Potrebbero piacerti anche
- Pharmacology Drug Chart: Drug Name Receptor Therapeutic Uses Adverse EffectsDocumento18 paginePharmacology Drug Chart: Drug Name Receptor Therapeutic Uses Adverse EffectsPadmavathy Naidu Chokkapu100% (2)
- Local Anesthetics - Blockers K+ Channel Blockers Ca2+ Channel BlockersDocumento4 pagineLocal Anesthetics - Blockers K+ Channel Blockers Ca2+ Channel Blockersmed testNessuna valutazione finora
- ANS DrugsDocumento2 pagineANS Drugsmed testNessuna valutazione finora
- Coagulation DrugsDocumento1 paginaCoagulation Drugsmed testNessuna valutazione finora
- Opioids PDFDocumento2 pagineOpioids PDFErica Hyeyeon LeeNessuna valutazione finora
- Opioids PDFDocumento2 pagineOpioids PDFErica Hyeyeon LeeNessuna valutazione finora
- Cardiac Meds CompleteDocumento3 pagineCardiac Meds CompleteDanielle100% (2)
- Electrocardiography (Ecg) : Presented By: Fahad I. HussienDocumento102 pagineElectrocardiography (Ecg) : Presented By: Fahad I. HussienMustafa A. DawoodNessuna valutazione finora
- Combat StressDocumento94 pagineCombat StressClaudia Maria Ivan100% (1)
- Asthma - Respiratory PDFDocumento1 paginaAsthma - Respiratory PDFErica Hyeyeon Lee0% (1)
- Pharm-Drugs ChartsDocumento21 paginePharm-Drugs ChartsCandace Flowers100% (3)
- ECG Interpretations GoodDocumento104 pagineECG Interpretations GoodaymenNessuna valutazione finora
- Cardiovascular Pharmacology 7-2010Documento67 pagineCardiovascular Pharmacology 7-2010Catlyn Chatpman100% (1)
- Antiarrhythmic Medication Chart - EBM Consult v3Documento2 pagineAntiarrhythmic Medication Chart - EBM Consult v3Linlin100% (1)
- ECGcheatsheet PDFDocumento1 paginaECGcheatsheet PDFTush RameNessuna valutazione finora
- Review Handouts For Medical Pharmacology PDFDocumento21 pagineReview Handouts For Medical Pharmacology PDFAndres F. TorresNessuna valutazione finora
- CardionotesDocumento5 pagineCardionotesNichole Coletta100% (1)
- Internal Medicine #1Documento167 pagineInternal Medicine #1Nikhil RayarakulaNessuna valutazione finora
- Sphere: These DiarrheaDocumento3 pagineSphere: These Diarrheamed testNessuna valutazione finora
- Antibiotics Cheat SheetDocumento2 pagineAntibiotics Cheat SheetAlejandro Rodas Salinas100% (1)
- CVPR Prototype Drugs TableDocumento27 pagineCVPR Prototype Drugs TablethommyvaNessuna valutazione finora
- Induction Agents MOA Onset, Duration Special Uses / Notes PropofolDocumento3 pagineInduction Agents MOA Onset, Duration Special Uses / Notes PropofolpaveethrahNessuna valutazione finora
- DRUG of CHOICE - InfectiousDocumento1 paginaDRUG of CHOICE - InfectiousJoseph De JoyaNessuna valutazione finora
- Ninja - Antihyperlipidemics PDFDocumento3 pagineNinja - Antihyperlipidemics PDFErica Hyeyeon Lee100% (1)
- Know Common Disease ManagementDocumento14 pagineKnow Common Disease Managementcdx25Nessuna valutazione finora
- Hypertension Drugs Cheat Sheet: by ViaDocumento3 pagineHypertension Drugs Cheat Sheet: by ViaGulzaib KhokharNessuna valutazione finora
- Ninja - Anti-Coagulants PDFDocumento3 pagineNinja - Anti-Coagulants PDFErica Hyeyeon Lee100% (1)
- Ninja - Anti-Coagulants PDFDocumento3 pagineNinja - Anti-Coagulants PDFErica Hyeyeon Lee100% (1)
- Renal Guide and Charts: AlbuminDocumento16 pagineRenal Guide and Charts: AlbuminYaima JimenezNessuna valutazione finora
- NSAIDS and SteroidsDocumento2 pagineNSAIDS and Steroidsmed testNessuna valutazione finora
- Legal - Register - Manufacturing Service (Aug '17) .Documento8 pagineLegal - Register - Manufacturing Service (Aug '17) .jagshishNessuna valutazione finora
- 60 Substance Abuse Group Therapy ActivitiesDocumento7 pagine60 Substance Abuse Group Therapy ActivitiesHanes Labajos100% (1)
- GI Drugs PDFDocumento6 pagineGI Drugs PDFErica Hyeyeon Lee100% (1)
- GI Drugs PDFDocumento6 pagineGI Drugs PDFErica Hyeyeon Lee100% (1)
- Ninja - Anti-HTN PDFDocumento6 pagineNinja - Anti-HTN PDFErica Hyeyeon Lee100% (2)
- Ninja - Anti-HTN PDFDocumento6 pagineNinja - Anti-HTN PDFErica Hyeyeon Lee100% (2)
- Ninja - Cholinergic Drugs PDFDocumento4 pagineNinja - Cholinergic Drugs PDFErica Hyeyeon Lee100% (2)
- Ninja - Cholinergic Drugs PDFDocumento4 pagineNinja - Cholinergic Drugs PDFErica Hyeyeon Lee100% (2)
- Week 4.1 The Law of ResonanceDocumento12 pagineWeek 4.1 The Law of ResonanceWim Massop100% (1)
- Guaranteed To Pass: Exam Tidbits in Easy To Digest, Bite Sized MorselsDocumento2 pagineGuaranteed To Pass: Exam Tidbits in Easy To Digest, Bite Sized MorselsAmberNessuna valutazione finora
- Bleeding During Pregnancy and Nursing Care PlanDocumento17 pagineBleeding During Pregnancy and Nursing Care PlanLizcelle Bihasa86% (7)
- Cardiovascular Drug IntroductionDocumento3 pagineCardiovascular Drug IntroductionSamah Khan100% (1)
- Antibiotic TableDocumento7 pagineAntibiotic TablenkuligowskiNessuna valutazione finora
- Local Government Financial Statistics England #23-2013Documento222 pagineLocal Government Financial Statistics England #23-2013Xavier Endeudado Ariztía FischerNessuna valutazione finora
- Antiarrhythmic DrugsDocumento3 pagineAntiarrhythmic DrugsdoktorcoopNessuna valutazione finora
- Critical Care Drug Reference SheetDocumento12 pagineCritical Care Drug Reference SheetYanina CoxNessuna valutazione finora
- Glomerulonephritis Cheat Sheet PDFDocumento1 paginaGlomerulonephritis Cheat Sheet PDFAnonymous aA9Ol6239Nessuna valutazione finora
- Drug Name Onset Concentration Dosing Instructions Drug Class How To TitrateDocumento1 paginaDrug Name Onset Concentration Dosing Instructions Drug Class How To Titrateje hanNessuna valutazione finora
- Updated Antibiotic Chart - 2016 PDFDocumento2 pagineUpdated Antibiotic Chart - 2016 PDFmugenzi eric100% (1)
- Advanced Ekg Interpretation: Micelle J. Haydel, M.D. LSU New Orleans Emergency MedicineDocumento88 pagineAdvanced Ekg Interpretation: Micelle J. Haydel, M.D. LSU New Orleans Emergency MedicineRoroNessuna valutazione finora
- Drug ChartDocumento8 pagineDrug Chartstudentalwaysstudy100% (1)
- Antiarrhythmic Drugs 1Documento32 pagineAntiarrhythmic Drugs 1AliImadAlKhasakiNessuna valutazione finora
- Zombie Brains PDFDocumento1 paginaZombie Brains PDFLorna GrayNessuna valutazione finora
- Antipsychotics - AMBOSS PDFDocumento7 pagineAntipsychotics - AMBOSS PDFOpio Isaac100% (1)
- Antiarrhythmic Drugs: Dr. Hiwa K. Saaed PH.D Pharmacology and ToxicologyDocumento79 pagineAntiarrhythmic Drugs: Dr. Hiwa K. Saaed PH.D Pharmacology and ToxicologyPrasan Bhandari100% (1)
- Musculoskeletal PharmacologyDocumento18 pagineMusculoskeletal PharmacologyBLEEMAGE100% (2)
- Pharmacology ChartDocumento23 paginePharmacology ChartKelly Milaski0% (1)
- Antiarrhythmic DrugsDocumento10 pagineAntiarrhythmic DrugsUma MounaNessuna valutazione finora
- A. Anti-Arrhythmic B.tech 5th SemDocumento49 pagineA. Anti-Arrhythmic B.tech 5th SemNitesh SinghNessuna valutazione finora
- Antibacterial Drugs SummaryDocumento13 pagineAntibacterial Drugs SummaryNeo Ramagaga100% (1)
- Groupwork Proposal BSW 3705 June 2022Documento17 pagineGroupwork Proposal BSW 3705 June 2022Mtshali Nthuseng100% (1)
- Binder 1Documento98 pagineBinder 1Anupama Poulose100% (1)
- 0.5. ANS Quicksheet PDFDocumento1 pagina0.5. ANS Quicksheet PDFErica Hyeyeon LeeNessuna valutazione finora
- Ninja - Antianginal Drugs PDFDocumento2 pagineNinja - Antianginal Drugs PDFErica Hyeyeon LeeNessuna valutazione finora
- Ninja - Autacoids PDFDocumento3 pagineNinja - Autacoids PDFErica Hyeyeon LeeNessuna valutazione finora
- Ninja - Anemias PDFDocumento1 paginaNinja - Anemias PDFErica Hyeyeon LeeNessuna valutazione finora
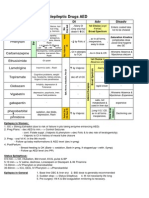
- Antiepileptic Drugs AED: D' DI Disadv SE AdvDocumento1 paginaAntiepileptic Drugs AED: D' DI Disadv SE Advrayooona88Nessuna valutazione finora
- Ace Inhibitors MnemonicDocumento1 paginaAce Inhibitors MnemonicGirish Waru0% (2)
- Cardiac Drugs HypertensionDocumento5 pagineCardiac Drugs HypertensionEciOwnsMeNessuna valutazione finora
- MBBS Antiarrhythmics 2014 Class II (Antiarrhythmic Drugs)Documento23 pagineMBBS Antiarrhythmics 2014 Class II (Antiarrhythmic Drugs)Dr.U.P.Rathnakar.MD.DIH.PGDHM100% (1)
- ArythmicDocumento40 pagineArythmicChia Yin NgNessuna valutazione finora
- Antiarrhythmic DrugsDocumento42 pagineAntiarrhythmic DrugsDr Hotimah HotimahNessuna valutazione finora
- Antiarrhythmic Drugs 2020Documento5 pagineAntiarrhythmic Drugs 2020bobNessuna valutazione finora
- Immunopharmacology PDFDocumento2 pagineImmunopharmacology PDFErica Hyeyeon LeeNessuna valutazione finora
- Ninja - Anemias PDFDocumento1 paginaNinja - Anemias PDFErica Hyeyeon LeeNessuna valutazione finora
- Ninja - Autacoids PDFDocumento3 pagineNinja - Autacoids PDFErica Hyeyeon LeeNessuna valutazione finora
- Ninja - Antianginal Drugs PDFDocumento2 pagineNinja - Antianginal Drugs PDFErica Hyeyeon LeeNessuna valutazione finora
- PHC Assignment 1Documento5 paginePHC Assignment 1Florenze Laiza Donor Lucas100% (1)
- 10 1007@s00068-mfjrbtDocumento14 pagine10 1007@s00068-mfjrbtJGunar VasquezNessuna valutazione finora
- Alprazolam: Why Is This Medicine Prescribed To You?Documento1 paginaAlprazolam: Why Is This Medicine Prescribed To You?Jerome GeronimoNessuna valutazione finora
- Gap AnalysisDocumento9 pagineGap Analysisapi-706947027Nessuna valutazione finora
- Phys Ther 2012 Macedo 363 77Documento18 paginePhys Ther 2012 Macedo 363 77Anang FajarNessuna valutazione finora
- 2022 Projects City of BethlehemDocumento17 pagine2022 Projects City of BethlehemLVNewsdotcomNessuna valutazione finora
- Manual Capsule Filling Machine DimensionsDocumento5 pagineManual Capsule Filling Machine Dimensionsamit chavanNessuna valutazione finora
- Case Report MyelopathyDocumento29 pagineCase Report MyelopathyNurul Hasanah SururyNessuna valutazione finora
- ProVari ManualDocumento16 pagineProVari ManualPatrickNessuna valutazione finora
- Practice Sheet Session 2 - 2021 - Student SheetDocumento2 paginePractice Sheet Session 2 - 2021 - Student SheetAlisa SayNessuna valutazione finora
- Clinical Practice Guidelines: High-Grade Glioma: ESMO Clinical Practice Guidelines For Diagnosis, Treatment and Follow-UpDocumento9 pagineClinical Practice Guidelines: High-Grade Glioma: ESMO Clinical Practice Guidelines For Diagnosis, Treatment and Follow-UpSiva SubramaniamNessuna valutazione finora
- MSDS PDFDocumento5 pagineMSDS PDFdang2172014Nessuna valutazione finora
- Experiment 9 - Hydrolysis of CarbohydratesDocumento2 pagineExperiment 9 - Hydrolysis of CarbohydratesJuren LasagaNessuna valutazione finora
- Ellness F T I O: Rom He Nside UtDocumento5 pagineEllness F T I O: Rom He Nside UthbgossNessuna valutazione finora
- HeartDocumento12 pagineHeartRebar photographyNessuna valutazione finora
- 21.JMM Promotion and Management, Inc. vs. Court of AppealsDocumento3 pagine21.JMM Promotion and Management, Inc. vs. Court of AppealsnathNessuna valutazione finora
- Ponr 1Documento14 paginePonr 1Jhade RelletaNessuna valutazione finora
- Syba Economics Syll 20-21Documento13 pagineSyba Economics Syll 20-21Saniya ShaikhNessuna valutazione finora
- Physical Fitness Test Individual Score CardDocumento12 paginePhysical Fitness Test Individual Score CardJunessa TadinaNessuna valutazione finora
- JHU Press Fall 2013 CatalogDocumento99 pagineJHU Press Fall 2013 CatalogjhupressNessuna valutazione finora
- Bkerzay Wellness BrochureDocumento1 paginaBkerzay Wellness BrochureSandra Abou JaoudehNessuna valutazione finora