Potrebbero piacerti anche
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- MBLEx Practice Exams PDFDocumento268 pagineMBLEx Practice Exams PDFVani100% (4)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (74)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- Physical AssessmentDocumento19 paginePhysical AssessmentMamerto Q. Flores IIINessuna valutazione finora
- Hamstring Rehabilitation in Elite Track and FieldDocumento13 pagineHamstring Rehabilitation in Elite Track and FieldBarry DoeNessuna valutazione finora
- James Holmes Parents Letter 121914Documento1 paginaJames Holmes Parents Letter 121914USA TODAYNessuna valutazione finora
- Kung Fu Guide 1Documento4 pagineKung Fu Guide 1Bayu Pidada100% (1)
- Laser in Endodontics-A Review ArticleDocumento7 pagineLaser in Endodontics-A Review ArticleKalpanaNessuna valutazione finora
- Jung 2020Documento3 pagineJung 2020KalpanaNessuna valutazione finora
- Lasers in Endodontics-A Review of Literature: P.A.Vasishta, K Anjaneyalu, Vinay Sivaswamy, K AnjaneyaluDocumento7 pagineLasers in Endodontics-A Review of Literature: P.A.Vasishta, K Anjaneyalu, Vinay Sivaswamy, K AnjaneyaluKalpanaNessuna valutazione finora
- Hot Tooth - A Challenge To EndodontistsDocumento5 pagineHot Tooth - A Challenge To EndodontistsKalpanaNessuna valutazione finora
- Recent Diagnostic Aids in Endodontics: Related PapersDocumento6 pagineRecent Diagnostic Aids in Endodontics: Related PapersKalpanaNessuna valutazione finora
- Lasers in Conservative Dentistry: An Overview: Journal of Clinical and Diagnostic Research May 2012Documento5 pagineLasers in Conservative Dentistry: An Overview: Journal of Clinical and Diagnostic Research May 2012KalpanaNessuna valutazione finora
- Head 13811 PDFDocumento14 pagineHead 13811 PDFDiana Putri DamayantiNessuna valutazione finora
- Ippolito 2020Documento2 pagineIppolito 2020KalpanaNessuna valutazione finora
- Ippolito 2020Documento9 pagineIppolito 2020KalpanaNessuna valutazione finora
- Behavioral Considerations and Impact On Personal Protective Equipment Use: Early Lessons From The Coronavirus (COVID-19) PandemicDocumento2 pagineBehavioral Considerations and Impact On Personal Protective Equipment Use: Early Lessons From The Coronavirus (COVID-19) PandemicKalpanaNessuna valutazione finora
- Journal Pre-ProofDocumento26 pagineJournal Pre-ProofKalpanaNessuna valutazione finora
- A Review On Biodentine PDFDocumento11 pagineA Review On Biodentine PDFKyaw MoeNessuna valutazione finora
- Dental Care and Personal Protective Measures For Dentists and Non-Dental Health Care WorkersDocumento5 pagineDental Care and Personal Protective Measures For Dentists and Non-Dental Health Care WorkersKalpanaNessuna valutazione finora
- 10 1016@j Bbi 2020 05 060 PDFDocumento5 pagine10 1016@j Bbi 2020 05 060 PDFBryan Panchana TorresNessuna valutazione finora
- Essay FinalDocumento4 pagineEssay FinalKalpanaNessuna valutazione finora
- Protecting Ourselves During The COVID-19 Pandemic: PerspectivesDocumento2 pagineProtecting Ourselves During The COVID-19 Pandemic: PerspectivesKalpanaNessuna valutazione finora
- PPE or Not PPE - That Is The Question: OpinionDocumento2 paginePPE or Not PPE - That Is The Question: OpinionKalpanaNessuna valutazione finora
- Seminars ListDocumento1 paginaSeminars ListKalpanaNessuna valutazione finora
- Journal Pre-Proof: AJIC: American Journal of Infection ControlDocumento18 pagineJournal Pre-Proof: AJIC: American Journal of Infection ControlKalpanaNessuna valutazione finora
- A Review of Root Fractures Diagnosis Treatment andDocumento10 pagineA Review of Root Fractures Diagnosis Treatment andNonoNessuna valutazione finora
- Local Anesthetics - Introduction and History, Mechanism of Action, Chemical StructureDocumento8 pagineLocal Anesthetics - Introduction and History, Mechanism of Action, Chemical StructureKalpanaNessuna valutazione finora
- MTA Versus Biodentine: Review of Literature With A Comparative AnalysisDocumento5 pagineMTA Versus Biodentine: Review of Literature With A Comparative AnalysisAishwarya Mahesh KumarNessuna valutazione finora
- Date Time Subject: Test Schedule-Second Year PGDocumento1 paginaDate Time Subject: Test Schedule-Second Year PGKalpanaNessuna valutazione finora
- A Review of Root Fractures Diagnosis Treatment andDocumento10 pagineA Review of Root Fractures Diagnosis Treatment andNonoNessuna valutazione finora
- Certificate List and ConferencesDocumento5 pagineCertificate List and ConferencesKalpanaNessuna valutazione finora
- Journal Club Discussion-Kalpana.R: S.No Date Title of Article Students Attended EvaluatorsDocumento1 paginaJournal Club Discussion-Kalpana.R: S.No Date Title of Article Students Attended EvaluatorsKalpanaNessuna valutazione finora
- Date Event Student Topic Staff in Charge: August-September ScheduleDocumento1 paginaDate Event Student Topic Staff in Charge: August-September ScheduleKalpanaNessuna valutazione finora
- Sathyabama Dental College and Hospital Department of Conservative Dentistry and Endodontics Evaluation of Journal Review PresentationsDocumento1 paginaSathyabama Dental College and Hospital Department of Conservative Dentistry and Endodontics Evaluation of Journal Review PresentationsKalpanaNessuna valutazione finora
- Belur Math and CharminarDocumento2 pagineBelur Math and CharminarKalpanaNessuna valutazione finora
- Seminars KalpanaDocumento1 paginaSeminars KalpanaKalpanaNessuna valutazione finora
- Deck and Pool Tips For A Safe Summer, Building Safety Month: Week 3Documento2 pagineDeck and Pool Tips For A Safe Summer, Building Safety Month: Week 3Michigan NewsNessuna valutazione finora
- Nidome No Yuusha Chapter 1 - Chapter 30Documento337 pagineNidome No Yuusha Chapter 1 - Chapter 30Yanina MonasterioNessuna valutazione finora
- Virtual Shoulder and Knee ExaminationDocumento10 pagineVirtual Shoulder and Knee ExaminationAdmirNessuna valutazione finora
- AO OTA Fracture and Dislocation ClassificationDocumento10 pagineAO OTA Fracture and Dislocation ClassificationBENEDICTUSNessuna valutazione finora
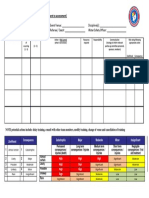
- Event Risk Template in PDFDocumento1 paginaEvent Risk Template in PDFGere TassewNessuna valutazione finora
- Interpretation of Fracturing PressuresDocumento11 pagineInterpretation of Fracturing Pressureslonely1976Nessuna valutazione finora
- Bashir Vs State On 19 March, 1953Documento14 pagineBashir Vs State On 19 March, 1953rahul rasveNessuna valutazione finora
- Cure & CareDocumento10 pagineCure & CareZee ShanNessuna valutazione finora
- Damages On Fatal AccidentDocumento72 pagineDamages On Fatal AccidentMuhammad Adnin Bin Mohd Rasidi100% (1)
- LEICA Sprinter - 50 ManualDocumento26 pagineLEICA Sprinter - 50 ManualGiurca EugenNessuna valutazione finora
- 2015 Physical Injury Part 2Documento8 pagine2015 Physical Injury Part 2Geraldine Marie SalvoNessuna valutazione finora
- Trauma Tulang Belakang-Ppgd - Dr. YoyosDocumento57 pagineTrauma Tulang Belakang-Ppgd - Dr. YoyoszaroziNessuna valutazione finora
- Sinopec Northen Construction Camp - Tilenga Job Hazard Analysis (Jha)Documento3 pagineSinopec Northen Construction Camp - Tilenga Job Hazard Analysis (Jha)Nora Afzam Abd WahabNessuna valutazione finora
- CHUCK PALAHNIUK - American Goth (An Interview With Marilyn Manson)Documento6 pagineCHUCK PALAHNIUK - American Goth (An Interview With Marilyn Manson)Rakendra Nikolas HanakoulasNessuna valutazione finora
- DatasheetDocumento5 pagineDatasheetPradeep KumarNessuna valutazione finora
- HarambeDocumento7 pagineHarambeapi-326395776Nessuna valutazione finora
- Risk Assessment/Management Form: Risk Assessment-Erection of Roof Girder and BeamDocumento3 pagineRisk Assessment/Management Form: Risk Assessment-Erection of Roof Girder and BeamJack PNessuna valutazione finora
- Working With Hammertoes: The Foot (PT I) (Myofascial Techniques)Documento4 pagineWorking With Hammertoes: The Foot (PT I) (Myofascial Techniques)Advanced-Trainings.com100% (5)
- Little Keep, Dorchester, DorsetDocumento86 pagineLittle Keep, Dorchester, DorsetWessex Archaeology100% (1)
- White Bread Competition by Jo Ann Yolanda HernandezDocumento210 pagineWhite Bread Competition by Jo Ann Yolanda HernandezArte Público PressNessuna valutazione finora
- Back Attacks Enter The System - FlowChart 1.2 2Documento1 paginaBack Attacks Enter The System - FlowChart 1.2 2Kellar Carnes0% (1)
- Postoperative Peritoneal Adhesions in Adults and Their Prevention - UpToDateDocumento17 paginePostoperative Peritoneal Adhesions in Adults and Their Prevention - UpToDateDesak PramestiNessuna valutazione finora
- Easy Guide To TensDocumento31 pagineEasy Guide To Tensmastahype100% (7)
- Post-Operative Complications of Craniotomy and CraniectomyDocumento9 paginePost-Operative Complications of Craniotomy and CraniectomyLusy Octavia SaputriNessuna valutazione finora
- Diabetic Foot UlcerDocumento46 pagineDiabetic Foot UlcerNeermaladevi ParamasivamNessuna valutazione finora