettingChristine MagallanesNessuna valutazione finora
- 12 FullDocumento31 pagine12 FullAnand KarnawatNessuna valutazione finora
- COVID-19 Pandemic - Impact On Deep Neck Space Infections: A Retrospective Cohort StudyDocumento8 pagineCOVID-19 Pandemic - Impact On Deep Neck Space Infections: A Retrospective Cohort Studymauricia sriNessuna valutazione finora
- ESGO/ESTRO/ESP Guidelines For The Management of Patients With Endometrial CarcinomaDocumento28 pagineESGO/ESTRO/ESP Guidelines For The Management of Patients With Endometrial CarcinomaElisabeth ElidaNessuna valutazione finora
- PS W 14 2017 Annual Report 2016Documento37 paginePS W 14 2017 Annual Report 2016pate malabananNessuna valutazione finora
- Rush2016 PDFDocumento8 pagineRush2016 PDFioanatiuNessuna valutazione finora
- Gonorrhoea 2012Documento24 pagineGonorrhoea 2012sisca widyanasariNessuna valutazione finora
- HerpesDocumento14 pagineHerpesNaila SyifaNessuna valutazione finora
- Sala Vast Ru 2017Documento6 pagineSala Vast Ru 2017Muhammad AmrullahNessuna valutazione finora
- Beuf BourguignonDocumento2 pagineBeuf BourguignonioanatiuNessuna valutazione finora
- Crown Roast Pork: IngredientsDocumento2 pagineCrown Roast Pork: IngredientsioanatiuNessuna valutazione finora
- Occupational Zoonosis Disease - Vitri WidyaningsihDocumento15 pagineOccupational Zoonosis Disease - Vitri WidyaningsihSindi KurniaNessuna valutazione finora
- Surfasafe Disinfectant Detergent For Surfaces and Equipment Fqy PDFDocumento2 pagineSurfasafe Disinfectant Detergent For Surfaces and Equipment Fqy PDFAlaa FasialNessuna valutazione finora
- MIKROBIOLOGIJA SistematikaDocumento5 pagineMIKROBIOLOGIJA SistematikaIvana GudeljNessuna valutazione finora
- Pcap - PathophysiologyDocumento4 paginePcap - PathophysiologyAyla Mar100% (1)
- Covid-19 Vaccination: Knowledge, Attitude & Challenges Among Medical and Nursing Students-A Web Based SurveyDocumento8 pagineCovid-19 Vaccination: Knowledge, Attitude & Challenges Among Medical and Nursing Students-A Web Based SurveyIJAR JOURNALNessuna valutazione finora
- Zoonotic DiseasesDocumento11 pagineZoonotic Diseasesapi-422995346Nessuna valutazione finora
- Antibiotic Study Cheat Sheet October 2018Documento1 paginaAntibiotic Study Cheat Sheet October 2018Nourhan100% (3)
- New Variants of CovidDocumento2 pagineNew Variants of CovidAdrian Jay BeloyNessuna valutazione finora
- First Aid: Dog BitesDocumento35 pagineFirst Aid: Dog BitesHairul MaisarNessuna valutazione finora
- Hepatitis C SlidesDocumento51 pagineHepatitis C SlidesChukwu NedumNessuna valutazione finora
- Systemic BacteriologyDocumento495 pagineSystemic BacteriologyAkash KaranwalNessuna valutazione finora
- FormularyDocumento49 pagineFormularyvijay kumarNessuna valutazione finora
- Hygiene and Human HealthDocumento69 pagineHygiene and Human HealthRalu OroszNessuna valutazione finora
- Develop A Solution To A Specific Ethical Dilemma Faced by A Health Care Professional by Applying Ethical PrinciplesDocumento6 pagineDevelop A Solution To A Specific Ethical Dilemma Faced by A Health Care Professional by Applying Ethical Principlesjossy MulingeNessuna valutazione finora
- Jonah Vaccine ProgramDocumento40 pagineJonah Vaccine ProgramEdwin MagnoNessuna valutazione finora
- AefiDocumento38 pagineAefizedregga2Nessuna valutazione finora
- Who Study Guide - Iimun 2015Documento50 pagineWho Study Guide - Iimun 2015SujayJainNessuna valutazione finora
- PCAP GuidelinesDocumento15 paginePCAP GuidelinesQueenie CuaroNessuna valutazione finora
- Salient Points of The Philippine Blood Banking LawsDocumento76 pagineSalient Points of The Philippine Blood Banking LawsAngelica Parreñas BayonaNessuna valutazione finora
- ArenavirusDocumento29 pagineArenavirusRamirez GiovarNessuna valutazione finora
- Research Methodology and BiostatisticsDocumento163 pagineResearch Methodology and BiostatisticsLourdesNessuna valutazione finora
- Cephalosporins in Veterinary MedicineDocumento23 pagineCephalosporins in Veterinary MedicineSunil100% (3)
- Bleeding DisordersDocumento34 pagineBleeding Disordersbpt2Nessuna valutazione finora
- Norovirus Fact SheetDocumento1 paginaNorovirus Fact SheetovwebmasterNessuna valutazione finora
- Nervous Tissue Anti-Rabies Vaccine For Human UseDocumento2 pagineNervous Tissue Anti-Rabies Vaccine For Human UseLet BNessuna valutazione finora
- Infection Control ManualDocumento205 pagineInfection Control ManualSalah ElbadawyNessuna valutazione finora
- Measles Virus (Rubeola) : Anne A. GershonDocumento10 pagineMeasles Virus (Rubeola) : Anne A. GershonTammy Utami DewiNessuna valutazione finora
- Covid CertificateDocumento1 paginaCovid CertificateTamer BadranNessuna valutazione finora
- February 8, 2021: BioNTech's NONCLINICAL OVERVIEW Submission To FDA For ComirnatyDocumento36 pagineFebruary 8, 2021: BioNTech's NONCLINICAL OVERVIEW Submission To FDA For ComirnatyBrian O'SheaNessuna valutazione finora
- Biographical DataDocumento29 pagineBiographical DataJai - HoNessuna valutazione finora