Potrebbero piacerti anche
- Response To States 4.2 Motion in Limine Character of VictimDocumento10 pagineResponse To States 4.2 Motion in Limine Character of VictimLaw of Self DefenseNessuna valutazione finora
- Leptospirosis PDFDocumento48 pagineLeptospirosis PDFTuan HaikalNessuna valutazione finora
- Nursing Care Plan: Fluid Volume Deficit R/T Active Fluid Loss (Increased Urine Output)Documento9 pagineNursing Care Plan: Fluid Volume Deficit R/T Active Fluid Loss (Increased Urine Output)Gayu Patel0% (1)
- Students Sleep During Classes: The Amount of Time VariesDocumento7 pagineStudents Sleep During Classes: The Amount of Time Variesjason_aaNessuna valutazione finora
- Anatomy and PhysiologyDocumento4 pagineAnatomy and PhysiologyBeRnAlieNessuna valutazione finora
- Case AnalysisDocumento25 pagineCase AnalysisGerly LagutingNessuna valutazione finora
- IMCI Chart BookletDocumento66 pagineIMCI Chart Bookletnorwin_033875Nessuna valutazione finora
- Reducing Maternal Mortality: Theories, Models, and PracticeDocumento17 pagineReducing Maternal Mortality: Theories, Models, and PracticeRavi Pamnani100% (2)
- SuctioningDocumento6 pagineSuctioningCriselda Ultado100% (2)
- Nursing Care Plan On HyperthermiaDocumento4 pagineNursing Care Plan On HyperthermiaAleah JayaganNessuna valutazione finora
- DM NCPDocumento2 pagineDM NCPVirgilio Reyes ManuelNessuna valutazione finora
- NCP On DyspneaDocumento5 pagineNCP On DyspneaDizzy BualanNessuna valutazione finora
- NCP PainDocumento2 pagineNCP PainApril_Ivy_Raga_3835Nessuna valutazione finora
- Activity Intolerance and PowerlessnessDocumento3 pagineActivity Intolerance and PowerlessnessLianmuel De GuzmanNessuna valutazione finora
- NCPDocumento2 pagineNCPNichole Audrey SaavedraNessuna valutazione finora
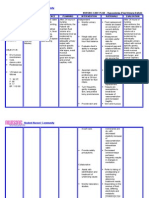
- Cues Diagnosis Background Knowledge Planning Intervention Rationale EvaluationDocumento2 pagineCues Diagnosis Background Knowledge Planning Intervention Rationale EvaluationhaniehaehaeNessuna valutazione finora
- Lapkas HegDocumento1 paginaLapkas HegkurniaNessuna valutazione finora
- NCPDocumento9 pagineNCPHendy Hency YunusNessuna valutazione finora
- NCP FVDDocumento1 paginaNCP FVDsisjing88510Nessuna valutazione finora
- NCPDocumento2 pagineNCPCamille VirayNessuna valutazione finora
- NCP PainDocumento4 pagineNCP PainMark Allison BuenaventuraNessuna valutazione finora
- NCP Knowledge Deficit PDFDocumento2 pagineNCP Knowledge Deficit PDFskylertNessuna valutazione finora
- Assessment Diagnosis Planning Implementation Rationale EvaluationDocumento14 pagineAssessment Diagnosis Planning Implementation Rationale EvaluationJennifer ArdeNessuna valutazione finora
- Drug StudyDocumento24 pagineDrug Studyabulan100% (1)
- Hypovolemia (Fluid Deficit)Documento2 pagineHypovolemia (Fluid Deficit)Lyn Reyes100% (1)
- Assessment Diagnosis Planning Implementation Rationale EvaluationDocumento3 pagineAssessment Diagnosis Planning Implementation Rationale EvaluationHanz AlecNessuna valutazione finora
- Child - Major Burn PDFDocumento3 pagineChild - Major Burn PDFAldith GrahamNessuna valutazione finora
- Nursing Diagnosis Rationale Interventions Rationale EvaluationDocumento2 pagineNursing Diagnosis Rationale Interventions Rationale EvaluationJobie CasipongNessuna valutazione finora
- Nursing Care Plan Impaired Gas ExchangeDocumento1 paginaNursing Care Plan Impaired Gas ExchangeKarylle PetilNessuna valutazione finora
- Ineffective Airway ClearanceDocumento1 paginaIneffective Airway ClearanceChristineAlaNessuna valutazione finora
- Nursing Care Plan Cues Nursing Diagnosis Objective Intervention Rationale Evaluation SubjectiveDocumento2 pagineNursing Care Plan Cues Nursing Diagnosis Objective Intervention Rationale Evaluation SubjectiveFreisanChenMandumotanNessuna valutazione finora
- Care PlanDocumento11 pagineCare PlanCathy GewontNessuna valutazione finora
- NCP Risk InfectionDocumento1 paginaNCP Risk InfectionEni RahmawatiNessuna valutazione finora
- Blood Glucose MonitoringDocumento30 pagineBlood Glucose MonitoringVictoria Castillo TamayoNessuna valutazione finora
- Nephrotic SyndromeDocumento20 pagineNephrotic Syndromeami5687Nessuna valutazione finora
- Case Study RespiDocumento3 pagineCase Study RespiMark Jheran AlvarezNessuna valutazione finora
- Ineffective Airway Clearance CareplanDocumento6 pagineIneffective Airway Clearance CareplanderreshaNessuna valutazione finora
- NCPDocumento6 pagineNCPgenevieve kryzleiNessuna valutazione finora
- Ineffective Airway ClearanceDocumento1 paginaIneffective Airway ClearanceFreisanChenMandumotanNessuna valutazione finora
- Assessment Diagnosis Planning Intervention Rationale EvaluationDocumento4 pagineAssessment Diagnosis Planning Intervention Rationale EvaluationJhoizel VenusNessuna valutazione finora
- Nursing Care Plan: Assessment Diagnosis Inference Goal Intervention Rationale EvaluationDocumento4 pagineNursing Care Plan: Assessment Diagnosis Inference Goal Intervention Rationale EvaluationSugar Capule - ManuelNessuna valutazione finora
- Peritonsillar AbscessDocumento2 paginePeritonsillar AbscessKevin Leo Lucero AragonesNessuna valutazione finora
- NCPDocumento6 pagineNCPNoemi GarciaNessuna valutazione finora
- NCP RiskDocumento2 pagineNCP RiskNorries Jonell CaballarNessuna valutazione finora
- NCP Drug StudyDocumento5 pagineNCP Drug StudyAndrea JoyaNessuna valutazione finora
- MODULE-9-Biotechnology, Genetically Modified Organisms, and Gene TherapyDocumento5 pagineMODULE-9-Biotechnology, Genetically Modified Organisms, and Gene TherapyKerry NuñezNessuna valutazione finora
- Cues Nursing Diagnosis Scientific Rationale Objectives Intervention Rationale Evaluation IndependentDocumento6 pagineCues Nursing Diagnosis Scientific Rationale Objectives Intervention Rationale Evaluation IndependentKasandra Dawn Moquia Beriso100% (1)
- Case Study NCPDocumento4 pagineCase Study NCPKelly OstolNessuna valutazione finora
- NCP ProperDocumento5 pagineNCP ProperRustan FrozenNessuna valutazione finora
- Assessment Diagnosis Scientific Background Planning Intervention Rationale Evaluation Short Term: IndependentDocumento2 pagineAssessment Diagnosis Scientific Background Planning Intervention Rationale Evaluation Short Term: IndependentNE TdrNessuna valutazione finora
- Code Green Introduction Reviewer - RedDocumento4 pagineCode Green Introduction Reviewer - RedJamieNessuna valutazione finora
- RLEFand ECSDocumento3 pagineRLEFand ECSPaul JacksonNessuna valutazione finora
- Fluid Volume Deficit BatuDocumento2 pagineFluid Volume Deficit Batumecz26Nessuna valutazione finora
- Pathophysiology: Risk FactorsDocumento4 paginePathophysiology: Risk FactorsEdson John DemayoNessuna valutazione finora
- Otitis Externa Case StudyDocumento5 pagineOtitis Externa Case StudyGino Al Ballano BorinagaNessuna valutazione finora
- NHPPD Calculating StaffingDocumento3 pagineNHPPD Calculating Staffingodin9360343Nessuna valutazione finora
- Assessment Diagnosis Planning Intervention Rationale Evaluation IndependentDocumento1 paginaAssessment Diagnosis Planning Intervention Rationale Evaluation IndependentAdhaNessuna valutazione finora
- F. Media Preparation and DecontaminationDocumento2 pagineF. Media Preparation and DecontaminationKristin KimNessuna valutazione finora
- Impaired Comfort PruritisDocumento5 pagineImpaired Comfort PruritisBondan PalestinNessuna valutazione finora
- NCP - JaundiceDocumento5 pagineNCP - JaundiceQueen Shine0% (1)
- SeizuresDocumento2 pagineSeizureskaythe08Nessuna valutazione finora
- Date, Shift & Time Assessment Need Nursing Diagnosis Plan Intervention EvaluationDocumento6 pagineDate, Shift & Time Assessment Need Nursing Diagnosis Plan Intervention EvaluationAubrey Unique EvangelistaNessuna valutazione finora
- NCP For LeptospirosisDocumento1 paginaNCP For LeptospirosiskyawNessuna valutazione finora
- NCP HyperthermiaDocumento6 pagineNCP HyperthermiavonjasonbuenafeNessuna valutazione finora
- Hyperthermia HIVDocumento3 pagineHyperthermia HIVam peNessuna valutazione finora
- NCP HyperthermiaDocumento4 pagineNCP HyperthermiaPrincess Alane MorenoNessuna valutazione finora
- PDX AssignmentDocumento8 paginePDX AssignmentAubrey Unique EvangelistaNessuna valutazione finora
- Revised Research ZoomDocumento51 pagineRevised Research ZoomAubrey Unique EvangelistaNessuna valutazione finora
- Health Information Seeking Behavior of Students in College of Medicine: An AssessmentDocumento6 pagineHealth Information Seeking Behavior of Students in College of Medicine: An AssessmentAubrey Unique EvangelistaNessuna valutazione finora
- JMC Paper 1.1Documento5 pagineJMC Paper 1.1Aubrey Unique EvangelistaNessuna valutazione finora
- Final Thesis File (1-5)Documento56 pagineFinal Thesis File (1-5)Aubrey Unique EvangelistaNessuna valutazione finora
- Bioethical Concepts, Principles and TheoriesDocumento8 pagineBioethical Concepts, Principles and TheoriesAubrey Unique EvangelistaNessuna valutazione finora
- COS Porphyria and Bile PigmentsDocumento8 pagineCOS Porphyria and Bile PigmentsAubrey Unique EvangelistaNessuna valutazione finora
- A-G IbmsDocumento4 pagineA-G IbmsAubrey Unique EvangelistaNessuna valutazione finora
- Pathology Case Study - EvangelistaDocumento17 paginePathology Case Study - EvangelistaAubrey Unique EvangelistaNessuna valutazione finora
- Jose Maria Collegecollege of Medicine Section of Biochemistry Clinically-Oriented SessionDocumento3 pagineJose Maria Collegecollege of Medicine Section of Biochemistry Clinically-Oriented SessionAubrey Unique EvangelistaNessuna valutazione finora
- CANE, Quiz, Preliminary Considerations For Operative DentistryDocumento2 pagineCANE, Quiz, Preliminary Considerations For Operative DentistryAubrey Unique EvangelistaNessuna valutazione finora
- Ibms 2 Group Case Presentation DraftDocumento18 pagineIbms 2 Group Case Presentation DraftAubrey Unique EvangelistaNessuna valutazione finora
- Differential DiagnosisDocumento1 paginaDifferential DiagnosisAubrey Unique EvangelistaNessuna valutazione finora
- Aubrey Unique M. Evangelista: Jose Maria College of Medicine FoundationDocumento5 pagineAubrey Unique M. Evangelista: Jose Maria College of Medicine FoundationAubrey Unique EvangelistaNessuna valutazione finora
- Anatomy Midterm NotesDocumento6 pagineAnatomy Midterm NotesAubrey Unique EvangelistaNessuna valutazione finora
- Jose Maria Collegecollege of Medicine Section of Biochemistry Clinically-Oriented SessionDocumento3 pagineJose Maria Collegecollege of Medicine Section of Biochemistry Clinically-Oriented SessionAubrey Unique EvangelistaNessuna valutazione finora
- CHC Agritech TomatoDocumento115 pagineCHC Agritech TomatoAubrey Unique EvangelistaNessuna valutazione finora
- Biochem CosDocumento2 pagineBiochem CosAubrey Unique EvangelistaNessuna valutazione finora
- Jose Maria College of MedicineDocumento50 pagineJose Maria College of MedicineAubrey Unique EvangelistaNessuna valutazione finora
- What Are The Salient Features of The Patient? (10pts)Documento7 pagineWhat Are The Salient Features of The Patient? (10pts)Aubrey Unique EvangelistaNessuna valutazione finora
- Ibms - Case AnalysisDocumento8 pagineIbms - Case AnalysisAubrey Unique EvangelistaNessuna valutazione finora
- Critical AppraisalDocumento4 pagineCritical AppraisalAubrey Unique EvangelistaNessuna valutazione finora
- Critical AppraisalDocumento4 pagineCritical AppraisalAubrey Unique EvangelistaNessuna valutazione finora
- COS Porphyria and Bile PigmentsDocumento8 pagineCOS Porphyria and Bile PigmentsAubrey Unique EvangelistaNessuna valutazione finora
- Mechanism of Pulmonary Ventilation and Management of CovidDocumento11 pagineMechanism of Pulmonary Ventilation and Management of CovidAubrey Unique EvangelistaNessuna valutazione finora
- What Is Primary Health Care and Its Relation To Universal Health Care? As A Medical Student, What Impact Can I Create in Implementing PHC and UHC?Documento2 pagineWhat Is Primary Health Care and Its Relation To Universal Health Care? As A Medical Student, What Impact Can I Create in Implementing PHC and UHC?Aubrey Unique EvangelistaNessuna valutazione finora
- Neuroscience AssignmentDocumento7 pagineNeuroscience AssignmentAubrey Unique EvangelistaNessuna valutazione finora
- Anatomy Essay 1Documento1 paginaAnatomy Essay 1Aubrey Unique EvangelistaNessuna valutazione finora
- Muscle Tissue NotesDocumento11 pagineMuscle Tissue NotesAubrey Unique EvangelistaNessuna valutazione finora
- Components of Your Extensor Compartment of The Wrist: TH THDocumento3 pagineComponents of Your Extensor Compartment of The Wrist: TH THAubrey Unique EvangelistaNessuna valutazione finora
- Antibiotics ResistanceDocumento8 pagineAntibiotics ResistanceboredtarteelNessuna valutazione finora
- Urtikaria Pada Perempuan Usia 39 Tahun: Laporan Kasus: Moh. Wahid Agung, Diany Nurdin, M. SabirDocumento5 pagineUrtikaria Pada Perempuan Usia 39 Tahun: Laporan Kasus: Moh. Wahid Agung, Diany Nurdin, M. SabirZakia AjaNessuna valutazione finora
- Answer Key Ielts 2Documento16 pagineAnswer Key Ielts 2Sovannak OnNessuna valutazione finora
- 1120161049855Documento16 pagine1120161049855Ruchi SharmaNessuna valutazione finora
- JUMPSTART TO SKINNY by Bob Harper: Rule #1Documento8 pagineJUMPSTART TO SKINNY by Bob Harper: Rule #1Random House Publishing GroupNessuna valutazione finora
- Janssen Pharmaceutica NVDocumento63 pagineJanssen Pharmaceutica NVRj jNessuna valutazione finora
- Doctoral Experience Capstone PortfolioDocumento29 pagineDoctoral Experience Capstone Portfolioapi-595108452Nessuna valutazione finora
- Topic ListDocumento6 pagineTopic ListEdwinNessuna valutazione finora
- Position Paper de l'UEFA Sur L'interdiction Du Gazon Synthétique Par l'ECHA 19 Juillet 2019Documento8 paginePosition Paper de l'UEFA Sur L'interdiction Du Gazon Synthétique Par l'ECHA 19 Juillet 2019LeMonde.frNessuna valutazione finora
- Understanding PTSD: Arleen Cerbone Faustina, PH.DDocumento85 pagineUnderstanding PTSD: Arleen Cerbone Faustina, PH.DMuthu SelvanNessuna valutazione finora
- Aravind Eye Care Systems: Providing Total Eye Care To The Rural PopulationDocumento13 pagineAravind Eye Care Systems: Providing Total Eye Care To The Rural PopulationAvik BorahNessuna valutazione finora
- Assoc Between Poor Sleep Quality - Depression Symptoms Among ElderlyDocumento8 pagineAssoc Between Poor Sleep Quality - Depression Symptoms Among ElderlyWindyanissa RecitaNessuna valutazione finora
- 2016 10 12 Members Letter-HHS OCR Organ Transplant DiscriminationDocumento4 pagine2016 10 12 Members Letter-HHS OCR Organ Transplant DiscriminationMike Honda100% (2)
- MiraMate Light Pad InstructionsDocumento8 pagineMiraMate Light Pad InstructionsLaurentMartinonNessuna valutazione finora
- Improving Lives of South Sudanese Communities Through Water and Sanitation: The Story of Salva DutDocumento1 paginaImproving Lives of South Sudanese Communities Through Water and Sanitation: The Story of Salva DutUNICEF South SudanNessuna valutazione finora
- Target Heart Rate Lesson PlanDocumento4 pagineTarget Heart Rate Lesson PlanEryn YeskeNessuna valutazione finora
- KEMH Guidelines On Cardiac Disease in PregnancyDocumento7 pagineKEMH Guidelines On Cardiac Disease in PregnancyAyesha RazaNessuna valutazione finora
- PARS 19 - Slide PDFDocumento23 paginePARS 19 - Slide PDFNorsyaliza Abd Razak100% (1)
- Domestic Violence Cycle of Violence Types of Families-2Documento22 pagineDomestic Violence Cycle of Violence Types of Families-2api-340420872Nessuna valutazione finora
- Typology of Nursing Problems in Family Nursing PracticeDocumento4 pagineTypology of Nursing Problems in Family Nursing PracticeLeah Abdul KabibNessuna valutazione finora
- Chapter 2 Lesson 1Documento3 pagineChapter 2 Lesson 1John Carldel VivoNessuna valutazione finora
- Research Chapter 1 V Final Autosaved 2 1Documento57 pagineResearch Chapter 1 V Final Autosaved 2 1Mirate JessNessuna valutazione finora
- AWB Health Care PDFDocumento54 pagineAWB Health Care PDFimepsystemsNessuna valutazione finora
- Food SafetyDocumento2 pagineFood SafetymacmanueNessuna valutazione finora