Potrebbero piacerti anche
- Instructions: Certification of Health Care Provider: Family and Medical Leave ActDocumento5 pagineInstructions: Certification of Health Care Provider: Family and Medical Leave ActMichelleNessuna valutazione finora
- Request To Postpone Certification Direct 1585343446169 PDFDocumento3 pagineRequest To Postpone Certification Direct 1585343446169 PDFMelvin Fernando Peralta SuazoNessuna valutazione finora
- U.S. Department of Labor Wage and Hour Division Certification of Health Care Provider For Employee's Serious Health Condition Under The Family and Medical Leave ActDocumento4 pagineU.S. Department of Labor Wage and Hour Division Certification of Health Care Provider For Employee's Serious Health Condition Under The Family and Medical Leave Actstawberry shortcakeNessuna valutazione finora
- Family and Medical LeaveDocumento5 pagineFamily and Medical LeaveGeorge RizkNessuna valutazione finora
- Sedgwick Logo - Certification of Health Care Provider For Family Member's Serious Health Condition (FMLA)Documento4 pagineSedgwick Logo - Certification of Health Care Provider For Family Member's Serious Health Condition (FMLA)teamirNessuna valutazione finora
- Certification Employees Serious Health ConditionDocumento4 pagineCertification Employees Serious Health ConditionAnika OkjeNessuna valutazione finora
- Family and Medical Leave PolicyDocumento3 pagineFamily and Medical Leave PolicyUttara KaleNessuna valutazione finora
- Section I - EmployerDocumento4 pagineSection I - EmployerBlanca AgueroNessuna valutazione finora
- What You Need To Know: The Following Dates Are Pending Decision(s)Documento6 pagineWhat You Need To Know: The Following Dates Are Pending Decision(s)Melvin Fernando Peralta SuazoNessuna valutazione finora
- Certification Form.: Please Fax The Completed Forms To The Correct Processing Center. Page 1 of 11Documento11 pagineCertification Form.: Please Fax The Completed Forms To The Correct Processing Center. Page 1 of 11Abi LewisNessuna valutazione finora
- Certification of Your Family Member's Serious Health Condition Form - July - 2023Documento7 pagineCertification of Your Family Member's Serious Health Condition Form - July - 2023Athenagoras SaldivarNessuna valutazione finora
- Certification of Health Care ProviderDocumento4 pagineCertification of Health Care ProviderDavidNessuna valutazione finora
- FAMILY MEMBER Notice of Eligibility Rights & Resp Template (WH-381 Exp 6.2023)Documento4 pagineFAMILY MEMBER Notice of Eligibility Rights & Resp Template (WH-381 Exp 6.2023)Alex DanielNessuna valutazione finora
- Pparx ApplicationsDocumento8 paginePparx ApplicationsJames MullinsNessuna valutazione finora
- 5004o00000P8ZJHAA3 - 1655998080504L080 Decision EOHCSTDDenied EE 04259813Documento15 pagine5004o00000P8ZJHAA3 - 1655998080504L080 Decision EOHCSTDDenied EE 04259813Sarah Ann KhalifaNessuna valutazione finora
- Medical Certification Employee Intermittent Continuous FinalDocumento9 pagineMedical Certification Employee Intermittent Continuous FinalRus RusNessuna valutazione finora
- Medical Certificates and Reports GP ObligationsDocumento12 pagineMedical Certificates and Reports GP ObligationsgovindaNessuna valutazione finora
- PD Medical Certification PD 615ADocumento3 paginePD Medical Certification PD 615AAfif Fauzan MNessuna valutazione finora
- Instructions For Steps in Processing FMLA Leave RequestsDocumento24 pagineInstructions For Steps in Processing FMLA Leave RequestsTexas WatchdogNessuna valutazione finora
- Leave Certification Requirements: Page 1 of 14Documento14 pagineLeave Certification Requirements: Page 1 of 14Anonymous zEf2TWiHgWNessuna valutazione finora
- Department of State Academic Exchanges Participant Medical History and Examination FormDocumento8 pagineDepartment of State Academic Exchanges Participant Medical History and Examination FormNurman HidayatNessuna valutazione finora
- Certification of Qualifying Exigency 1108 MilitaryDocumento4 pagineCertification of Qualifying Exigency 1108 MilitaryvanjaurkeNessuna valutazione finora
- FMLA Leave Notice of Designation, Request, & Approval FMLA - Form #1Documento2 pagineFMLA Leave Notice of Designation, Request, & Approval FMLA - Form #1ahong100Nessuna valutazione finora
- (IL) FMLA Certification Form Employee Condition Beatriz RuizDocumento5 pagine(IL) FMLA Certification Form Employee Condition Beatriz RuizBeatriz RuizNessuna valutazione finora
- Documentation for Skilled Nursing & Long-Term Care: A Guide for Occupational TherapistsDa EverandDocumentation for Skilled Nursing & Long-Term Care: A Guide for Occupational TherapistsNessuna valutazione finora
- FMLA QuestionsDocumento4 pagineFMLA Questionsahong100Nessuna valutazione finora
- SSS Form CLD-9NDocumento2 pagineSSS Form CLD-9NCat LedesmaNessuna valutazione finora
- Curbing Abuse of Intermittent FMLA LeaveDocumento4 pagineCurbing Abuse of Intermittent FMLA LeavehospitalitylawyerNessuna valutazione finora
- Philhealth cf4Documento6 paginePhilhealth cf4Jose AcuinNessuna valutazione finora
- Coca Cola Bottlers Phils. Inc. Vs Dr. Dean N. ClimacoDocumento7 pagineCoca Cola Bottlers Phils. Inc. Vs Dr. Dean N. ClimacoRuby Sedilles ZamoraNessuna valutazione finora
- Medical Certificate To Be Filled by DoctorDocumento3 pagineMedical Certificate To Be Filled by DoctorPsychology TodayNessuna valutazione finora
- Certification Vaccination EmployeesDocumento2 pagineCertification Vaccination EmployeesMediafax.roNessuna valutazione finora
- Sss 02Documento2 pagineSss 02June CruzNessuna valutazione finora
- Fmla-Certification Employees Serious Health Condition 0Documento3 pagineFmla-Certification Employees Serious Health Condition 076xzv4kk5vNessuna valutazione finora
- Cross-Training: The Medical Assistant WorkbookDa EverandCross-Training: The Medical Assistant WorkbookNessuna valutazione finora
- Coca Cola V ClimacoDocumento12 pagineCoca Cola V ClimacoAstina85Nessuna valutazione finora
- Asking-for-FMLA DocumentationDocumento2 pagineAsking-for-FMLA DocumentationnomadinNessuna valutazione finora
- Leave Form Digital v. 2Documento1 paginaLeave Form Digital v. 2Dominic.ManalotoNessuna valutazione finora
- Extension Request LetterpacketDocumento6 pagineExtension Request LetterpacketSherif AhmedNessuna valutazione finora
- Nurse Practitioner Sample ContractDocumento8 pagineNurse Practitioner Sample ContractKassandra RamosNessuna valutazione finora
- Coca Cola Bottlers v. Climaco, G.R. No. 146881february 5, 2007Documento7 pagineCoca Cola Bottlers v. Climaco, G.R. No. 146881february 5, 2007Judel MatiasNessuna valutazione finora
- Medical CertificateDocumento4 pagineMedical CertificateTullimelli AmulyaNessuna valutazione finora
- Medical CertificationDocumento4 pagineMedical CertificationranggadrNessuna valutazione finora
- Health CareDocumento1 paginaHealth CareMikeNessuna valutazione finora
- On The WHD Website at WWW - Dol.gov/agencies/whd/fmlaDocumento4 pagineOn The WHD Website at WWW - Dol.gov/agencies/whd/fmlaknackkayNessuna valutazione finora
- Emergency Sick PayDocumento6 pagineEmergency Sick PayJenNessuna valutazione finora
- Family and Illness LeaveDocumento3 pagineFamily and Illness Leaveshiraz76Nessuna valutazione finora
- Disability Support Pension Claim FormsDocumento11 pagineDisability Support Pension Claim Formscurtisbrown89Nessuna valutazione finora
- COVID RTW Form (CAN)Documento3 pagineCOVID RTW Form (CAN)A. MuyepaNessuna valutazione finora
- FML FormDocumento1 paginaFML Formapi-350774652Nessuna valutazione finora
- FMLA Revised 12-09Documento5 pagineFMLA Revised 12-09Jennifer RobertsNessuna valutazione finora
- FmlaenDocumento1 paginaFmlaenManzarie SinghNessuna valutazione finora
- Under The Family and Medical Leave Act: Employee Rights and ResponsibilitiesDocumento1 paginaUnder The Family and Medical Leave Act: Employee Rights and ResponsibilitiesEnus BenjaminNessuna valutazione finora
- GW Hospital MOU & Observer Health Information FormDocumento2 pagineGW Hospital MOU & Observer Health Information Formengel0321hotmail.comNessuna valutazione finora
- Inform ConsentDocumento9 pagineInform ConsentMeta Bachtiar100% (1)
- Lesley Fugon FMLA Eligbility NoticeDocumento4 pagineLesley Fugon FMLA Eligbility Noticebessy cedilloNessuna valutazione finora
- DEBATEDocumento4 pagineDEBATEMirasol BaykingNessuna valutazione finora
- A Guide for Medical Case Managers: Stop Loss Insurance for Medical ProfessionalsDa EverandA Guide for Medical Case Managers: Stop Loss Insurance for Medical ProfessionalsNessuna valutazione finora
- Newman's Medical Billing and Coding Technicians Study GuideDa EverandNewman's Medical Billing and Coding Technicians Study GuideNessuna valutazione finora
- Newman's Billing and Coding Technicians Study GuideDa EverandNewman's Billing and Coding Technicians Study GuideValutazione: 4.5 su 5 stelle4.5/5 (2)
- Danh Sach Khach Hang VIP Diamond PlazaDocumento9 pagineDanh Sach Khach Hang VIP Diamond PlazaHiệu chuẩn Hiệu chuẩnNessuna valutazione finora
- Concrete For Water StructureDocumento22 pagineConcrete For Water StructureIntan MadiaaNessuna valutazione finora
- Review of Accounting Process 1Documento2 pagineReview of Accounting Process 1Stacy SmithNessuna valutazione finora
- ArpitResumeISM PDFDocumento1 paginaArpitResumeISM PDFchethan rNessuna valutazione finora
- Sales Manager Latin AmericaDocumento3 pagineSales Manager Latin Americaapi-76934736Nessuna valutazione finora
- Caso Kola RealDocumento17 pagineCaso Kola RealEvelyn Dayhanna Escobar PalomequeNessuna valutazione finora
- LICDocumento82 pagineLICTinu Burmi Anand100% (2)
- Syed Hamid Kazmi - CVDocumento2 pagineSyed Hamid Kazmi - CVHamid KazmiNessuna valutazione finora
- Quantum Hopfield NetworksDocumento83 pagineQuantum Hopfield NetworksSiddharth SharmaNessuna valutazione finora
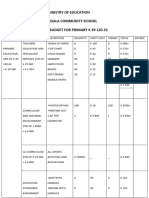
- Ministry of Education Musala SCHDocumento5 pagineMinistry of Education Musala SCHlaonimosesNessuna valutazione finora
- CPE Cisco LTE Datasheet - c78-732744Documento17 pagineCPE Cisco LTE Datasheet - c78-732744abds7Nessuna valutazione finora
- Project Management: Chapter-2Documento26 pagineProject Management: Chapter-2Juned BhavayaNessuna valutazione finora
- Chapter 2 A Guide To Using UnixDocumento53 pagineChapter 2 A Guide To Using UnixAntwon KellyNessuna valutazione finora
- Ethercombing Independent Security EvaluatorsDocumento12 pagineEthercombing Independent Security EvaluatorsangelNessuna valutazione finora
- 7Documento101 pagine7Navindra JaggernauthNessuna valutazione finora
- Types of MemoryDocumento3 pagineTypes of MemoryVenkatareddy Mula0% (1)
- Residential BuildingDocumento5 pagineResidential Buildingkamaldeep singhNessuna valutazione finora
- Petitioner's Response To Show CauseDocumento95 paginePetitioner's Response To Show CauseNeil GillespieNessuna valutazione finora
- (ACYFAR2) Toribio Critique Paper K36.editedDocumento12 pagine(ACYFAR2) Toribio Critique Paper K36.editedHannah Jane ToribioNessuna valutazione finora
- Millionaire Next Door QuestionsDocumento7 pagineMillionaire Next Door Questionsapi-360370073Nessuna valutazione finora
- Marley Product Catalogue Brochure Grease TrapsDocumento1 paginaMarley Product Catalogue Brochure Grease TrapsKushalKallychurnNessuna valutazione finora
- Lemon AidDocumento17 pagineLemon AidJade Anne Mercado BalmesNessuna valutazione finora
- KrauseDocumento3 pagineKrauseVasile CuprianNessuna valutazione finora
- 6 AsianregionalismDocumento32 pagine6 AsianregionalismChandria Ford100% (1)
- EC2 406006 001 EFE 0121 - Controgen Generator Excitation System Description - Rev - ADocumento29 pagineEC2 406006 001 EFE 0121 - Controgen Generator Excitation System Description - Rev - AAnonymous bSpP1m8j0n50% (2)
- FBW Manual-Jan 2012-Revised and Corrected CS2Documento68 pagineFBW Manual-Jan 2012-Revised and Corrected CS2Dinesh CandassamyNessuna valutazione finora
- PartitionDocumento5 paginePartitionKotagiri AravindNessuna valutazione finora
- ELC Work DescriptionDocumento36 pagineELC Work DescriptionHari100% (1)
- Econ 1006 Summary Notes 1Documento24 pagineEcon 1006 Summary Notes 1KulehNessuna valutazione finora