Potrebbero piacerti anche
- Schizophrenia Case StudyDocumento14 pagineSchizophrenia Case Studykristinanicole47100% (3)
- Lippincott ProceduresDocumento3 pagineLippincott ProceduresYmon TuallaNessuna valutazione finora
- FormDocumento10 pagineFormjesperdomincilbayauaNessuna valutazione finora
- Disaster Preparedness for Healthcare FacilitiesDa EverandDisaster Preparedness for Healthcare FacilitiesValutazione: 2 su 5 stelle2/5 (3)
- Neonatal ResuscitationDocumento15 pagineNeonatal Resuscitationpriyanka88% (8)
- Disaster Management Guide in 40 CharactersDocumento6 pagineDisaster Management Guide in 40 CharacterssimmyvashishtNessuna valutazione finora
- Nursing Care of Clients in Emergency Situation 2Documento52 pagineNursing Care of Clients in Emergency Situation 2Danica FrancoNessuna valutazione finora
- Emergency Disaster Management GuideDocumento12 pagineEmergency Disaster Management GuideAparna KinginiNessuna valutazione finora
- Lozano Disaster Nursing PDFDocumento21 pagineLozano Disaster Nursing PDFDeva Hiyas100% (1)
- BMC Nursing Evaluation FormDocumento4 pagineBMC Nursing Evaluation FormEmman Acosta DomingcilNessuna valutazione finora
- DPP Unit - VDocumento59 pagineDPP Unit - V153-B RAKSHITHANessuna valutazione finora
- Disaster Risk Management and MitigationDocumento5 pagineDisaster Risk Management and MitigationMarivic DianoNessuna valutazione finora
- Medical-Surgical Nursing: An Integrated Approach, 2E: Nursing Care of The Client: Responding To EmergenciesDocumento25 pagineMedical-Surgical Nursing: An Integrated Approach, 2E: Nursing Care of The Client: Responding To EmergenciesRS Buenavista100% (1)
- Triage Lecture DR F Mesa GaerlanDocumento55 pagineTriage Lecture DR F Mesa Gaerlanapi-19431894100% (1)
- Theatre Nursing: By: Gachuhi WangariDocumento130 pagineTheatre Nursing: By: Gachuhi WangariJonah nyachae100% (1)
- DISASTERDocumento55 pagineDISASTERojiNessuna valutazione finora
- DISASTER ManagementDocumento45 pagineDISASTER ManagementShang Divina EbradaNessuna valutazione finora
- Epidemiology and Public HealthDocumento21 pagineEpidemiology and Public HealthFatima SumabatNessuna valutazione finora
- Disaster ManagementDocumento38 pagineDisaster ManagementKailash Nagar100% (2)
- Communicable DiseasesDocumento20 pagineCommunicable DiseasesKILLUANessuna valutazione finora
- Et IntubateDocumento47 pagineEt IntubatectuagentNessuna valutazione finora
- Provision of A Safe EnvironmentDocumento19 pagineProvision of A Safe EnvironmentKristian Jane de JesusNessuna valutazione finora
- Microbiology Burton's Chapter 16Documento74 pagineMicrobiology Burton's Chapter 16Whenzhie Villaverde PampoNessuna valutazione finora
- Disaster Nursing P1 Learning PlanDocumento5 pagineDisaster Nursing P1 Learning PlanPamela GastalaNessuna valutazione finora
- Procedure Checklist For Applying Hard Cervical CollarDocumento3 pagineProcedure Checklist For Applying Hard Cervical Collarirish felixNessuna valutazione finora
- Perioperative Nursing: Rose Delia P. Ocariza, RN, MANDocumento66 paginePerioperative Nursing: Rose Delia P. Ocariza, RN, MANDeva HiyasNessuna valutazione finora
- Basic Life Support (BLS) and Advanced Cardiac Life Support (ACLS)Documento7 pagineBasic Life Support (BLS) and Advanced Cardiac Life Support (ACLS)Rizki YuliantoNessuna valutazione finora
- Disaster MGMTDocumento72 pagineDisaster MGMTVarinder PalNessuna valutazione finora
- CPR Checklist PDFDocumento2 pagineCPR Checklist PDFSakura SaitoNessuna valutazione finora
- St. Mary's College Nursing Program Teaches Critical Care ConceptsDocumento33 pagineSt. Mary's College Nursing Program Teaches Critical Care ConceptsAlyssa Gaile EspirituNessuna valutazione finora
- Scope and Practice of Emergency With LectureDocumento34 pagineScope and Practice of Emergency With LectureArvie ReyesNessuna valutazione finora
- Pain ManagementDocumento7 paginePain ManagementDenisia HoltNessuna valutazione finora
- Unit - I IntroConcepts of Psychiatric NursingDocumento16 pagineUnit - I IntroConcepts of Psychiatric NursingNarayan K GhorapdeNessuna valutazione finora
- Test Taking Tips For The Nursing Board Exam 1 PDFDocumento4 pagineTest Taking Tips For The Nursing Board Exam 1 PDFRaya MesiasNessuna valutazione finora
- Essential First Aid SkillsDocumento13 pagineEssential First Aid SkillsVian ArccenioNessuna valutazione finora
- Skin Integrity and Wound CareDocumento47 pagineSkin Integrity and Wound CareCHALIE MEQUNessuna valutazione finora
- Disaster Nursing ReviewerDocumento60 pagineDisaster Nursing ReviewerGienelle Susana San Juan FerrerNessuna valutazione finora
- Basic Life SupportDocumento5 pagineBasic Life SupportbuenoevelynNessuna valutazione finora
- Triage and Disaster: Nur Masyeerah Abdul JalilDocumento22 pagineTriage and Disaster: Nur Masyeerah Abdul JalilnavenNessuna valutazione finora
- Host defense mechanisms overviewDocumento7 pagineHost defense mechanisms overviewmyfilesNessuna valutazione finora
- 0 Comments: Disaster PreparednessDocumento18 pagine0 Comments: Disaster PreparednessCharis Paroginog100% (1)
- Communicable DiseasesDocumento24 pagineCommunicable DiseasesJanus de LeonNessuna valutazione finora
- Hospital Emergency PlanDocumento5 pagineHospital Emergency PlandedefreddyNessuna valutazione finora
- SnakebiteDocumento4 pagineSnakebiteallenininiNessuna valutazione finora
- Emergency Trauma CareDocumento49 pagineEmergency Trauma Careandrei neagNessuna valutazione finora
- Management of Patients With Burn InjuryDocumento36 pagineManagement of Patients With Burn Injuryraghad awwad100% (1)
- Guidelines For Preoperative Patient Skin AntisepsisDocumento49 pagineGuidelines For Preoperative Patient Skin Antisepsisluckyswiss7776848Nessuna valutazione finora
- Emergency Severity Index Guidelines For Triage CeuDocumento71 pagineEmergency Severity Index Guidelines For Triage Ceuani mulyani100% (1)
- TRIAGEDocumento55 pagineTRIAGELaveena AswaleNessuna valutazione finora
- Rubric For Collaborative Lesson Plan Writing: Score 4 (Exemplary) 3 (Proficient) 2 (Developing) 1 (Needs Improvement)Documento3 pagineRubric For Collaborative Lesson Plan Writing: Score 4 (Exemplary) 3 (Proficient) 2 (Developing) 1 (Needs Improvement)Nikki CrystelNessuna valutazione finora
- Approach To BSN CurriculumDocumento14 pagineApproach To BSN CurriculumCheska DillupacNessuna valutazione finora
- SnakebiteDocumento54 pagineSnakebiteDimas Satrio BNessuna valutazione finora
- Anti InfectivesDocumento126 pagineAnti Infectiveseunice lachicaNessuna valutazione finora
- Respiratory Emergencies2Documento47 pagineRespiratory Emergencies2yeniNessuna valutazione finora
- Emergency Rooms (ER) : Presented By: AdamDocumento6 pagineEmergency Rooms (ER) : Presented By: AdamSulemanNessuna valutazione finora
- CPR Critical SkillsDocumento2 pagineCPR Critical SkillsErickson TiuNessuna valutazione finora
- Professionalism: Workplace EthicsDocumento45 pagineProfessionalism: Workplace Ethicsprecious maningasNessuna valutazione finora
- Emergency and Disaster NursingDocumento8 pagineEmergency and Disaster NursingJOvie RectinNessuna valutazione finora
- Lecture 2 Microbial Growth and NutritionDocumento35 pagineLecture 2 Microbial Growth and NutritionMaria Florida ClementeNessuna valutazione finora
- Patient AssessmentDocumento5 paginePatient AssessmentMary Janine Joy RimanoNessuna valutazione finora
- Disaster ManagementDocumento12 pagineDisaster ManagementharpreetNessuna valutazione finora
- Disaster and Emergency ManagementDocumento11 pagineDisaster and Emergency Managementsanket.visputeNessuna valutazione finora
- Getting A Leg Up On ChartingDocumento3 pagineGetting A Leg Up On ChartingTenIs ForMeNessuna valutazione finora
- Focus Charting Example PDFDocumento1 paginaFocus Charting Example PDFRegine Lorenzana Mey-AngNessuna valutazione finora
- Importance of Technology in NursingDocumento6 pagineImportance of Technology in NursingTenIs ForMeNessuna valutazione finora
- Spatial and Temporal Analysis of Dengue Infections in Queensland, Australia Recent Trend and PerspectivesDocumento18 pagineSpatial and Temporal Analysis of Dengue Infections in Queensland, Australia Recent Trend and PerspectivesTenIs ForMeNessuna valutazione finora
- Refining A Self-Assessment of Informatics Competency Scale Using Mokken Scaling AnalysisDocumento9 pagineRefining A Self-Assessment of Informatics Competency Scale Using Mokken Scaling AnalysisTenIs ForMeNessuna valutazione finora
- Content ServerDocumento14 pagineContent ServerTenIs ForMeNessuna valutazione finora
- Nursing Informatics The Intersection of Nursing, Computer, PDFDocumento5 pagineNursing Informatics The Intersection of Nursing, Computer, PDFTenIs ForMeNessuna valutazione finora
- Informatics in The Nursing Curriculum: A National Survey of Nursing Informatics Requirements in Nursing CurriculaDocumento7 pagineInformatics in The Nursing Curriculum: A National Survey of Nursing Informatics Requirements in Nursing CurriculaTenIs ForMeNessuna valutazione finora
- An Emergent Nursing PracticeDocumento6 pagineAn Emergent Nursing PracticeTenIs ForMeNessuna valutazione finora
- The Development and Evaluation of A Nursing Information System For Caring Clinical In-PatientDocumento7 pagineThe Development and Evaluation of A Nursing Information System For Caring Clinical In-PatientTenIs ForMeNessuna valutazione finora
- Importance of Technology in NursingDocumento6 pagineImportance of Technology in NursingTenIs ForMeNessuna valutazione finora
- Developing Nurse Educators' Computer Skills Towards Proficiency in Nursing InformaticsDocumento21 pagineDeveloping Nurse Educators' Computer Skills Towards Proficiency in Nursing InformaticsTenIs ForMeNessuna valutazione finora
- The Shan People's Health Beliefs, KnowledgeDocumento16 pagineThe Shan People's Health Beliefs, KnowledgeTenIs ForMeNessuna valutazione finora
- The Shan People's Health Beliefs, KnowledgeDocumento16 pagineThe Shan People's Health Beliefs, KnowledgeTenIs ForMeNessuna valutazione finora
- Forecasting Dengue Fever in Brazil AnDocumento17 pagineForecasting Dengue Fever in Brazil AnTenIs ForMeNessuna valutazione finora
- Forecasting Dengue Fever in Brazil AnDocumento17 pagineForecasting Dengue Fever in Brazil AnTenIs ForMeNessuna valutazione finora
- Predictive Models For The Medical Diagnosis of Dengue A CaseDocumento9 paginePredictive Models For The Medical Diagnosis of Dengue A CaseTenIs ForMeNessuna valutazione finora
- A1111111111 A1111111111 A1111111111 A1111111111 A1111111111: Author SummaryDocumento14 pagineA1111111111 A1111111111 A1111111111 A1111111111 A1111111111: Author SummaryTenIs ForMeNessuna valutazione finora
- Lessons Learned From DengueDocumento10 pagineLessons Learned From DengueTenIs ForMeNessuna valutazione finora
- A1111111111 A1111111111 A1111111111 A1111111111 A1111111111: Author SummaryDocumento14 pagineA1111111111 A1111111111 A1111111111 A1111111111 A1111111111: Author SummaryTenIs ForMeNessuna valutazione finora
- History of Nursing in The PhilippiinesDocumento2 pagineHistory of Nursing in The Philippiinesmaimytshad5318Nessuna valutazione finora
- Building A Culture of Research Recommended Practices PDFDocumento33 pagineBuilding A Culture of Research Recommended Practices PDFRajeev KamalNessuna valutazione finora
- Focus Charting Review PDFDocumento9 pagineFocus Charting Review PDFTenIs ForMeNessuna valutazione finora
- Importance of Technology in NursingDocumento6 pagineImportance of Technology in NursingTenIs ForMeNessuna valutazione finora
- Focus ChartingDocumento3 pagineFocus ChartingMan GatuankoNessuna valutazione finora
- Nursing Glossary Original FilesDocumento25 pagineNursing Glossary Original FilesTenIs ForMeNessuna valutazione finora
- CHN Concepts CompiledDocumento81 pagineCHN Concepts CompiledTenIs ForMe0% (1)
- Focus Charting Review PDFDocumento9 pagineFocus Charting Review PDFTenIs ForMeNessuna valutazione finora
- Novatech's Robotics Centre Establishes STEM LearningDocumento12 pagineNovatech's Robotics Centre Establishes STEM LearningTenIs ForMeNessuna valutazione finora
- Nursing Foundation Course OutlineDocumento17 pagineNursing Foundation Course OutlineTenIs ForMeNessuna valutazione finora
- Exposure To Early Life Stress and Risk For DepressionDocumento14 pagineExposure To Early Life Stress and Risk For DepressionCarla MesquitaNessuna valutazione finora
- Lesson 2: First Aid Qualities of A Good First Aider: Gentle Observant Resorceful Sympathetic Tactful CheerfulDocumento4 pagineLesson 2: First Aid Qualities of A Good First Aider: Gentle Observant Resorceful Sympathetic Tactful CheerfulDexter BangayanNessuna valutazione finora
- Custom-Made 3d-Printed Face Masks in Case of Pandemic Crisis Situations With A Lack of Commercially Available FFP2/3 MasksDocumento5 pagineCustom-Made 3d-Printed Face Masks in Case of Pandemic Crisis Situations With A Lack of Commercially Available FFP2/3 MasksBryan Panchana TorresNessuna valutazione finora
- World Stroke Day 2019Documento3 pagineWorld Stroke Day 2019GhaniNessuna valutazione finora
- Rehabilitation Services Group6Documento62 pagineRehabilitation Services Group6Garima KwatraNessuna valutazione finora
- Community Healthcare Family Nursing Care Plan Presence of Breeding SitesDocumento2 pagineCommunity Healthcare Family Nursing Care Plan Presence of Breeding SitesAndrea LapuraNessuna valutazione finora
- Pernicious Anemia: Pernicious Anemia Is A Type of Vitamin BDocumento14 paginePernicious Anemia: Pernicious Anemia Is A Type of Vitamin BCorneliu PaschanuNessuna valutazione finora
- Jamie Tobin ResumeDocumento1 paginaJamie Tobin Resumeapi-417102517Nessuna valutazione finora
- Water Borne DiseaseDocumento21 pagineWater Borne DiseaseJassimarSinghWahiNessuna valutazione finora
- Fecal Impaction A Cause For ConcernDocumento7 pagineFecal Impaction A Cause For Concernadkhiatul muslihatinNessuna valutazione finora
- English: Quarter 2 - Module 5Documento7 pagineEnglish: Quarter 2 - Module 5Arellano CheireyNessuna valutazione finora
- Jenis-Jenis AutismeDocumento17 pagineJenis-Jenis AutismeAmir AsrafNessuna valutazione finora
- CLD CaseDocumento12 pagineCLD Casemed.student657Nessuna valutazione finora
- Ilovepdf Merged 2 PDFDocumento307 pagineIlovepdf Merged 2 PDFAhmed ZidanNessuna valutazione finora
- IteraxDocumento2 pagineIteraxianecunar100% (2)
- Laporan GiziDocumento11 pagineLaporan GiziEfrata MadridistaNessuna valutazione finora
- Nurses Notes Soapie Day 2Documento3 pagineNurses Notes Soapie Day 2Sunny Al asadiNessuna valutazione finora
- Mental Health ProgramDocumento33 pagineMental Health ProgramjosephNessuna valutazione finora
- Monasteries Meditation Centres Sri Lanka2013 PDFDocumento23 pagineMonasteries Meditation Centres Sri Lanka2013 PDFeberalejandroNessuna valutazione finora
- PE11_Q4_Module4a_Weeks1and2Documento20 paginePE11_Q4_Module4a_Weeks1and2JOMEL CASTRONessuna valutazione finora
- Oladokun Et Al-2019-Plant PathologyDocumento8 pagineOladokun Et Al-2019-Plant PathologyJim EspinosaNessuna valutazione finora
- Material Downloaded From - 1 / 5Documento5 pagineMaterial Downloaded From - 1 / 5Abhinav ThakurNessuna valutazione finora
- The Lancet NCDI Poverty Commission: Bridging A Gap in Universal Health Coverage For The Poorest BillionDocumento54 pagineThe Lancet NCDI Poverty Commission: Bridging A Gap in Universal Health Coverage For The Poorest BillionMario DavilaNessuna valutazione finora
- Nursing Care Plan-Mam LazoDocumento7 pagineNursing Care Plan-Mam LazoGayLah MomblancoNessuna valutazione finora
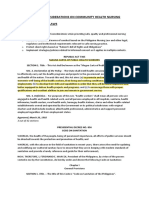
- 0.1 Chapter 7 - Ethical Considerations On Community Health NursingDocumento45 pagine0.1 Chapter 7 - Ethical Considerations On Community Health NursingyounggirldavidNessuna valutazione finora
- Hemoglobinopathies Awareness and Screening SurveyDocumento74 pagineHemoglobinopathies Awareness and Screening SurveyDolly SurelaNessuna valutazione finora
- L30 - FPSC Paper Mill Colony C38/1, Gurdwara Road, Siddheshwar LucknowDocumento4 pagineL30 - FPSC Paper Mill Colony C38/1, Gurdwara Road, Siddheshwar LucknowShamsuddin ShamsNessuna valutazione finora
- Aatcc TM100Documento2 pagineAatcc TM100Kunal ShingalaNessuna valutazione finora