Potrebbero piacerti anche
- Economic Recession 2008Documento6 pagineEconomic Recession 2008Osama AhmedNessuna valutazione finora
- GAD IndexDocumento3 pagineGAD IndexAJAY SHINDENessuna valutazione finora
- Fosroc Chemical Breaker PDFDocumento2 pagineFosroc Chemical Breaker PDFKishore Kumar RajaNessuna valutazione finora
- Inflatable Packers and Grouting Procedures Injection GroutingDocumento7 pagineInflatable Packers and Grouting Procedures Injection GroutingRipe PackersNessuna valutazione finora
- Causes of Global Economic Crisis 2008Documento11 pagineCauses of Global Economic Crisis 2008PriyadarshiSoumyaPrakashNessuna valutazione finora
- Maha Super Housing LoanDocumento4 pagineMaha Super Housing Loansakshishree09Nessuna valutazione finora
- GMLR Eoi PDFDocumento6 pagineGMLR Eoi PDFdheeraj sehgalNessuna valutazione finora
- GMLR EC Report PDFDocumento136 pagineGMLR EC Report PDFprafulvg123Nessuna valutazione finora
- A-165 (13-41) PC - House - For - Incheon - Bridge - Pile-Cap PDFDocumento7 pagineA-165 (13-41) PC - House - For - Incheon - Bridge - Pile-Cap PDFKwon Joon myoungNessuna valutazione finora
- Vetting Sample LetterDocumento1 paginaVetting Sample LetterSHAURYA RANJANNessuna valutazione finora
- Open Saving Account LetterDocumento1 paginaOpen Saving Account LetterSalma AidaNessuna valutazione finora
- Customer Details and Policy Feature Change Request Form Version 2.0 - tcm47-60089Documento2 pagineCustomer Details and Policy Feature Change Request Form Version 2.0 - tcm47-60089UserNED100% (2)
- Loan Application Form: Personal DetailsDocumento8 pagineLoan Application Form: Personal DetailsNihar KNessuna valutazione finora
- Client Information Sheet (For Individual Buyer/S) : Are You An Existing or Previous SBC Account Holder?Documento2 pagineClient Information Sheet (For Individual Buyer/S) : Are You An Existing or Previous SBC Account Holder?Nurhussein RaopanNessuna valutazione finora
- Maturity FormDocumento3 pagineMaturity FormNashitNessuna valutazione finora
- Combined Address Change FormDocumento2 pagineCombined Address Change FormsushikumNessuna valutazione finora
- Used Cars For Sale Offer FormDocumento3 pagineUsed Cars For Sale Offer FormRaymond GabrielNessuna valutazione finora
- Account Transfer FormDocumento2 pagineAccount Transfer FormHemant PandeyNessuna valutazione finora
- Service Request FormDocumento2 pagineService Request FormRS Consultants100% (1)
- JKB PersonaleBankingFormDocumento3 pagineJKB PersonaleBankingFormasoo786Nessuna valutazione finora
- Auto-Offer PSBANKDocumento3 pagineAuto-Offer PSBANKAnna KristinaNessuna valutazione finora
- KYC Form PDFDocumento6 pagineKYC Form PDFKarthik KichuNessuna valutazione finora
- Request For Change in Custo Er Details M: Change/Update Contact Details - Residence/Office/Mobile No./ Email IDDocumento2 pagineRequest For Change in Custo Er Details M: Change/Update Contact Details - Residence/Office/Mobile No./ Email IDPrakash SinghNessuna valutazione finora
- Death Claim Form Under Special Cases (Natural Disaster, Calamities, Bomb Blast) - With 1Documento2 pagineDeath Claim Form Under Special Cases (Natural Disaster, Calamities, Bomb Blast) - With 1raviNessuna valutazione finora
- Change of Address FormDocumento2 pagineChange of Address FormVishal DagarNessuna valutazione finora
- Alfalah Visa Application FormDocumento4 pagineAlfalah Visa Application Formmasoodibrahim100% (1)
- SIB Car Loan Closure DocumentsDocumento3 pagineSIB Car Loan Closure DocumentsRamNessuna valutazione finora
- Personal Account Opening Form: DdmmyyyyDocumento4 paginePersonal Account Opening Form: DdmmyyyyTasneef ChowdhuryNessuna valutazione finora
- Neft Mandateform-1Documento1 paginaNeft Mandateform-1Vishwas ThakurNessuna valutazione finora
- Loan Application Form: XXXXXXX X XXXXXXXXDocumento10 pagineLoan Application Form: XXXXXXX X XXXXXXXXgopikiran6Nessuna valutazione finora
- Customer Cif Amendment Request Form: For Individual / Joint Accounts (Non-Resident Customers Only)Documento1 paginaCustomer Cif Amendment Request Form: For Individual / Joint Accounts (Non-Resident Customers Only)Rizwan.descon DesconNessuna valutazione finora
- Surrender Application FormDocumento1 paginaSurrender Application FormAnanthsai SrikanthNessuna valutazione finora
- Loan Application Form With CollateralDocumento4 pagineLoan Application Form With CollateralIBP Bohol ChapterNessuna valutazione finora
- Application Form For Outward Remittance From Nre AccountDocumento1 paginaApplication Form For Outward Remittance From Nre AccountArjun WadhawanNessuna valutazione finora
- App Form Apna Office IndividualDocumento6 pagineApp Form Apna Office IndividualKadhar AnwarNessuna valutazione finora
- CIB ReportDocumento3 pagineCIB ReportSheikh RonyNessuna valutazione finora
- Application 13009Documento2 pagineApplication 13009frankline nyabutoNessuna valutazione finora
- Agvb KycDocumento19 pagineAgvb KycJeherul BhuyanNessuna valutazione finora
- Accidental Total Permanent Disability - Form - v4Documento4 pagineAccidental Total Permanent Disability - Form - v4raviNessuna valutazione finora
- Accidental Total Permanent Disability - Form - v4Documento4 pagineAccidental Total Permanent Disability - Form - v4raviNessuna valutazione finora
- Delinking FormDocumento2 pagineDelinking Formprofessionalassociates97Nessuna valutazione finora
- Declaration For Re-KYC - Low Risk - IndividualsDocumento2 pagineDeclaration For Re-KYC - Low Risk - IndividualsSubhash Kumar SainNessuna valutazione finora
- Bank Mandate Form PDFDocumento1 paginaBank Mandate Form PDFtechie_10Nessuna valutazione finora
- Customer Information Updation Form (NRI) : NotesDocumento5 pagineCustomer Information Updation Form (NRI) : NotesMoloy GoraiNessuna valutazione finora
- Modfication Form Latest-2Documento2 pagineModfication Form Latest-2navin vargheseNessuna valutazione finora
- Sbi Profile Duplicate Password 2Documento3 pagineSbi Profile Duplicate Password 2An JiNessuna valutazione finora
- Customer Request Form: Dear Sir, Kindly Execute The Following Request/s Which Are Selected BelowDocumento1 paginaCustomer Request Form: Dear Sir, Kindly Execute The Following Request/s Which Are Selected BelowAyyanarNessuna valutazione finora
- NEFT MandateDocumento1 paginaNEFT MandateAyan ParuiNessuna valutazione finora
- Application-Canara Bank FormDocumento4 pagineApplication-Canara Bank Form9589 DIWAKARNessuna valutazione finora
- Updated Customer Service Request Form 2020Documento1 paginaUpdated Customer Service Request Form 2020Maddison YuNessuna valutazione finora
- New Change Request Form - Update - 021219Documento1 paginaNew Change Request Form - Update - 021219Samuel CadelinaNessuna valutazione finora
- Nri 2.5 PDFDocumento2 pagineNri 2.5 PDFGowri A Nair0% (1)
- Account PortabilityDocumento2 pagineAccount PortabilityAshutosh TiwariNessuna valutazione finora
- Customer Risk Profile FormDocumento8 pagineCustomer Risk Profile Formraja duraiNessuna valutazione finora
- Credit ApplicationDocumento3 pagineCredit ApplicationALSIRAT CONTRACTINGNessuna valutazione finora
- Customer Request Form PDFDocumento1 paginaCustomer Request Form PDFMehmood ChawlaNessuna valutazione finora
- FPF400 Request For Transfer of Members Records and Loan DetailsDocumento1 paginaFPF400 Request For Transfer of Members Records and Loan DetailsMiyay AlmirayNessuna valutazione finora
- Premium Prize BondDocumento2 paginePremium Prize BondTariq Mehmood6530% (1)
- Allahabad Bank RtgsDocumento1 paginaAllahabad Bank Rtgsmeraj alamNessuna valutazione finora
- Air Accident Report - 20030312-0 - B744 - 9V-SMTDocumento32 pagineAir Accident Report - 20030312-0 - B744 - 9V-SMTRajiv KumarNessuna valutazione finora
- Regards,: Rubi Arya AVP-Human ResourcesDocumento2 pagineRegards,: Rubi Arya AVP-Human ResourcesRajiv KumarNessuna valutazione finora
- AIS Manual - 1Documento215 pagineAIS Manual - 1Rajiv KumarNessuna valutazione finora
- TDS Authorization Letter PDFDocumento1 paginaTDS Authorization Letter PDFRajiv KumarNessuna valutazione finora
- Group Mediclaim Manual KingfisherDocumento5 pagineGroup Mediclaim Manual KingfisherRajiv KumarNessuna valutazione finora
- I Tried This A Couple of Times, To Reconfirm Unbelievable!Documento1 paginaI Tried This A Couple of Times, To Reconfirm Unbelievable!Rajiv KumarNessuna valutazione finora
- KF - Fuel Policy Oct09Documento1 paginaKF - Fuel Policy Oct09Rajiv KumarNessuna valutazione finora
- Live A LifeDocumento9 pagineLive A LifeRajiv KumarNessuna valutazione finora
- The Titan Book of para CordDocumento14 pagineThe Titan Book of para CordRajiv KumarNessuna valutazione finora
- The Ascent of ManDocumento20 pagineThe Ascent of ManRajiv KumarNessuna valutazione finora
- FIP Mandate FormDocumento2 pagineFIP Mandate FormRajiv KumarNessuna valutazione finora
- Domestic Help Varification Form2Documento3 pagineDomestic Help Varification Form2Rajiv KumarNessuna valutazione finora
- Operating Manual: RegisterDocumento12 pagineOperating Manual: RegisterRajiv KumarNessuna valutazione finora
- Membership Form: (If Different From No. 2)Documento1 paginaMembership Form: (If Different From No. 2)Rajiv KumarNessuna valutazione finora
- Domestic Help Varification Form1Documento3 pagineDomestic Help Varification Form1Rajiv KumarNessuna valutazione finora
- Assign 2assign2Documento4 pagineAssign 2assign2Dawson AdorNessuna valutazione finora
- Bank ReconDocumento18 pagineBank ReconJoefferey Barandino33% (3)
- 3GPP TS 38.304Documento28 pagine3GPP TS 38.304holapaquitoNessuna valutazione finora
- Aurasemi - Timing BU - Main - PresentationDocumento72 pagineAurasemi - Timing BU - Main - PresentationAnindyaSahaNessuna valutazione finora
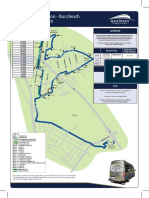
- Marlboro Station - Buccleuch Midibus Service: R10 Per TripDocumento1 paginaMarlboro Station - Buccleuch Midibus Service: R10 Per TripRudy PentyNessuna valutazione finora
- Ippb Finacle Menus and OperationsDocumento35 pagineIppb Finacle Menus and OperationsSathishKumarNessuna valutazione finora
- HDTX - Audit Report 2018 PDFDocumento85 pagineHDTX - Audit Report 2018 PDFFajar PambudiNessuna valutazione finora
- Ict Request LetterDocumento2 pagineIct Request LetterYow200sNessuna valutazione finora
- Fidelity Investments OverviewDocumento3 pagineFidelity Investments OverviewChristian Angelo AyusonNessuna valutazione finora
- Car Loan FinalDocumento21 pagineCar Loan Finalislamkilaniya66100% (1)
- RCRDDocumento2 pagineRCRDjplaurel barangayNessuna valutazione finora
- TM 12-Ch07 Accounting Information System EDITDocumento40 pagineTM 12-Ch07 Accounting Information System EDITLydia PujiellitaNessuna valutazione finora
- Bank Statement09-2020Documento6 pagineBank Statement09-2020Tnt SolutionsNessuna valutazione finora
- Distribution Management Module 2Documento36 pagineDistribution Management Module 2Adam Nicole Sta AnaNessuna valutazione finora
- Quotation: Order Comfirmation Sutek Joint Stock CompanyDocumento1 paginaQuotation: Order Comfirmation Sutek Joint Stock CompanyNguyễn SangNessuna valutazione finora
- Allstate Declaration - 20221110 - 0001Documento4 pagineAllstate Declaration - 20221110 - 0001Shilyn KaufmanNessuna valutazione finora
- L2 - ABFA1173 POA (Lecturer)Documento21 pagineL2 - ABFA1173 POA (Lecturer)Tan SiewsiewNessuna valutazione finora
- MGT 330 FinalDocumento13 pagineMGT 330 FinalKANIZ FATEMANessuna valutazione finora
- Statement of AccountDocumento7 pagineStatement of AccountAdventurous FreakNessuna valutazione finora
- Ducepec Let PhilhealthDocumento1 paginaDucepec Let PhilhealthRaysunNessuna valutazione finora
- The Nature of Electronic Commerce Group 2Documento23 pagineThe Nature of Electronic Commerce Group 2Danica ZabalaNessuna valutazione finora
- Best Buy Strategy Report - FinalDocumento26 pagineBest Buy Strategy Report - FinalcuryaismaraNessuna valutazione finora
- Statement For A/c XXXXXXXXX2500 For The Period 23-Apr-2022 To 22-Apr-2023Documento3 pagineStatement For A/c XXXXXXXXX2500 For The Period 23-Apr-2022 To 22-Apr-2023DANGI TVSNessuna valutazione finora
- Payment Receipt PDFDocumento1 paginaPayment Receipt PDFrajeshNessuna valutazione finora
- Corporate Salary Account Report For HDFC BankDocumento42 pagineCorporate Salary Account Report For HDFC BankShubhranshu SumanNessuna valutazione finora
- A Better Way Health Care SnapshotDocumento3 pagineA Better Way Health Care SnapshotStephen LoiaconiNessuna valutazione finora
- FY-7.6 Student Activity Packet - Google DocsDocumento2 pagineFY-7.6 Student Activity Packet - Google Docstarikhero755Nessuna valutazione finora
- Electronic Ticket Receipt: Netcomp Keishampat Imphal 8974048979 Passenger Contact: 8812940523Documento1 paginaElectronic Ticket Receipt: Netcomp Keishampat Imphal 8974048979 Passenger Contact: 8812940523Surjit SharmaNessuna valutazione finora
- Technical Description of The Mt940 Statement Format For Business 24Documento8 pagineTechnical Description of The Mt940 Statement Format For Business 24tracefalcon007Nessuna valutazione finora
- Executor PHPDocumento2 pagineExecutor PHPosman zainuddinNessuna valutazione finora