Potrebbero piacerti anche
- Respiratory Physiology PDFDocumento84 pagineRespiratory Physiology PDFMichael MoaawadNessuna valutazione finora
- Suggest Fluid Responsiveness: Pulse Pressure Variation (PPV) Cardiac Arrest UtilityDocumento1 paginaSuggest Fluid Responsiveness: Pulse Pressure Variation (PPV) Cardiac Arrest Utilityabobader2100% (1)
- Day 4-01 - Well Performance - 1Documento61 pagineDay 4-01 - Well Performance - 1Haider AshourNessuna valutazione finora
- OkDocumento46 pagineOkHidayati IdaNessuna valutazione finora
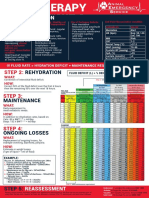
- FLUIDTHERAPY STEP 1: PERFUSIONDocumento1 paginaFLUIDTHERAPY STEP 1: PERFUSIONChristian De Leon100% (1)
- Hemodynamic MonitoringDocumento41 pagineHemodynamic MonitoringSuresh KumarNessuna valutazione finora
- MODULE 3: Engaging in Moderate To Vigorous Physical ActivityDocumento12 pagineMODULE 3: Engaging in Moderate To Vigorous Physical ActivityJohn Erniest Tabungar Austria100% (3)
- PBM Module1 MTP Template 0Documento2 paginePBM Module1 MTP Template 0Daniela Marie RonquilloNessuna valutazione finora
- Cardiac Output FactorsDocumento61 pagineCardiac Output FactorsSyed Ali MoosaNessuna valutazione finora
- Pediatric AnesthesiaDocumento46 paginePediatric AnesthesiaAnnan Agyekum Joshua100% (2)
- Pediatric AnesthesiaDocumento46 paginePediatric AnesthesiaAnnan Agyekum Joshua100% (2)
- Clinical Osteopathic Approaches To Emotions: - Kenneth Lossing DO - AAO Convocation 2016Documento57 pagineClinical Osteopathic Approaches To Emotions: - Kenneth Lossing DO - AAO Convocation 2016Diana SchlittlerNessuna valutazione finora
- Prosper User Course (From Mazhar)Documento33 pagineProsper User Course (From Mazhar)ashraff09Nessuna valutazione finora
- Nursing Care Plan Ovarian CancerDocumento2 pagineNursing Care Plan Ovarian CancerKathleen Dimacali100% (1)
- Graphical Analysis of CO and VR CurvesDocumento29 pagineGraphical Analysis of CO and VR Curvesevamed2027Nessuna valutazione finora
- Regulation of Blood PressureDocumento25 pagineRegulation of Blood PressurePhysiology by Dr RaghuveerNessuna valutazione finora
- Fluid ResponsivenessDocumento42 pagineFluid Responsivenessgwhqvmqks5Nessuna valutazione finora
- Physiology of Hemodynamics-1: Dr. Ghaleb AlmekhlafiDocumento52 paginePhysiology of Hemodynamics-1: Dr. Ghaleb AlmekhlafiGHALEB A. AlmekhlafiNessuna valutazione finora
- Physiology of Hemodynamics-1: Dr. Ghaleb AlmekhlafiDocumento52 paginePhysiology of Hemodynamics-1: Dr. Ghaleb AlmekhlafiGHALEB A. AlmekhlafiNessuna valutazione finora
- Biokimia KardioDocumento98 pagineBiokimia KardioirmaNessuna valutazione finora
- CVS AdaptationDocumento20 pagineCVS AdaptationAlya KamarrudenNessuna valutazione finora
- Blood Pressure Regulation Mechanisms: Short and Long Term Control ExplainedDocumento55 pagineBlood Pressure Regulation Mechanisms: Short and Long Term Control ExplainedDisha SuvarnaNessuna valutazione finora
- PhysiologyDocumento10 paginePhysiologyAmyrah MagajiNessuna valutazione finora
- Final Integrated Labcon Batch 2010Documento32 pagineFinal Integrated Labcon Batch 2010api-3700579Nessuna valutazione finora
- HemodynamicsDocumento2 pagineHemodynamicsbecksterbooNessuna valutazione finora
- Hemodynamics OverviewDocumento10 pagineHemodynamics OverviewAzmeera NagarajuNessuna valutazione finora
- CARDIODocumento10 pagineCARDIOMarcel TabucolNessuna valutazione finora
- Fluids LectureDocumento59 pagineFluids LectureSheryll Almira HilarioNessuna valutazione finora
- Pulmonary Hypertension and EchocardiographyDocumento57 paginePulmonary Hypertension and EchocardiographySiska Istanah Wong SintingNessuna valutazione finora
- Advanced Haemodynamic MonitoringDocumento29 pagineAdvanced Haemodynamic MonitoringParvathy R NairNessuna valutazione finora
- Exphys Paper OutlineDocumento3 pagineExphys Paper OutlineGayle Sixwillfix GreyNessuna valutazione finora
- Fisiologi ShockDocumento31 pagineFisiologi Shockdmandatari7327Nessuna valutazione finora
- Aurigemma Haemodynamics 2021 SlidesDocumento67 pagineAurigemma Haemodynamics 2021 SlidesSajjad HussainNessuna valutazione finora
- Effects of Reverse Trendelenburg on Cardiovascular & Special Circulations During AnesthesiaDocumento5 pagineEffects of Reverse Trendelenburg on Cardiovascular & Special Circulations During AnesthesiaDonkeyManNessuna valutazione finora
- Arterial Pressure RegulationDocumento50 pagineArterial Pressure RegulationareebNessuna valutazione finora
- Renal Physiology: Functions of The KidneyDocumento16 pagineRenal Physiology: Functions of The KidneyUsman Ali Akbar0% (1)
- Physiology of Venous ReturnDocumento42 paginePhysiology of Venous Returncovid kojaNessuna valutazione finora
- Blood PressureDocumento27 pagineBlood PressureSreedeep TejaNessuna valutazione finora
- Central Venous PressureDocumento1 paginaCentral Venous Pressuredian5christiani5malaNessuna valutazione finora
- 10 Pulm HTN Florida - 2017Documento81 pagine10 Pulm HTN Florida - 2017MNessuna valutazione finora
- Coordinated cardiovascular responses to posture, Valsalva maneuver and exerciseDocumento10 pagineCoordinated cardiovascular responses to posture, Valsalva maneuver and exerciseDrbee10Nessuna valutazione finora
- Fluid Responsiveness in Mechanically Ventilated Patients A Review of Indices Used in Intensive CADocumento9 pagineFluid Responsiveness in Mechanically Ventilated Patients A Review of Indices Used in Intensive CAerwanNessuna valutazione finora
- Blood PressureDocumento64 pagineBlood PressureSrishti GoenkaNessuna valutazione finora
- Starling Resistor in Sitting Position in APSF NewsletterDocumento2 pagineStarling Resistor in Sitting Position in APSF NewsletterJennifer PraneviciusNessuna valutazione finora
- 1 VascularDocumento75 pagine1 Vasculareman el saeedNessuna valutazione finora
- Stop BleedingDocumento26 pagineStop BleedingANNENessuna valutazione finora
- HD Problem SolvingDocumento23 pagineHD Problem SolvingGHALEB A. AlmekhlafiNessuna valutazione finora
- 1 HD Problem SolvingDocumento23 pagine1 HD Problem SolvingGHALEB A. AlmekhlafiNessuna valutazione finora
- Blood Flow Images 2Documento35 pagineBlood Flow Images 2Naveen EldoseNessuna valutazione finora
- Cardiac Cycle Stages and Valve MovementsDocumento2 pagineCardiac Cycle Stages and Valve MovementsmeandnewNessuna valutazione finora
- Drugs For Renal PreservationDocumento10 pagineDrugs For Renal PreservationParvathy R NairNessuna valutazione finora
- Normal Hemodynamic Parameters - AdultDocumento3 pagineNormal Hemodynamic Parameters - Adultelangdutamandala12Nessuna valutazione finora
- Terapi Cairan Pada Pasien Shock HemooragikDocumento41 pagineTerapi Cairan Pada Pasien Shock HemooragikNur Syifa FadhilahNessuna valutazione finora
- Hemodynamic Pocket CardDocumento2 pagineHemodynamic Pocket CardTheresa EvilaNessuna valutazione finora
- 5559 NHP Flyer 2Documento1 pagina5559 NHP Flyer 2Kate udeshiNessuna valutazione finora
- Gas Lift - Week 1Documento134 pagineGas Lift - Week 1Made WiraNessuna valutazione finora
- Driller - S Method (Surface)Documento22 pagineDriller - S Method (Surface)JeNggo's YouNgestNessuna valutazione finora
- Assessment of Left AtriumDocumento68 pagineAssessment of Left Atriumadh30Nessuna valutazione finora
- Presentor: DR - Kumar Moderator: DR - VamsidharDocumento71 paginePresentor: DR - Kumar Moderator: DR - VamsidharJayaprakash KuppusamyNessuna valutazione finora
- Basics Hemodynamic Assessment: waveforms and cardiac outputDocumento27 pagineBasics Hemodynamic Assessment: waveforms and cardiac outputTkv UhamkaNessuna valutazione finora
- MD-8 Regulation of Cardiovascular FunctionssDocumento22 pagineMD-8 Regulation of Cardiovascular FunctionssvincenzoNessuna valutazione finora
- Stroke Volume Factors and Effects on Cardiac OutputDocumento2 pagineStroke Volume Factors and Effects on Cardiac OutputJustine Dinice MunozNessuna valutazione finora
- Normal Hemodynamic Parameters - EDWARDSDocumento4 pagineNormal Hemodynamic Parameters - EDWARDSCristell CardenasNessuna valutazione finora
- Basics of Fluid Therapy and PhysiologyDocumento17 pagineBasics of Fluid Therapy and PhysiologyAde GunawanNessuna valutazione finora
- Kuliah Shock Abdurrab UniversityDocumento124 pagineKuliah Shock Abdurrab UniversityVivi AnggrainyNessuna valutazione finora
- Chap+12+CO, VRegul+Fall11 1Documento17 pagineChap+12+CO, VRegul+Fall11 1Drbee100% (1)
- Anesthesia Orthopaedic SurgeryDocumento110 pagineAnesthesia Orthopaedic SurgerychitranganNessuna valutazione finora
- Chronic Obstructive Pulmonary Disease and Anaesthesia: Andrew Lumb Mbbs Frca Claire Biercamp MBCHB FrcaDocumento5 pagineChronic Obstructive Pulmonary Disease and Anaesthesia: Andrew Lumb Mbbs Frca Claire Biercamp MBCHB FrcaHidayati IdaNessuna valutazione finora
- Antibiotics in ICUDocumento63 pagineAntibiotics in ICUsayantanNessuna valutazione finora
- 2015 Anesthesia For Genetic, Metabolic, & Dysmorphic Syndromes of Childhood PDFDocumento965 pagine2015 Anesthesia For Genetic, Metabolic, & Dysmorphic Syndromes of Childhood PDFHidayati IdaNessuna valutazione finora
- Epidural Anesthesia for Labor Pain Relief: Benefits and RisksDocumento12 pagineEpidural Anesthesia for Labor Pain Relief: Benefits and RisksHidayati IdaNessuna valutazione finora
- Post Anesthesia Care Unit (PACU) MahasiswaDocumento10 paginePost Anesthesia Care Unit (PACU) MahasiswaHidayati IdaNessuna valutazione finora
- Ardiology Atient AGE: Bridging AnticoagulationDocumento3 pagineArdiology Atient AGE: Bridging AnticoagulationHidayati IdaNessuna valutazione finora
- Anesthesia services for GI proceduresDocumento6 pagineAnesthesia services for GI proceduresHidayati IdaNessuna valutazione finora
- Epidural Anesthesia for Labor Pain Relief: Benefits and RisksDocumento12 pagineEpidural Anesthesia for Labor Pain Relief: Benefits and RisksHidayati IdaNessuna valutazione finora
- Post Anesthesia Care Unit (PACU) MahasiswaDocumento10 paginePost Anesthesia Care Unit (PACU) MahasiswaHidayati Ida100% (1)
- CVC Insertion OverviewDocumento33 pagineCVC Insertion OverviewHidayati IdaNessuna valutazione finora
- Marik Anes PDFDocumento7 pagineMarik Anes PDFHidayati IdaNessuna valutazione finora
- Marik Anes PDFDocumento7 pagineMarik Anes PDFHidayati IdaNessuna valutazione finora
- R11 YazigiDocumento27 pagineR11 YazigiHidayati IdaNessuna valutazione finora
- Sedation, Pain, and Analgesia: Ricardo R. Jiménez, MDDocumento62 pagineSedation, Pain, and Analgesia: Ricardo R. Jiménez, MDHidayati IdaNessuna valutazione finora
- File 829783Documento20 pagineFile 829783Hidayati IdaNessuna valutazione finora
- Detect AKI Early with Novel BiomarkersDocumento34 pagineDetect AKI Early with Novel BiomarkersSree Nivas ReddyNessuna valutazione finora
- Sedation, Pain, and Analgesia: Ricardo R. Jiménez, MDDocumento62 pagineSedation, Pain, and Analgesia: Ricardo R. Jiménez, MDHidayati IdaNessuna valutazione finora
- R11 YazigiDocumento27 pagineR11 YazigiHidayati IdaNessuna valutazione finora
- AkiDocumento16 pagineAkichris_arc90Nessuna valutazione finora
- Pi Is 0007091217432090Documento2 paginePi Is 0007091217432090Hidayati IdaNessuna valutazione finora
- OkDocumento16 pagineOkHidayati IdaNessuna valutazione finora
- Antibiotics in ICUDocumento63 pagineAntibiotics in ICUsayantanNessuna valutazione finora
- Management of Pregnancy With Eisenmenger Syndrome: AnesthesiaDocumento12 pagineManagement of Pregnancy With Eisenmenger Syndrome: AnesthesiawidyamsNessuna valutazione finora
- 2-2018 Target Fluid TherapyDocumento46 pagine2-2018 Target Fluid TherapyHidayati IdaNessuna valutazione finora
- High school drug rehabilitation case studiesDocumento3 pagineHigh school drug rehabilitation case studiesAudrie Allyson GabalesNessuna valutazione finora
- Physio Xtra Slides Color 2021Documento17 paginePhysio Xtra Slides Color 2021teapalmtreeNessuna valutazione finora
- Rotational Exam Surgery StudentDocumento2 pagineRotational Exam Surgery StudentFerdinand TerceroNessuna valutazione finora
- The LungsDocumento6 pagineThe LungsnandaNessuna valutazione finora
- Critical Care Handbook for Non-AnaesthetistsDocumento23 pagineCritical Care Handbook for Non-AnaesthetistsAtikaNessuna valutazione finora
- The Failing Heart-An Engine Out of FuelDocumento12 pagineThe Failing Heart-An Engine Out of FuelJorge Leonardo BedoyaNessuna valutazione finora
- Mark Scheme (Results) January 2022Documento16 pagineMark Scheme (Results) January 2022윤소리Nessuna valutazione finora
- Respiratory Assessment Guide for NursesDocumento12 pagineRespiratory Assessment Guide for NursesDhen Marc0% (1)
- 8.1 - Nervous Impulses - 1Documento8 pagine8.1 - Nervous Impulses - 1jamilNessuna valutazione finora
- Introduction To Endocrinology, Hormones and Their Classification Lecture NO: 2 MbbsDocumento32 pagineIntroduction To Endocrinology, Hormones and Their Classification Lecture NO: 2 MbbsOmaraye JoshuaNessuna valutazione finora
- Respiratory System Is Also One of The Important Systems of The Body Which Provides Oxygen To All TheDocumento1 paginaRespiratory System Is Also One of The Important Systems of The Body Which Provides Oxygen To All Thelucas OmondiNessuna valutazione finora
- Raven Biology of Plants 8th Edition Evert Test BankDocumento13 pagineRaven Biology of Plants 8th Edition Evert Test Bankwilliamvanrqg100% (26)
- Hokkaido University Collection of Scholarly and Academic Papers: HUSCAPDocumento8 pagineHokkaido University Collection of Scholarly and Academic Papers: HUSCAPn4dn4dNessuna valutazione finora
- Life Processes: Multiple Choice QuestionsDocumento9 pagineLife Processes: Multiple Choice QuestionsSaaiNessuna valutazione finora
- Clinical Hemodynamic Correlation in Mitral StenosisDocumento82 pagineClinical Hemodynamic Correlation in Mitral StenosisHristo MateevNessuna valutazione finora
- Pacemakers Cardiac External Invasive Electrodes TransvenousDocumento6 paginePacemakers Cardiac External Invasive Electrodes TransvenousEduardoNessuna valutazione finora
- Nusing Assessment Guide: Kidney Failure (CKD) Area: CCUDocumento15 pagineNusing Assessment Guide: Kidney Failure (CKD) Area: CCUAbbas AwfiNessuna valutazione finora
- Timing Protein Intake Increases Energy Expenditure 24 H After Resistance TrainingDocumento6 pagineTiming Protein Intake Increases Energy Expenditure 24 H After Resistance TrainingAyi Abdul BasithNessuna valutazione finora
- Patient Chart: Chart For Henry Williams Simulation #1Documento7 paginePatient Chart: Chart For Henry Williams Simulation #1Kenzie JordanNessuna valutazione finora
- Chapter 66 2Documento13 pagineChapter 66 2isapatrick8126100% (2)
- Cardiorespiratory Endurance: in This Chapter Student Web ResourcesDocumento9 pagineCardiorespiratory Endurance: in This Chapter Student Web ResourcesFRANCO PANUGALINGNessuna valutazione finora
- Surgery: Cholecystectomy: Mariano Marcos State UniversityDocumento23 pagineSurgery: Cholecystectomy: Mariano Marcos State UniversityFrancine JoseNessuna valutazione finora
- C9apstudy GuideDocumento37 pagineC9apstudy GuidejqtdNessuna valutazione finora
- Internal Medicine - Phase 3: Important Legal InformationDocumento19 pagineInternal Medicine - Phase 3: Important Legal InformationClaire YabaNessuna valutazione finora
- TAPVR in Neonate NeoReviews Jan2019Documento3 pagineTAPVR in Neonate NeoReviews Jan2019Sridhar KaushikNessuna valutazione finora
- 4th Q Sci 8 ExamDocumento4 pagine4th Q Sci 8 ExamRuthchel GuillarteNessuna valutazione finora
- Grade 11 Life Sciences Remote Learning Booklet - Term 3 & 4Documento91 pagineGrade 11 Life Sciences Remote Learning Booklet - Term 3 & 4destineemande07Nessuna valutazione finora