Potrebbero piacerti anche
- Psalm151 160Documento3 paginePsalm151 160Gina KristenNessuna valutazione finora
- NETTER DermatomDocumento1 paginaNETTER Dermatomngwinda90100% (1)
- Dro SNS 2V-3V (English Manual)Documento59 pagineDro SNS 2V-3V (English Manual)farid said errahmani50% (2)
- P0073-Ambient Air Temperature Sensor Circuit High PDFDocumento5 pagineP0073-Ambient Air Temperature Sensor Circuit High PDFFranklin PerezNessuna valutazione finora
- The Moon That Embrace The SunDocumento36 pagineThe Moon That Embrace The SunNorma PuspitaNessuna valutazione finora
- Frequency Converter English ManualDocumento33 pagineFrequency Converter English Manualproduccion multipack100% (2)
- Motorcycle Troubleshooting ManualDocumento15 pagineMotorcycle Troubleshooting ManualJan Warmerdam100% (1)
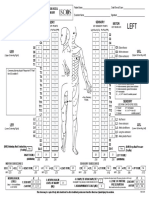
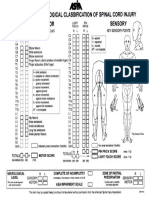
- ASIA International Standards For Neurological Classification of Spinal Cord InjuryDocumento2 pagineASIA International Standards For Neurological Classification of Spinal Cord InjuryMicah Tagle100% (1)
- UER UEL: R L Zone of Partial Preservation R LDocumento2 pagineUER UEL: R L Zone of Partial Preservation R LIridian Berenice Villaseñor XochimitlNessuna valutazione finora
- Formato Escala ASIADocumento2 pagineFormato Escala ASIADavid ParraNessuna valutazione finora
- ASIA ISCOS IntlWorksheet - 2019Documento2 pagineASIA ISCOS IntlWorksheet - 2019Luisa CruzNessuna valutazione finora
- ASIA ISCOS IntlWorksheet 2019Documento2 pagineASIA ISCOS IntlWorksheet 2019Raquel GomesNessuna valutazione finora
- ASIA ISCOS IntlWorksheet 2019Documento2 pagineASIA ISCOS IntlWorksheet 2019Anastasia CanahuateNessuna valutazione finora
- ASIA ISCOS Worksheet - 10.2019 - PRINT Page 1 2Documento2 pagineASIA ISCOS Worksheet - 10.2019 - PRINT Page 1 2Ade Marvira PutriNessuna valutazione finora
- Right Left: UER UELDocumento2 pagineRight Left: UER UELGiieeeNessuna valutazione finora
- Asia PDFDocumento2 pagineAsia PDFIrro Asentista CabelloNessuna valutazione finora
- Patient Name - Date/Time of Exam - Examiner Name - SignatureDocumento1 paginaPatient Name - Date/Time of Exam - Examiner Name - SignatureVineeth ReddyNessuna valutazione finora
- CH01 Sample PDFDocumento32 pagineCH01 Sample PDFDilah RahmaNessuna valutazione finora
- Asia ScaleDocumento1 paginaAsia ScaleShubham SinghNessuna valutazione finora
- Right Totals (Maximum)Documento6 pagineRight Totals (Maximum)kaychi zNessuna valutazione finora
- Pemeriksaan NeurologisDocumento1 paginaPemeriksaan NeurologisLuthfi LazuardiNessuna valutazione finora
- TecnicoDocumento2 pagineTecnicoAbulonNessuna valutazione finora
- Chiro PT FormDocumento4 pagineChiro PT FormMohammad AliNessuna valutazione finora
- Parts Manual: Mini ExcavatorDocumento167 pagineParts Manual: Mini ExcavatorSamuel BenavidesNessuna valutazione finora
- Tissue Cutting BladesDocumento4 pagineTissue Cutting BladesGertie CaiNessuna valutazione finora
- Lecturelbp AngelatulaarforpresentationrecDocumento80 pagineLecturelbp Angelatulaarforpresentationrecamelia rahayuNessuna valutazione finora
- Pointec Catalog PDFDocumento44 paginePointec Catalog PDFPrerak PatelNessuna valutazione finora
- Autumn 2019-20 First In-Sem Exam TimetableDocumento1 paginaAutumn 2019-20 First In-Sem Exam TimetableHari PatelNessuna valutazione finora
- Wiring Diagram: K20A1 Engine: A B C DDocumento1 paginaWiring Diagram: K20A1 Engine: A B C DAlexgavgray GNessuna valutazione finora
- Single Line Wiring Diagram 275M 250kvaDocumento1 paginaSingle Line Wiring Diagram 275M 250kvazeshanjamilNessuna valutazione finora
- Single Line Wiring Diagram 275M 250kva PDFDocumento1 paginaSingle Line Wiring Diagram 275M 250kva PDFzeshanjamilNessuna valutazione finora
- 035 Ext Holders (Screw-On Clamp Series)Documento2 pagine035 Ext Holders (Screw-On Clamp Series)petrus airdropNessuna valutazione finora
- 2013 G 1.6 DOHC MFI Control System Schematic DiagramsDocumento1 pagina2013 G 1.6 DOHC MFI Control System Schematic DiagramsManuel GuevaraNessuna valutazione finora
- Noise Filter: Secondary PrimaryDocumento9 pagineNoise Filter: Secondary PrimaryДенис БородинNessuna valutazione finora
- CT Series: Instruction ManualDocumento2 pagineCT Series: Instruction ManualHelton ClarindoNessuna valutazione finora
- Electrical TWD-110 YuchaiDocumento1 paginaElectrical TWD-110 YuchaizeshanjamilNessuna valutazione finora
- Hub Motor Line-02 Process Validation Sheet - RH - Cover Press - 27.06.2023 - VMAP - ManesarDocumento6 pagineHub Motor Line-02 Process Validation Sheet - RH - Cover Press - 27.06.2023 - VMAP - ManesarRavi KumarNessuna valutazione finora
- UD13466B - Baseline Wireless Output Expander Quick Start Guide V1.2 - 20181013 - MultilanguageDocumento3 pagineUD13466B - Baseline Wireless Output Expander Quick Start Guide V1.2 - 20181013 - MultilanguageEdward GutierrezNessuna valutazione finora
- Jam Code2625Documento89 pagineJam Code2625Phụng MinhNessuna valutazione finora
- 42074-Omranya C SLDDocumento1 pagina42074-Omranya C SLDMuhamed Elsayed - ZalatNessuna valutazione finora
- EDUC1-I - Vježba 2Documento1 paginaEDUC1-I - Vježba 2Zdenko NagyNessuna valutazione finora
- SchematicDocumento2 pagineSchematicjcallistusNessuna valutazione finora
- Ig Toyota TeriosDocumento10 pagineIg Toyota TeriosCarlos Awo OsaureNessuna valutazione finora
- 2019 Gran I10 G 1.2 Mpi-DiagramDocumento1 pagina2019 Gran I10 G 1.2 Mpi-DiagramDarwin MosqueraNessuna valutazione finora
- LC-32E67U: Sharp Electronics Corporation Sharp CorporationDocumento47 pagineLC-32E67U: Sharp Electronics Corporation Sharp Corporationjwb123Nessuna valutazione finora
- Service Intervals and Recommended Maintenance: VT750C / CD / CD2Documento66 pagineService Intervals and Recommended Maintenance: VT750C / CD / CD2Igor Gura100% (1)
- GROUND DISTRIBUTION - Honda Civic Hybrid 2005 - SYSTEM WIRING DIAGRAMSDocumento9 pagineGROUND DISTRIBUTION - Honda Civic Hybrid 2005 - SYSTEM WIRING DIAGRAMSbazucaNessuna valutazione finora
- Locust (Pirate S Bane) LCT-PBDocumento1 paginaLocust (Pirate S Bane) LCT-PBjakester404Nessuna valutazione finora
- 016-035 Oktron eDocumento20 pagine016-035 Oktron eraj_ritu_aNessuna valutazione finora
- CMKS-L Dies Construction Sheet: QIJG:.Documento2 pagineCMKS-L Dies Construction Sheet: QIJG:.Trần Long VũNessuna valutazione finora
- JST Cmkdpsaita03064 Jst-065Documento2 pagineJST Cmkdpsaita03064 Jst-065Trần Long VũNessuna valutazione finora
- Quick Guide Na9300k Aa Dg68 01094a 01 en Mes CFRDocumento20 pagineQuick Guide Na9300k Aa Dg68 01094a 01 en Mes CFRXander OttenNessuna valutazione finora
- Manual MotovibradorDocumento56 pagineManual MotovibradorNicanor CaritasNessuna valutazione finora
- FS9721-LP3 4000 Counts Digital Multimeter: FortuneDocumento32 pagineFS9721-LP3 4000 Counts Digital Multimeter: FortunePlaneta MatrixNessuna valutazione finora
- P076A-Dc Solenoid Circuit: Special Tools: Click To Display A List of Tools Used in This ProcedureDocumento8 pagineP076A-Dc Solenoid Circuit: Special Tools: Click To Display A List of Tools Used in This ProcedureAntonio GallegosNessuna valutazione finora
- (J) Counters: Programmable Counter/Timer CT Series Compact LCD Counter LA8N SeriesDocumento1 pagina(J) Counters: Programmable Counter/Timer CT Series Compact LCD Counter LA8N SeriesMr. Rahul SubramanianNessuna valutazione finora
- Star DeltaDocumento1 paginaStar DeltaVERY YOGA MARULI TUA SIHOMBING TBANessuna valutazione finora
- Jaw CrusherDocumento26 pagineJaw CrusherRufai Muhammad modibboNessuna valutazione finora
- 1SDM000068R0001Documento84 pagine1SDM000068R0001MIGUEL SANCHEZNessuna valutazione finora
- Wiring DiagramsDocumento1 paginaWiring Diagrams조장현Nessuna valutazione finora
- Record SheetsDocumento14 pagineRecord Sheetsjakester404Nessuna valutazione finora
- Second in Sem Exam Schedule Winter 2018-19Documento1 paginaSecond in Sem Exam Schedule Winter 2018-19KeyurNessuna valutazione finora
- Introduction: Science and Environment: Brgy - Pampang, Angeles City, PhilippinesDocumento65 pagineIntroduction: Science and Environment: Brgy - Pampang, Angeles City, PhilippinesLance AustriaNessuna valutazione finora
- Mechanism Design: A SeriesDocumento3 pagineMechanism Design: A Seriesamirmasood kholojiniNessuna valutazione finora
- Exploded View & Parts Listing Air Operated Double Diaphragm PumpDocumento2 pagineExploded View & Parts Listing Air Operated Double Diaphragm PumpCarlos AvalosNessuna valutazione finora
- 4th Semester Electrical Engg.Documento19 pagine4th Semester Electrical Engg.Bhojpuri entertainmentNessuna valutazione finora
- Bsi MD Ivdr Conformity Assessment Routes Booklet Uk enDocumento15 pagineBsi MD Ivdr Conformity Assessment Routes Booklet Uk enGuillaumeNessuna valutazione finora
- Burst Abdomen 3Documento12 pagineBurst Abdomen 3Satvik BansalNessuna valutazione finora
- Habitat Preference of Great Argus Pheasant ArgusiaDocumento11 pagineHabitat Preference of Great Argus Pheasant ArgusiaFaradlina MuftiNessuna valutazione finora
- Design of Cycle Rickshaw For School ChildrenDocumento23 pagineDesign of Cycle Rickshaw For School ChildrenAditya GuptaNessuna valutazione finora
- Company Profile Pt. KPT PDFDocumento23 pagineCompany Profile Pt. KPT PDFfery buyaNessuna valutazione finora
- SweetenersDocumento23 pagineSweetenersNur AfifahNessuna valutazione finora
- UntitledDocumento413 pagineUntitledjgj38j90Nessuna valutazione finora
- Soccer Training DiaryDocumento1 paginaSoccer Training DiaryMark DeaconNessuna valutazione finora
- DUPIXENT Doctor Discussion GuideDocumento4 pagineDUPIXENT Doctor Discussion GuideTAP THANH CHAUNessuna valutazione finora
- 5 160 1 PBDocumento13 pagine5 160 1 PBLotkomoaidone Harahu TukambaNessuna valutazione finora
- DSR Codes - 1Documento108 pagineDSR Codes - 1lakkireddy seshireddyNessuna valutazione finora
- What A Wonderful WorldDocumento3 pagineWhat A Wonderful Worldapi-333684519Nessuna valutazione finora
- The Gingerbread Man-1 EnglishareDocumento40 pagineThe Gingerbread Man-1 EnglishareamayalibelulaNessuna valutazione finora
- Benefits of OTN in Transport SDNDocumento9 pagineBenefits of OTN in Transport SDNGhallab AlsadehNessuna valutazione finora
- Accessories 162-USDocumento20 pagineAccessories 162-USعايد التعزيNessuna valutazione finora
- Nitrogen CycleDocumento12 pagineNitrogen Cycleasa bspcpkNessuna valutazione finora
- DEAD STARS by Paz Marquez BenitezDocumento17 pagineDEAD STARS by Paz Marquez BenitezArmiethazen Khea Page PalarcaNessuna valutazione finora
- Case Study (Co2 Flooding)Documento10 pagineCase Study (Co2 Flooding)Jessica KingNessuna valutazione finora
- Anchor Chart-Describing Words-Descriptive Details of Setting and Character PDFDocumento2 pagineAnchor Chart-Describing Words-Descriptive Details of Setting and Character PDFdellindiaNessuna valutazione finora
- FP Lecture Midterm Exam Sec - Sem.2020Documento4 pagineFP Lecture Midterm Exam Sec - Sem.2020SAEEDA ALMUQAHWINessuna valutazione finora
- The Royal Commonwealth Society of Malaysia: Function MenuDocumento3 pagineThe Royal Commonwealth Society of Malaysia: Function MenuMynak KrishnaNessuna valutazione finora
- American Pile Driving Equipment Equipment CatalogDocumento25 pagineAmerican Pile Driving Equipment Equipment CatalogW Morales100% (1)