Potrebbero piacerti anche
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- Cloete 2018 Scielo South AfricaDocumento10 pagineCloete 2018 Scielo South AfricalibremdNessuna valutazione finora
- Boukary 2012 Plos OneDocumento12 pagineBoukary 2012 Plos OnelibremdNessuna valutazione finora
- Zhang 2019 Plos NTDDocumento20 pagineZhang 2019 Plos NTDlibremdNessuna valutazione finora
- Questions To Integrate A Gender Perspective Into Research CooperationDocumento3 pagineQuestions To Integrate A Gender Perspective Into Research CooperationlibremdNessuna valutazione finora
- Arnault 2008 Is There An Asian Idiom of Distress Somatic Symptoms in FemaleDocumento15 pagineArnault 2008 Is There An Asian Idiom of Distress Somatic Symptoms in FemalelibremdNessuna valutazione finora
- Curriculum Vitae Ladson Hinton Personal Information: Lwhinton@ucdavis - EduDocumento34 pagineCurriculum Vitae Ladson Hinton Personal Information: Lwhinton@ucdavis - EdulibremdNessuna valutazione finora
- Multinomial Logistic Regression Basic RelationshipsDocumento73 pagineMultinomial Logistic Regression Basic RelationshipslibremdNessuna valutazione finora
- No Woman Should Die Giving LifeDocumento112 pagineNo Woman Should Die Giving LifelibremdNessuna valutazione finora
- Nguyen Minh Tuan 2013Documento8 pagineNguyen Minh Tuan 2013libremdNessuna valutazione finora
- Nutrition Transition in 2 Lowland Bolivian Subsistence PopulationsDocumento13 pagineNutrition Transition in 2 Lowland Bolivian Subsistence PopulationslibremdNessuna valutazione finora
- Cineforum 2017: Director: Davis GuggenheimDocumento1 paginaCineforum 2017: Director: Davis GuggenheimlibremdNessuna valutazione finora
- Tesis AlirezaDocumento98 pagineTesis AlirezalibremdNessuna valutazione finora
- Clinical Dementia Rating Worksheet: Memory Questions For InformantDocumento10 pagineClinical Dementia Rating Worksheet: Memory Questions For InformantlibremdNessuna valutazione finora
- Fahetal2010 PDFDocumento10 pagineFahetal2010 PDFlibremdNessuna valutazione finora
- Call For Abstracts Social Inequity in Health SymposiumDocumento1 paginaCall For Abstracts Social Inequity in Health SymposiumlibremdNessuna valutazione finora
- Welcomeletter Research Method and Philosophy November 2014Documento1 paginaWelcomeletter Research Method and Philosophy November 2014libremdNessuna valutazione finora
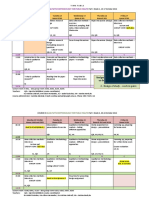
- QM 1 Schedule 2014-15 Final 0930 CambroDocumento2 pagineQM 1 Schedule 2014-15 Final 0930 CambrolibremdNessuna valutazione finora
- Abstract Book Leish World Congress 5Documento1.116 pagineAbstract Book Leish World Congress 5libremdNessuna valutazione finora
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (74)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- CIAVDocumento5 pagineCIAVAdolfo KwanNessuna valutazione finora
- Smoking and Malignancy in Sinonasal Inverted PapillomaDocumento5 pagineSmoking and Malignancy in Sinonasal Inverted Papillomadarmayanti ibnuNessuna valutazione finora
- Role of The Nurse in Stroke RehabilitationDocumento2 pagineRole of The Nurse in Stroke RehabilitationAnonymous mTqyS6Nessuna valutazione finora
- 2020 03 31 Guidance To Safely Send and Receive Resources Between School and HomeDocumento5 pagine2020 03 31 Guidance To Safely Send and Receive Resources Between School and HomeJimmellee EllenNessuna valutazione finora
- HDU AuditDocumento3 pagineHDU AuditAsdf DgfhgNessuna valutazione finora
- MedicineDocumento34 pagineMedicinezaher jubeiliNessuna valutazione finora
- Community Health Nursing 116 final exam 19/12/2019 دونج تايحت عم 116 نيلوهجملا MCQDocumento6 pagineCommunity Health Nursing 116 final exam 19/12/2019 دونج تايحت عم 116 نيلوهجملا MCQA.A M.A.RNessuna valutazione finora
- Incursions Learning Objectives/Study Guide: EEDA/IAT Web-Based CourseDocumento7 pagineIncursions Learning Objectives/Study Guide: EEDA/IAT Web-Based Coursevdcastillo13Nessuna valutazione finora
- Dimension of Development: Health Awareness: Nstp-Cwts Chapter 6Documento8 pagineDimension of Development: Health Awareness: Nstp-Cwts Chapter 6Rika Mae100% (3)
- Annexures 8-10 For PWDDocumento5 pagineAnnexures 8-10 For PWDAbhishek TiwariNessuna valutazione finora
- Celiac DiseaseDocumento14 pagineCeliac Diseasebibhutimah02Nessuna valutazione finora
- Smallpox Pamphlet Group 2Documento3 pagineSmallpox Pamphlet Group 2classdocsNessuna valutazione finora
- Principles of Infection Control and Personal Protective EquipmentDocumento94 paginePrinciples of Infection Control and Personal Protective EquipmentBidsandAwardsCommittee CagayanValleyMedicalCenterNessuna valutazione finora
- LS - GCL - Individual Above NEL Form - FillableDocumento1 paginaLS - GCL - Individual Above NEL Form - FillableJerald Peter VargasNessuna valutazione finora
- 29-09-2020 HMB EnglishDocumento22 pagine29-09-2020 HMB EnglishNeeraj S GNessuna valutazione finora
- Belanja Online Di Masa Pandemi Covid-19: Studi Kasus Ibu-Ibu Rumah Tangga Di MakassarDocumento15 pagineBelanja Online Di Masa Pandemi Covid-19: Studi Kasus Ibu-Ibu Rumah Tangga Di MakassarAmeliaphutri PutriNessuna valutazione finora
- Asthma Treatment GuidlineDocumento56 pagineAsthma Treatment GuidlineEsther OdumanyeNessuna valutazione finora
- Body-Weakness-Ncp X Drug StudyDocumento3 pagineBody-Weakness-Ncp X Drug Studyhayascent hilarioNessuna valutazione finora
- Epidemiological and Nutrition Transition in Developing Countries: Impact On Human Health and DevelopmentDocumento9 pagineEpidemiological and Nutrition Transition in Developing Countries: Impact On Human Health and DevelopmentariniNessuna valutazione finora
- BMJ 22-09Documento15 pagineBMJ 22-09Kiran ShahNessuna valutazione finora
- QuizDocumento8 pagineQuizTareq EmadNessuna valutazione finora
- Uji Reliabilitas Brief Peripheral NeuropathyDocumento7 pagineUji Reliabilitas Brief Peripheral NeuropathyfauzihidayatNessuna valutazione finora
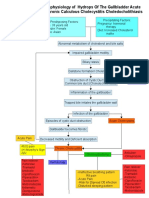
- Pathophysiology of CholecystitisDocumento2 paginePathophysiology of CholecystitisAnonymous gDp7y3Cl82% (22)
- Epidemiology Computational ModelsDocumento16 pagineEpidemiology Computational ModelsIbrahim Jynx FalamaNessuna valutazione finora
- CRCDocumento5 pagineCRCanon_619577898Nessuna valutazione finora
- Case Study For PneumoniaDocumento11 pagineCase Study For PneumoniaGabbii Cinco100% (1)
- IMNCIDocumento84 pagineIMNCIAyenew100% (1)
- Coronavirus Disease (COVID-19) : Case Investigation FormDocumento2 pagineCoronavirus Disease (COVID-19) : Case Investigation FormJudeLaxNessuna valutazione finora
- Epidemiology AssignmentDocumento12 pagineEpidemiology AssignmentSagar ParajuliNessuna valutazione finora
- 1502 DiseasesFromMedicalSystemDocumento7 pagine1502 DiseasesFromMedicalSystemTaste manNessuna valutazione finora