Potrebbero piacerti anche
- Case Simu 101Documento5 pagineCase Simu 101Princess Levie CenizaNessuna valutazione finora
- DewormingDocumento48 pagineDewormingJulie Ann Escartin80% (5)
- Clinical Nursing JudgmentDocumento7 pagineClinical Nursing Judgmentapi-502994344Nessuna valutazione finora
- Ati RN 2016 Mental HealthDocumento6 pagineAti RN 2016 Mental HealthStan Tan0% (1)
- 1358453842.3856hematology Question BankDocumento182 pagine1358453842.3856hematology Question BankKay BristolNessuna valutazione finora
- Growth Hormone DisordersDocumento1 paginaGrowth Hormone DisordersVishalNessuna valutazione finora
- Prioritization LectureDocumento6 paginePrioritization LecturesamNessuna valutazione finora
- 31 Acid Base Imbalances ABGs II - 230110 - 004938Documento2 pagine31 Acid Base Imbalances ABGs II - 230110 - 004938JanaNessuna valutazione finora
- Pediatric Pharmacology 07Documento45 paginePediatric Pharmacology 07Nadz CyNessuna valutazione finora
- Concept Map CholesectomyDocumento3 pagineConcept Map CholesectomyDoreen Claire100% (1)
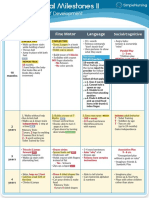
- Visual Chart 2 - Developmental MilestonesDocumento1 paginaVisual Chart 2 - Developmental MilestonesVishalNessuna valutazione finora
- Prof. Sandra M. Covarrubias - September 24, 2021: 5.2fluid & Electrolytes ImbalancesDocumento5 pagineProf. Sandra M. Covarrubias - September 24, 2021: 5.2fluid & Electrolytes ImbalancesIvy VillalobosNessuna valutazione finora
- Maternal Ob NotesDocumento103 pagineMaternal Ob NotesBoris OrbetaNessuna valutazione finora
- Asthma - Pathom, Signs & ComlicationsDocumento1 paginaAsthma - Pathom, Signs & ComlicationsVishalNessuna valutazione finora
- Parenting Styles: - Dictatorial or AuthoritarianDocumento45 pagineParenting Styles: - Dictatorial or AuthoritarianCourseTree LearningNessuna valutazione finora
- Global Nursing Pediatrics. Nclex - RNDocumento14 pagineGlobal Nursing Pediatrics. Nclex - RNNANANessuna valutazione finora
- OB Quizlet3 Nursing Care of ChildrenDocumento6 pagineOB Quizlet3 Nursing Care of ChildrenDanielle ShullNessuna valutazione finora
- Musculoskeletal Disorders: Aurang ZebDocumento73 pagineMusculoskeletal Disorders: Aurang ZebMuhammadNessuna valutazione finora
- EndocrineDocumento2 pagineEndocrineUnclePorkchopNessuna valutazione finora
- Approaches To Common Pediatric Disease and Injury:: An Emergency Room PerspectiveDocumento67 pagineApproaches To Common Pediatric Disease and Injury:: An Emergency Room PerspectiveKarl RobleNessuna valutazione finora
- Focused ReviewDocumento6 pagineFocused ReviewGina GiammalvoNessuna valutazione finora
- Endocrine: Common Lab Tests For Endocrine and Hormonal DisordersDocumento19 pagineEndocrine: Common Lab Tests For Endocrine and Hormonal DisordersPhilip SimanganNessuna valutazione finora
- Kaplan Focus ReviewDocumento9 pagineKaplan Focus ReviewSaidel ElizondoNessuna valutazione finora
- Unit 1 Definitions/key Terms Varcarolis Mental Health NursingDocumento6 pagineUnit 1 Definitions/key Terms Varcarolis Mental Health Nursingatl_nurse_studentNessuna valutazione finora
- Testing Strategies For The Nclex-Rn Examination: Chapter OneDocumento22 pagineTesting Strategies For The Nclex-Rn Examination: Chapter OneShiraishiNessuna valutazione finora
- Part I: Emergency Department (ED) : SKINNY ReasoningDocumento6 paginePart I: Emergency Department (ED) : SKINNY ReasoningUzumaki KNessuna valutazione finora
- Fluid Overload Student PagesDocumento4 pagineFluid Overload Student PagesJess OswaldNessuna valutazione finora
- Understanding Growth and Development ToddlersDocumento3 pagineUnderstanding Growth and Development ToddlersSimranNessuna valutazione finora
- Hyperemesis Gravidarum: Bleeding Complications of PregnancyDocumento6 pagineHyperemesis Gravidarum: Bleeding Complications of PregnancykirbsNessuna valutazione finora
- Medical-Surgical Nursing: Perioperative OverviewDocumento24 pagineMedical-Surgical Nursing: Perioperative OverviewSheena Ann L. LLarenasNessuna valutazione finora
- Mark Klimek NCLEX ReviewDocumento67 pagineMark Klimek NCLEX ReviewJohanisah Casidar MacarambonNessuna valutazione finora
- Cranial NervesDocumento6 pagineCranial Nervesvienny kayeNessuna valutazione finora
- Function of G I System: The Primary Digestive Functions Are Break Down Food Particles "Documento113 pagineFunction of G I System: The Primary Digestive Functions Are Break Down Food Particles "cherryann_12100% (1)
- GGGGHHDocumento7 pagineGGGGHHนีล ไบรอันNessuna valutazione finora
- Ineffective Coping - Nursing Diagnosis & Care Plan - NurseslabsDocumento13 pagineIneffective Coping - Nursing Diagnosis & Care Plan - NurseslabsLester MooreNessuna valutazione finora
- Physiological IntegrityDocumento317 paginePhysiological IntegrityMoreiyamNessuna valutazione finora
- VSim SARAH LIN For Nursing - Health Assessment POST QUIZDocumento5 pagineVSim SARAH LIN For Nursing - Health Assessment POST QUIZWen RodsaNessuna valutazione finora
- Immunity 1Documento6 pagineImmunity 1Tori RolandNessuna valutazione finora
- Basic Chart 1 of 2 - Delopmental MilestonesDocumento1 paginaBasic Chart 1 of 2 - Delopmental MilestonesVishalNessuna valutazione finora
- Asthma That Disappears Between Ages 6-8 - Bronchioles Grew & Resolved The AsthmaDocumento27 pagineAsthma That Disappears Between Ages 6-8 - Bronchioles Grew & Resolved The Asthmasimonedarling100% (1)
- 2017 Fluid and Electrolytes LECTURE NOTESDocumento34 pagine2017 Fluid and Electrolytes LECTURE NOTESHarley Justiniani Dela CruzNessuna valutazione finora
- Bullets Nclex Terms 50Documento48 pagineBullets Nclex Terms 50ShazaNessuna valutazione finora
- Https:Jetmapp - orbundsis.com:Einstein-freshair:Videos::102793DigitalDownload LabValues NurseInTheMaking 2pagesDocumento5 pagineHttps:Jetmapp - orbundsis.com:Einstein-freshair:Videos::102793DigitalDownload LabValues NurseInTheMaking 2pagesamazonian005100% (1)
- Pediatric MedicationsDocumento25 paginePediatric MedicationsGloryJaneNessuna valutazione finora
- Ati RN 2016 NutritionDocumento6 pagineAti RN 2016 NutritionStan Tan0% (1)
- NCLEX 15 WK 1critical ThinkingDocumento2 pagineNCLEX 15 WK 1critical ThinkingNikita TamrakarNessuna valutazione finora
- Endocrine MedicationsDocumento47 pagineEndocrine MedicationsAamir AzizNessuna valutazione finora
- Presented By: Anjani.S.Kamal 1 Year MSC (N)Documento23 paginePresented By: Anjani.S.Kamal 1 Year MSC (N)shubham vermaNessuna valutazione finora
- Muscoskeletal DisordersDocumento17 pagineMuscoskeletal DisordersAntonio Andag SalasNessuna valutazione finora
- Review of Systems ANDREADocumento7 pagineReview of Systems ANDREAAndrea Dora OrtalizNessuna valutazione finora
- Ati Pharm 2011 BDocumento4 pagineAti Pharm 2011 BStan Tan50% (2)
- GI Signs and SymptomsDocumento40 pagineGI Signs and SymptomsJohnny BeeNessuna valutazione finora
- Hypertension Potassium: DO NOT Delegate What You Can EAT! E - Evaluate A - Assess T - TeachDocumento35 pagineHypertension Potassium: DO NOT Delegate What You Can EAT! E - Evaluate A - Assess T - TeachEsterly Puracan AmparoNessuna valutazione finora
- TonsillitisDocumento1 paginaTonsillitisVishalNessuna valutazione finora
- Ch. 1, Lesson 1: What Is The Next Gen NCLEXDocumento4 pagineCh. 1, Lesson 1: What Is The Next Gen NCLEXChantelNessuna valutazione finora
- Nursing ProcessDocumento12 pagineNursing Processgrey26Nessuna valutazione finora
- Cardiac Mnemonics/ Memory CardsDocumento35 pagineCardiac Mnemonics/ Memory CardsLids70Nessuna valutazione finora
- Concept Map TemplateDocumento16 pagineConcept Map Templatenursing concept mapsNessuna valutazione finora
- Funds Study Guide 29Documento29 pagineFunds Study Guide 29Vin Lorenzo CampbellNessuna valutazione finora
- COMPREHENSIVE NURSING ACHIEVEMENT TEST (RN): Passbooks Study GuideDa EverandCOMPREHENSIVE NURSING ACHIEVEMENT TEST (RN): Passbooks Study GuideNessuna valutazione finora
- 14 Fun Facts About Your Heart: Educational VersionDa Everand14 Fun Facts About Your Heart: Educational VersionNessuna valutazione finora
- 2423 20160427105703 FbcfiDocumento16 pagine2423 20160427105703 FbcfiCorrinne Mah Yoke Yin0% (1)
- Behind The Tower of BabelDocumento310 pagineBehind The Tower of Babelmartyken100% (1)
- Prospectus PDFDocumento68 pagineProspectus PDFPrince Digital ComputersNessuna valutazione finora
- Pathogenesis of PcosDocumento14 paginePathogenesis of PcosMitali Narurkar100% (1)
- KetamineDocumento4 pagineKetamineapi-235915759Nessuna valutazione finora
- Metoprolol and AmiodaroneDocumento5 pagineMetoprolol and AmiodaroneNolte BombayNessuna valutazione finora
- Radiologi Kedaruratan & Traumatologi-Prof. Dr. Bachtiar MDocumento55 pagineRadiologi Kedaruratan & Traumatologi-Prof. Dr. Bachtiar MMonazzt AsshagabNessuna valutazione finora
- Research EssasyDocumento9 pagineResearch Essasyapi-279881900Nessuna valutazione finora
- Introduction To Anatomy and Homeostasis Within The BodyDocumento24 pagineIntroduction To Anatomy and Homeostasis Within The BodyTrinity SherNessuna valutazione finora
- Drug Therapy in Pregnancy (Soal)Documento6 pagineDrug Therapy in Pregnancy (Soal)Yola FebriyantiNessuna valutazione finora
- Fluids and Electrolytes Study GuideDocumento13 pagineFluids and Electrolytes Study GuideElizabeth McKeeNessuna valutazione finora
- National Congress of Veterinary Medicine Students HISTORYDocumento3 pagineNational Congress of Veterinary Medicine Students HISTORYRoyd Joseph R. MosasoNessuna valutazione finora
- RXN For DR - SagamlaDocumento2 pagineRXN For DR - Sagamlayeng botzNessuna valutazione finora
- Cesarean Surgical Techniques - GLOWMDocumento36 pagineCesarean Surgical Techniques - GLOWMOana BalintNessuna valutazione finora
- Real - VITAL-SIGNS ChecklistDocumento2 pagineReal - VITAL-SIGNS ChecklistLoraine SandovalNessuna valutazione finora
- Simultaneous Determination of Methylparaben + Propylparaben + Hidrocortisone Topical Cream PDFDocumento7 pagineSimultaneous Determination of Methylparaben + Propylparaben + Hidrocortisone Topical Cream PDFNájla KassabNessuna valutazione finora
- Physical Capabilities of Instructors at The End of Hot Fire Training (0305) (158529)Documento42 paginePhysical Capabilities of Instructors at The End of Hot Fire Training (0305) (158529)Onion PapaNessuna valutazione finora
- Nine Principles For Improved Nurse Staffing by Bob DentDocumento6 pagineNine Principles For Improved Nurse Staffing by Bob DentJennyLapitanNessuna valutazione finora
- Postmenopausal OSTEOPOROSIS GuidelinesDocumento42 paginePostmenopausal OSTEOPOROSIS GuidelinesAbelNessuna valutazione finora
- Coci Gram - Bacili Gram + Bacili Gram - Fam. EnterobacteriaceaeDocumento1 paginaCoci Gram - Bacili Gram + Bacili Gram - Fam. Enterobacteriaceaeodiseu81Nessuna valutazione finora
- Interns 2016 DistributionDocumento13 pagineInterns 2016 DistributionKashish ChawlaNessuna valutazione finora
- Beyond Schein DentalDocumento9 pagineBeyond Schein DentaltomdietzlerNessuna valutazione finora
- Neurotransmitters & NeuromodulatorsDocumento41 pagineNeurotransmitters & Neuromodulatorsafiwahyu100% (1)
- Grafic AsistentiDocumento64 pagineGrafic AsistentibadeaNessuna valutazione finora
- UKA: When Would I Do It?Documento35 pagineUKA: When Would I Do It?neareastspineNessuna valutazione finora
- Doctor Mi Kay Khau Nandini DhargalkarDocumento51 pagineDoctor Mi Kay Khau Nandini Dhargalkarabmopalhvac0% (1)
- Cardioversion of Atrial Fibrillation and AtrialDocumento13 pagineCardioversion of Atrial Fibrillation and AtrialLabontu IustinaNessuna valutazione finora
- What Is Personal HygieneDocumento4 pagineWhat Is Personal HygieneAnonymous 0FWhoTu100% (1)