Potrebbero piacerti anche
- Managing Medical Devices within a Regulatory FrameworkDa EverandManaging Medical Devices within a Regulatory FrameworkBeth Ann FiedlerValutazione: 5 su 5 stelle5/5 (1)
- Rules On Vigilance of Medical Devices PDFDocumento8 pagineRules On Vigilance of Medical Devices PDFsks27974Nessuna valutazione finora
- Govt GazzetteDocumento27 pagineGovt GazzetteMuntana TewpaingamNessuna valutazione finora
- Schedule M of Drug and Cosmetic ActDocumento83 pagineSchedule M of Drug and Cosmetic Actnishantu_2255705@gmail.comNessuna valutazione finora
- MDD Articles and AnnexesDocumento13 pagineMDD Articles and AnnexestalhasherwaniNessuna valutazione finora
- Sur g0001 Guide To Field Safety Corrective Actions For Medical Devices and in Vitro Diagnostic Medical Devices v5Documento7 pagineSur g0001 Guide To Field Safety Corrective Actions For Medical Devices and in Vitro Diagnostic Medical Devices v5Usman AhmadNessuna valutazione finora
- Guide To: Field Safety Corrective Actions For Medical Devices and In-Vitro Diagnostic Medical DevicesDocumento7 pagineGuide To: Field Safety Corrective Actions For Medical Devices and In-Vitro Diagnostic Medical DevicessachinNessuna valutazione finora
- Zakon o Medicinskim-Sredstvima EngleskiDocumento93 pagineZakon o Medicinskim-Sredstvima EngleskiSlaviša ŠimetićNessuna valutazione finora
- Pharmacovigilance Directive English 2020Documento26 paginePharmacovigilance Directive English 2020Zelalem KetemaNessuna valutazione finora
- Directiva 90 385 EecDocumento35 pagineDirectiva 90 385 EecDebreteni FlorinNessuna valutazione finora
- Medical Product Safety and RegulationDocumento77 pagineMedical Product Safety and Regulationreycardo100% (1)
- Decree 98 2021 1Documento34 pagineDecree 98 2021 1Dân Vùng BiênNessuna valutazione finora
- GHTF Sg2 FD 99 7 Reporting Guidance 990629Documento11 pagineGHTF Sg2 FD 99 7 Reporting Guidance 990629Krishanarju VenkatesanNessuna valutazione finora
- Guideline For Classification of in Vitro Diagnostic Medical Devices - EFDADocumento14 pagineGuideline For Classification of in Vitro Diagnostic Medical Devices - EFDAa.razakhajiNessuna valutazione finora
- Medical DeviceDocumento8 pagineMedical DeviceHarshvardhan ChoudharyNessuna valutazione finora
- 93 42 EEC ChecklistDocumento15 pagine93 42 EEC ChecklistdulichsinhthaiNessuna valutazione finora
- Medical Devices Guideline 2017Documento70 pagineMedical Devices Guideline 2017Robert SplinterNessuna valutazione finora
- SfdaDocumento42 pagineSfdaSHERAZNessuna valutazione finora
- Decree - 4725 - 2005 Label p-25Documento34 pagineDecree - 4725 - 2005 Label p-25Manuela BernalNessuna valutazione finora
- Healthcare Client Alert KUWAITDocumento4 pagineHealthcare Client Alert KUWAITRipunjoy GoswamiNessuna valutazione finora
- Sop VigilanceDocumento7 pagineSop VigilanceLal KrishnaNessuna valutazione finora
- Procedure For Adverse Event Reporting-AOC1Documento6 pagineProcedure For Adverse Event Reporting-AOC1Mohamed EzzatNessuna valutazione finora
- phl186 TDocumento19 paginephl186 TCha GabrielNessuna valutazione finora
- 2023-10 SchweizDocumento56 pagine2023-10 SchweizRabel TalpurNessuna valutazione finora
- Sop VigilanceDocumento7 pagineSop VigilanceJane BrownNessuna valutazione finora
- Sop VigilanceDocumento7 pagineSop VigilanceBiolytic LifesciencesNessuna valutazione finora
- Canada MDRDocumento52 pagineCanada MDRMagdalena MichulecNessuna valutazione finora
- GN-10-R1 - Guidance On Medical Device Field Safety Corrective ActionDocumento20 pagineGN-10-R1 - Guidance On Medical Device Field Safety Corrective ActionnormalNessuna valutazione finora
- GN-13-R1.1 Guidance On The Risk Classification of General Medical DevicesDocumento31 pagineGN-13-R1.1 Guidance On The Risk Classification of General Medical DevicesJoresp EspinozaNessuna valutazione finora
- (MDS-G10) Ar, en - 1 LabelingDocumento20 pagine(MDS-G10) Ar, en - 1 LabelingAhmed AlyNessuna valutazione finora
- Guideline - 11 03 2020Documento62 pagineGuideline - 11 03 2020CynthiaNessuna valutazione finora
- Fedlex Data Admin CH Eli CC 2020 552 20220526 en PDF ADocumento58 pagineFedlex Data Admin CH Eli CC 2020 552 20220526 en PDF ASaksham JNessuna valutazione finora
- Team NB PositionPaper Off LabelUse V1 20221005Documento5 pagineTeam NB PositionPaper Off LabelUse V1 20221005Sasha GelfandNessuna valutazione finora
- Eu MDRDocumento10 pagineEu MDRumeshchandra24276Nessuna valutazione finora
- Regulations On Good Clinical Practice For Medical DevicesDocumento16 pagineRegulations On Good Clinical Practice For Medical DevicesRatheesh RaribaNessuna valutazione finora
- Medical Devices Act - M 3 en PDFDocumento42 pagineMedical Devices Act - M 3 en PDFDewa GedeNessuna valutazione finora
- Embedded Sensor Systems in Medical Devices: Requisites and Challenges AheadDocumento28 pagineEmbedded Sensor Systems in Medical Devices: Requisites and Challenges AheadAbdullah Bin MasoodNessuna valutazione finora
- Mandatory Problem ReportingDocumento24 pagineMandatory Problem ReportingTZ LABNessuna valutazione finora
- Annex 4 SOP AMDF SF Reporting v5Documento9 pagineAnnex 4 SOP AMDF SF Reporting v5Xanderz95Nessuna valutazione finora
- Guideline For MD RegisterationDocumento36 pagineGuideline For MD RegisterationIsidoro OlveraNessuna valutazione finora
- Regulatory GuidlineDocumento88 pagineRegulatory GuidlineM Usman KhanNessuna valutazione finora
- Pharmacovigilance RegulationDocumento10 paginePharmacovigilance Regulationjaggwe rogersNessuna valutazione finora
- IVD GuideDocumento23 pagineIVD GuidevolkandemirNessuna valutazione finora
- Adverse EventDocumento5 pagineAdverse EventSarfraz TejaniNessuna valutazione finora
- ADR Reporting - A Guide For ResearchersDocumento6 pagineADR Reporting - A Guide For ResearchersVivek PoojaryNessuna valutazione finora
- SPO Penarikan AlatDocumento2 pagineSPO Penarikan AlatTettanya Iyu Sama AriqahNessuna valutazione finora
- Guideline On Medical Products Special Import PermitDocumento22 pagineGuideline On Medical Products Special Import PermitTarekegnNessuna valutazione finora
- Medical Device RecallDocumento27 pagineMedical Device RecallTZ LABNessuna valutazione finora
- Who Reuse Single UseDocumento13 pagineWho Reuse Single UsenonanoviNessuna valutazione finora
- Software Testing For Medical DevicesDocumento8 pagineSoftware Testing For Medical Devicesandrewd420% (1)
- GD Classification Draft1Documento31 pagineGD Classification Draft1Suresh AnandNessuna valutazione finora
- Medical Devices - Guidance DocumentDocumento22 pagineMedical Devices - Guidance DocumentloireesNessuna valutazione finora
- Regulation For Medical Devices in IndiaDocumento5 pagineRegulation For Medical Devices in IndiaPavan kumar NaikNessuna valutazione finora
- September 2015 ASEAN Medical Device Directive PDFDocumento106 pagineSeptember 2015 ASEAN Medical Device Directive PDFfayakun14Nessuna valutazione finora
- Questions Answers Adverse Event Reporting - enDocumento4 pagineQuestions Answers Adverse Event Reporting - ensijioladejiNessuna valutazione finora
- Ebook For PV Interview PreparationDocumento100 pagineEbook For PV Interview Preparationaishwarya bodkeNessuna valutazione finora
- MEDICALDEVICEguidlinesfor UAEDocumento31 pagineMEDICALDEVICEguidlinesfor UAEjaberjoumana9683100% (1)
- 1-Medical Devices ActDocumento26 pagine1-Medical Devices ActShankar BNessuna valutazione finora
- Decree 35/2005 (VIII. 26.) of The Minister of Health - in EnglishDocumento12 pagineDecree 35/2005 (VIII. 26.) of The Minister of Health - in EnglishEva LorinczNessuna valutazione finora
- Property Income Bill TemplateDocumento4 pagineProperty Income Bill TemplateSlaviša ŠimetićNessuna valutazione finora
- Birth Certificate: Republic of SerbiaDocumento1 paginaBirth Certificate: Republic of SerbiaSlaviša ŠimetićNessuna valutazione finora
- Zakon o Medicinskim-Sredstvima EngleskiDocumento93 pagineZakon o Medicinskim-Sredstvima EngleskiSlaviša ŠimetićNessuna valutazione finora
- Recnik Mesovitih Tehnickih PojmovaDocumento74 pagineRecnik Mesovitih Tehnickih PojmovaSlaviša Šimetić60% (5)
- Express™ XT - VPS Impression MaterialsDocumento6 pagineExpress™ XT - VPS Impression Materials3mEgyptCoordinatorNessuna valutazione finora
- Effectiveness of Locking Compression Plate in Wedge Fracture of Diaphysis of Radius and Ulna in Adults: A Descriptive Case SeriesDocumento23 pagineEffectiveness of Locking Compression Plate in Wedge Fracture of Diaphysis of Radius and Ulna in Adults: A Descriptive Case SeriesRanjit SahNessuna valutazione finora
- Health Unit Coordinator CoursesDocumento13 pagineHealth Unit Coordinator CoursesMan Tue ThaiNessuna valutazione finora
- 2005 Magnetom Flash 1Documento96 pagine2005 Magnetom Flash 1Herick Savione100% (1)
- Hyperemesis Gravidarum Diagnosis and PathogenesisDocumento5 pagineHyperemesis Gravidarum Diagnosis and PathogenesisLaelatun NafillahNessuna valutazione finora
- DjdlkjsaljdljlDocumento18 pagineDjdlkjsaljdljlEricNessuna valutazione finora
- The Code of Ethics For NursesDocumento8 pagineThe Code of Ethics For NursesZulkifli PomalangoNessuna valutazione finora
- Stratification in The Cox Model: Patrick BrehenyDocumento20 pagineStratification in The Cox Model: Patrick BrehenyRaiJúniorNessuna valutazione finora
- Collection and Transport of Histopathology SpecimensDocumento38 pagineCollection and Transport of Histopathology SpecimensOmair Riaz100% (3)
- Ambulatory CareDocumento11 pagineAmbulatory Caremitishahirlekar100% (1)
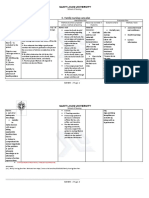
- C. Family Nursing Care Plan: Saint Louis UniversityDocumento2 pagineC. Family Nursing Care Plan: Saint Louis UniversityLEONELLGABRIEL RAGUINDIN0% (1)
- 11 Common Symptoms of CandidaDocumento12 pagine11 Common Symptoms of Candidasantana2013Nessuna valutazione finora
- Head Nursing ToolDocumento26 pagineHead Nursing ToolJeneva L. LauzonNessuna valutazione finora
- Complications-Hypoglycemia Ada PDFDocumento68 pagineComplications-Hypoglycemia Ada PDFjorgefjdNessuna valutazione finora
- Viapath JobDocumento6 pagineViapath JobRebeca UrseNessuna valutazione finora
- 2016 AVA NotesDocumento7 pagine2016 AVA NotesPremNessuna valutazione finora
- Chapter 27 Chest InjuriesDocumento70 pagineChapter 27 Chest Injuriesventus virNessuna valutazione finora
- Arch-En-Design New Delhi / LucknowDocumento12 pagineArch-En-Design New Delhi / LucknowMC EstimationNessuna valutazione finora
- Insomnia: Management of Underlying ProblemsDocumento6 pagineInsomnia: Management of Underlying Problems7OrangesNessuna valutazione finora
- Types of Dosage FormsDocumento92 pagineTypes of Dosage Formsneha_dand1591Nessuna valutazione finora
- Medication History Interview Form Demographic DataDocumento3 pagineMedication History Interview Form Demographic Datakim jongin100% (1)
- ABC of DiabetesDocumento111 pagineABC of DiabetesCandy E Ri ViNessuna valutazione finora
- Deep BretahingDocumento4 pagineDeep Bretahingagustina ika100% (1)
- Lyme DiseaseDocumento133 pagineLyme Diseaseernestval100% (3)
- Filaria PPT - ClassDocumento59 pagineFilaria PPT - ClassGauravMeratwal100% (2)
- P.2 English Exercise TwoDocumento2 pagineP.2 English Exercise TwoAthiyo MartinNessuna valutazione finora
- Module 2Documento2 pagineModule 2Duchess Juliane Jose MirambelNessuna valutazione finora
- Normal GFR in ChildDocumento8 pagineNormal GFR in ChildbobbypambudimdNessuna valutazione finora
- FDARDocumento12 pagineFDARAlyssa Agravante100% (1)
- A Complete Guide to Safety Officer Interview Questions and AnswersDa EverandA Complete Guide to Safety Officer Interview Questions and AnswersValutazione: 4 su 5 stelle4/5 (1)
- Practical Industrial Safety, Risk Assessment and Shutdown SystemsDa EverandPractical Industrial Safety, Risk Assessment and Shutdown SystemsValutazione: 4 su 5 stelle4/5 (11)
- Rules of Thumb for Maintenance and Reliability EngineersDa EverandRules of Thumb for Maintenance and Reliability EngineersValutazione: 4.5 su 5 stelle4.5/5 (12)
- Workbook to Accompany Maintenance & Reliability Best PracticesDa EverandWorkbook to Accompany Maintenance & Reliability Best PracticesValutazione: 3.5 su 5 stelle3.5/5 (3)
- Guidelines for Auditing Process Safety Management SystemsDa EverandGuidelines for Auditing Process Safety Management SystemsNessuna valutazione finora
- Handbook of Fire and Explosion Protection Engineering Principles: for Oil, Gas, Chemical and Related FacilitiesDa EverandHandbook of Fire and Explosion Protection Engineering Principles: for Oil, Gas, Chemical and Related FacilitiesValutazione: 4.5 su 5 stelle4.5/5 (2)
- Healthy Buildings: How Indoor Spaces Drive Performance and ProductivityDa EverandHealthy Buildings: How Indoor Spaces Drive Performance and ProductivityValutazione: 5 su 5 stelle5/5 (2)
- Guidelines for Initiating Events and Independent Protection Layers in Layer of Protection AnalysisDa EverandGuidelines for Initiating Events and Independent Protection Layers in Layer of Protection AnalysisValutazione: 5 su 5 stelle5/5 (1)
- Functional Safety from Scratch: A Practical Guide to Process Industry ApplicationsDa EverandFunctional Safety from Scratch: A Practical Guide to Process Industry ApplicationsNessuna valutazione finora
- Chemical Process Safety: Learning from Case HistoriesDa EverandChemical Process Safety: Learning from Case HistoriesValutazione: 4 su 5 stelle4/5 (14)
- Plutopia: Nuclear Families, Atomic Cities, and the Great Soviet and American Plutonium DisastersDa EverandPlutopia: Nuclear Families, Atomic Cities, and the Great Soviet and American Plutonium DisastersValutazione: 4 su 5 stelle4/5 (32)
- The ISO 45001:2018 Implementation Handbook: Guidance on Building an Occupational Health and Safety Management SystemDa EverandThe ISO 45001:2018 Implementation Handbook: Guidance on Building an Occupational Health and Safety Management SystemNessuna valutazione finora
- The Invisible Rainbow: A History of Electricity and LifeDa EverandThe Invisible Rainbow: A History of Electricity and LifeValutazione: 4.5 su 5 stelle4.5/5 (21)
- Tensor Technology Guide: Tensor Ring Benefits and UsesDa EverandTensor Technology Guide: Tensor Ring Benefits and UsesValutazione: 5 su 5 stelle5/5 (2)
- Nutritional and Therapeutic Interventions for Diabetes and Metabolic SyndromeDa EverandNutritional and Therapeutic Interventions for Diabetes and Metabolic SyndromeNessuna valutazione finora
- A Poison Like No Other: How Microplastics Corrupted Our Planet and Our BodiesDa EverandA Poison Like No Other: How Microplastics Corrupted Our Planet and Our BodiesValutazione: 5 su 5 stelle5/5 (1)
- Environmental and Health and Safety Management: A Guide to ComplianceDa EverandEnvironmental and Health and Safety Management: A Guide to ComplianceValutazione: 4 su 5 stelle4/5 (2)
- General Orders for Security Personnel: A Guide to Maintaining Discipline and ProfessionalismDa EverandGeneral Orders for Security Personnel: A Guide to Maintaining Discipline and ProfessionalismNessuna valutazione finora
- Establishing an occupational health & safety management system based on ISO 45001Da EverandEstablishing an occupational health & safety management system based on ISO 45001Valutazione: 4 su 5 stelle4/5 (5)
- Epidemiology and Demography in Public HealthDa EverandEpidemiology and Demography in Public HealthJaphet KillewoValutazione: 5 su 5 stelle5/5 (1)
- Handbook of Hazardous Chemical PropertiesDa EverandHandbook of Hazardous Chemical PropertiesValutazione: 5 su 5 stelle5/5 (1)
- Safety Fundamentals and Best Practices in Construction IndustryDa EverandSafety Fundamentals and Best Practices in Construction IndustryNessuna valutazione finora