Potrebbero piacerti anche
- Dr. Ago Harlim - MikosisDocumento50 pagineDr. Ago Harlim - MikosisBrian Pasa NababanNessuna valutazione finora
- MiliariaDocumento6 pagineMiliariaZyzah HasibuanNessuna valutazione finora
- Fraktur Dan Infeksi TulangDocumento25 pagineFraktur Dan Infeksi TulangAnonymous HAbhRTs2TfNessuna valutazione finora
- CLARA SKIN Who PDFDocumento154 pagineCLARA SKIN Who PDFhasnul ramadhaniNessuna valutazione finora
- Erythrosquamous Diseases / Papulosquamous DiseasesDocumento38 pagineErythrosquamous Diseases / Papulosquamous DiseasesadystiNessuna valutazione finora
- Pityriasis Rosea - Background, Pathophysiology, EtiologyDocumento4 paginePityriasis Rosea - Background, Pathophysiology, EtiologysyahrulroziNessuna valutazione finora
- Pityriasis RoseaDocumento20 paginePityriasis RoseaMendy Herianto100% (1)
- Eritro Papulo Skuamosa 2021Documento47 pagineEritro Papulo Skuamosa 2021Yolanda Agnesia Purba0% (1)
- Diabetes Melitus: Dr. Ihsanil Husna, SPPDDocumento67 pagineDiabetes Melitus: Dr. Ihsanil Husna, SPPDnathan timothyNessuna valutazione finora
- Gnaps EmedicineDocumento13 pagineGnaps Emedicineharyanti lupitaNessuna valutazione finora
- Referat Kandidosis Kutis - Dhira Dan A. Fari-70700120034 Dan 038Documento14 pagineReferat Kandidosis Kutis - Dhira Dan A. Fari-70700120034 Dan 038Ahmad Fari Arief LopaNessuna valutazione finora
- Komplikasi Dan Prognosis Demam TifoidDocumento6 pagineKomplikasi Dan Prognosis Demam TifoidPundi Pandan Putri PinantiNessuna valutazione finora
- Sindrom NefrotikDocumento22 pagineSindrom NefrotikGyta Apriati100% (1)
- Jurding PVDocumento17 pagineJurding PVAnisaAyuningtyasNessuna valutazione finora
- Drug EruptionDocumento46 pagineDrug EruptionSisca ChearzNessuna valutazione finora
- Tinea PedisDocumento35 pagineTinea PedisharzalinaNessuna valutazione finora
- Tatalaksana Pada Luka BakarDocumento55 pagineTatalaksana Pada Luka Bakarmagdalena sriNessuna valutazione finora
- Gangguan Sistem LakrimalDocumento14 pagineGangguan Sistem LakrimalraiNessuna valutazione finora
- Eritrasma 2012Documento17 pagineEritrasma 2012Ammar HasyimNessuna valutazione finora
- Palmoplantar PustulosisDocumento3 paginePalmoplantar PustulosisRobby ZayendraNessuna valutazione finora
- Patogenesis Patofisiologi Gejala KlinikDocumento4 paginePatogenesis Patofisiologi Gejala KlinikAdrian KuswantoNessuna valutazione finora
- Tifoid PerforasiDocumento5 pagineTifoid PerforasiSisca Dwi Agustina0% (1)
- Drug EruptionDocumento46 pagineDrug EruptionSyahDikaNessuna valutazione finora
- Systemic Lupus Erythematosus (SLE) : Pembimbing: Dr. Sondang M Lumban Batu, Sp.ADocumento36 pagineSystemic Lupus Erythematosus (SLE) : Pembimbing: Dr. Sondang M Lumban Batu, Sp.AWinda Oktavia PakpahanNessuna valutazione finora
- Chapter 193:: Herpes Simplex:: Adriana R. Marques & Jeffrey I. CohenDocumento16 pagineChapter 193:: Herpes Simplex:: Adriana R. Marques & Jeffrey I. CohenwadejackNessuna valutazione finora
- KARDIOMYOPATI - Kuliah DR - ErlinaDocumento28 pagineKARDIOMYOPATI - Kuliah DR - ErlinaArif Zulfian MubarokNessuna valutazione finora
- Dermatomikosis JurnalDocumento6 pagineDermatomikosis JurnalNuciana Siti Andrianti100% (1)
- Hepatoma 1Documento37 pagineHepatoma 1Syifa FadyaNessuna valutazione finora
- The Effectiveness of Galactomyces FermentDocumento6 pagineThe Effectiveness of Galactomyces FermentFransiscus Clinton100% (1)
- Kegawatan Respirasi May2016-FkumyDocumento62 pagineKegawatan Respirasi May2016-FkumyAgustina Tri P. DNessuna valutazione finora
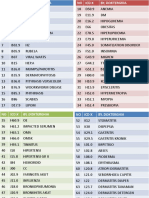
- Icd XDocumento3 pagineIcd XR Ghianesya GantinaNessuna valutazione finora
- A 62 Years Old Woman With Recurrent Depressive Disorder, Episode Now Being With Somatic SymptomsDocumento7 pagineA 62 Years Old Woman With Recurrent Depressive Disorder, Episode Now Being With Somatic SymptomsFauziahNasutionNessuna valutazione finora
- Keratitis PPT 1 SUB ENGLISHDocumento33 pagineKeratitis PPT 1 SUB ENGLISHarif rhNessuna valutazione finora
- Episkleritis N Skleritis EditDocumento12 pagineEpiskleritis N Skleritis EditAnonymous HgX3mN1oNessuna valutazione finora
- 5.soap Chest PainDocumento19 pagine5.soap Chest PainDesiana Kemala SariNessuna valutazione finora
- Krisis AdrenalDocumento18 pagineKrisis AdrenalListya NormalitaNessuna valutazione finora
- Eritroderma - Bolognia 4th EditionDocumento15 pagineEritroderma - Bolognia 4th EditionAisyahNessuna valutazione finora
- Refreshing Obat Muscle Relaxant AnestesiDocumento34 pagineRefreshing Obat Muscle Relaxant AnestesiAnugrah Dwi RiskiNessuna valutazione finora
- LimfadenitisDocumento24 pagineLimfadenitisrahmah ningsihNessuna valutazione finora
- Dandruff PDFDocumento8 pagineDandruff PDFArthur ChietraNessuna valutazione finora
- Referat Kulit KakayDocumento26 pagineReferat Kulit KakayRezky Dwiputra FellanysNessuna valutazione finora
- Drug EruptionDocumento18 pagineDrug EruptionReza AntoniNessuna valutazione finora
- Trichinella Spiralis: A. ClassificationDocumento6 pagineTrichinella Spiralis: A. ClassificationtinasheNessuna valutazione finora
- Mallory Weiss TearDocumento12 pagineMallory Weiss TeararshadmunNessuna valutazione finora
- Jurnal AcneDocumento5 pagineJurnal AcneStacy VaniaNessuna valutazione finora
- SCROFULODERMADocumento25 pagineSCROFULODERMAFaradiba MaricarNessuna valutazione finora
- Filariasis: Dr. Suhaemi, SPPD, FinasimDocumento30 pagineFilariasis: Dr. Suhaemi, SPPD, FinasimErreli K. KhusumawerdanieNessuna valutazione finora
- 194 Surgical Cases PDFDocumento160 pagine194 Surgical Cases PDFkint100% (4)
- K4. Diagnosis Holistik - EngDocumento21 pagineK4. Diagnosis Holistik - EngBevila KorspoilvilNessuna valutazione finora
- Overview of The Mucopolysaccharidoses: RheumatologyDocumento9 pagineOverview of The Mucopolysaccharidoses: RheumatologyLaura Orjuela MateusNessuna valutazione finora
- Leprosy (Morbus Hansen) : Dr. Uun Khusnul Khotimah, SPKKDocumento38 pagineLeprosy (Morbus Hansen) : Dr. Uun Khusnul Khotimah, SPKKagilNessuna valutazione finora
- Tinea CorporisDocumento3 pagineTinea CorporisAndiTriciliaDwiPuspaNessuna valutazione finora
- Alopecia AreataDocumento13 pagineAlopecia AreataAchoonk RamadhanNessuna valutazione finora
- Rheumatic Fever and RHD-SA, HS - FIX PDFDocumento48 pagineRheumatic Fever and RHD-SA, HS - FIX PDFSyadza Rhizky Putri AkhmadNessuna valutazione finora
- Critical Limb IschemiaDocumento11 pagineCritical Limb Ischemianurliah armandNessuna valutazione finora
- Paederus Dermatitis Karthikeyan K, Kumar A - Indian J Dermatol Venereol LeprolDocumento11 paginePaederus Dermatitis Karthikeyan K, Kumar A - Indian J Dermatol Venereol Leprolalmas prawoto100% (1)
- Pityriasis AlbaDocumento7 paginePityriasis AlbaAri Kurniawan100% (1)
- Pityriasis AlbaDocumento6 paginePityriasis AlbaLee Eng SiangNessuna valutazione finora
- Pityriasis Alba: Are You Confident of The Diagnosis?Documento3 paginePityriasis Alba: Are You Confident of The Diagnosis?freska ayu wardhaniNessuna valutazione finora
- Jadotte Pityriasis AlbaDocumento8 pagineJadotte Pityriasis Albapene asoyNessuna valutazione finora
- Etiologies. In: The Open Dermatology Journal. North CarolinaDocumento1 paginaEtiologies. In: The Open Dermatology Journal. North Carolinafreska ayu wardhaniNessuna valutazione finora
- Pityriasis Alba: Are You Confident of The Diagnosis?Documento3 paginePityriasis Alba: Are You Confident of The Diagnosis?freska ayu wardhaniNessuna valutazione finora
- Lumbar SpondylosisDocumento49 pagineLumbar Spondylosisfreska ayu wardhaniNessuna valutazione finora
- Natural History: Changes in Disc Structure With Aging and DegenerationDocumento11 pagineNatural History: Changes in Disc Structure With Aging and Degenerationfreska ayu wardhaniNessuna valutazione finora
- WHO Pocket EmergencyDocumento256 pagineWHO Pocket Emergencypbiluan100% (1)
- EPI201 - 2019 - 00 - Course OverviewDocumento6 pagineEPI201 - 2019 - 00 - Course OverviewJenny WangNessuna valutazione finora
- Impak Krisis Covid19 Terhadap Sektor PertanianDocumento8 pagineImpak Krisis Covid19 Terhadap Sektor PertanianfatinNessuna valutazione finora
- Expel Mucus, Fight Respiratory Irritation With Mighty Mullein & GingerDocumento8 pagineExpel Mucus, Fight Respiratory Irritation With Mighty Mullein & GingerCarl MacCordNessuna valutazione finora
- Master Organism Com Commensals ListsDocumento596 pagineMaster Organism Com Commensals ListslfwaibNessuna valutazione finora
- KKU Scholar III Physical Examination Certificate 2023Documento3 pagineKKU Scholar III Physical Examination Certificate 2023SAMAVIA IRFAN BS Public AdministrationNessuna valutazione finora
- Necrotizing Pneumonitis Caused by Mycoplasma Pneumoniae in Pediatric PatientsDocumento4 pagineNecrotizing Pneumonitis Caused by Mycoplasma Pneumoniae in Pediatric Patientswawa chenNessuna valutazione finora
- Cerebral PalsyDocumento31 pagineCerebral PalsyravannofanizzaNessuna valutazione finora
- PeritonitisDocumento34 paginePeritonitisabrar_zaidiNessuna valutazione finora
- Ja PamphletDocumento2 pagineJa Pamphletapi-460111382Nessuna valutazione finora
- Hepatitis A Treatment in Pune - Kaizen Gastro CareDocumento4 pagineHepatitis A Treatment in Pune - Kaizen Gastro CareKaizen Gastro CareNessuna valutazione finora
- Chap 18 Reading WorksheetDocumento3 pagineChap 18 Reading WorksheetSarahNessuna valutazione finora
- Limberg Flap in Management of Sacrococcygeal Pilonidal Sinus: Our ExperienceDocumento7 pagineLimberg Flap in Management of Sacrococcygeal Pilonidal Sinus: Our ExperienceIJAR JOURNALNessuna valutazione finora
- MalariaDocumento8 pagineMalarianurulzafNessuna valutazione finora
- RabiesDocumento32 pagineRabiesKareen Mae Porras BieneNessuna valutazione finora
- A Story of AcceptanceDocumento3 pagineA Story of AcceptanceArzoo SharmaNessuna valutazione finora
- B5 Communicable Diseases TEST MS F CombinedDocumento3 pagineB5 Communicable Diseases TEST MS F Combinedakio haruNessuna valutazione finora
- Diabetes MellitusDocumento2 pagineDiabetes MellitusElyas MehdarNessuna valutazione finora
- OP DocumenyDocumento10 pagineOP Documenyaliya aslamNessuna valutazione finora
- Pathognomonic Signs of Communicable DiseasesDocumento2 paginePathognomonic Signs of Communicable DiseasesErjohn Vincent Lim0% (1)
- Gutierrez, Winell M. 5 NOVEMBER 2019 BSN Ii-3 Rle-Camantiles Rhu PoliomyelitisDocumento6 pagineGutierrez, Winell M. 5 NOVEMBER 2019 BSN Ii-3 Rle-Camantiles Rhu PoliomyelitisWinell GutierrezNessuna valutazione finora
- Checklist ChildbearingDocumento3 pagineChecklist ChildbearingChristine CornagoNessuna valutazione finora
- Certificate For COVID-19 Vaccination: Beneficiary DetailsDocumento1 paginaCertificate For COVID-19 Vaccination: Beneficiary Detailskonduru revanthNessuna valutazione finora
- Herpes PresentationDocumento10 pagineHerpes PresentationOkafor AugustineNessuna valutazione finora
- CD Respi 30 ADocumento3 pagineCD Respi 30 ANae OrdanozoNessuna valutazione finora
- Scrub Typhus: The Re-Emerging Threat - Thesis SynopsisDocumento17 pagineScrub Typhus: The Re-Emerging Threat - Thesis SynopsisRajesh PadhiNessuna valutazione finora
- CPH Chapter 1Documento5 pagineCPH Chapter 1Claire NicoleNessuna valutazione finora
- Donor ScreeningDocumento39 pagineDonor ScreeningMa. Pe Delaine Mendros100% (1)
- Aaron Morris - The Future Diagnostic Lab ... Inside Your BodyDocumento2 pagineAaron Morris - The Future Diagnostic Lab ... Inside Your BodysoulpixyNessuna valutazione finora
- Dysente RY: ALVAREZ, Ronilyn A. BSN Ii-BDocumento20 pagineDysente RY: ALVAREZ, Ronilyn A. BSN Ii-BRonilyn Mae AlvarezNessuna valutazione finora