Potrebbero piacerti anche
- Appendix 32 - DISBURSEMENT VOUCHERDocumento1 paginaAppendix 32 - DISBURSEMENT VOUCHERPau PerezNessuna valutazione finora
- Annex 5-REGISTER OF CASH RECEIPTS, DEPOSITS AND OTHER RELATED FINANCIALDocumento3 pagineAnnex 5-REGISTER OF CASH RECEIPTS, DEPOSITS AND OTHER RELATED FINANCIALVermon JayNessuna valutazione finora
- Certification of Travel Completed: Appendix 47Documento1 paginaCertification of Travel Completed: Appendix 47ALLAN RONULONessuna valutazione finora
- Handbook FTSK 260Documento1 paginaHandbook FTSK 260adam AlmeraNessuna valutazione finora
- Letter of Transmittal To COADocumento1 paginaLetter of Transmittal To COAKrizza Lorraine Duhaylungsod-Quicoy100% (1)
- Suggested Solutions (RBCPB RSPFCPB - 1st Quarter) PDFDocumento5 pagineSuggested Solutions (RBCPB RSPFCPB - 1st Quarter) PDFJogie BonNessuna valutazione finora
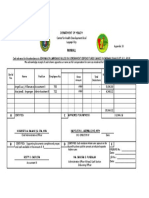
- Appendix 33 - PayrollDocumento1 paginaAppendix 33 - PayrollAngeli Lou Joven Villanueva100% (1)
- Summary of Cash PaymentsDocumento2 pagineSummary of Cash PaymentsSt. Veronica Learning CenterNessuna valutazione finora
- Annex 3 - Rspfcpb-MooeDocumento1 paginaAnnex 3 - Rspfcpb-MooeSK GACAO PALO, LEYTENessuna valutazione finora
- Exercise 6-2 Supplies and Materials 04-01-2019Documento3 pagineExercise 6-2 Supplies and Materials 04-01-2019Arnel ManalastasNessuna valutazione finora
- Annex 11 - LcicDocumento1 paginaAnnex 11 - LcicNestie BryalNessuna valutazione finora
- Bac Reso 2020-011 Recommending Emergency Procurement For Isolation CenterDocumento2 pagineBac Reso 2020-011 Recommending Emergency Procurement For Isolation CenterEduard FerrerNessuna valutazione finora
- Locators SlipDocumento1 paginaLocators SlipGreatDharz DjDiego SolanoyNessuna valutazione finora
- Inspection and Acceptance Report: Annex 16Documento1 paginaInspection and Acceptance Report: Annex 16June Anthony DobleNessuna valutazione finora
- Semestral Report On Status of Submission of Barangay Financial Transaction DocumentsDocumento2 pagineSemestral Report On Status of Submission of Barangay Financial Transaction DocumentsBARANGAY 146Nessuna valutazione finora
- Electronic Payment Payor Enrollment Form: Landbank of The Philippines - BranchDocumento1 paginaElectronic Payment Payor Enrollment Form: Landbank of The Philippines - BranchKilikili East100% (1)
- Registry of Budget, Commitments, Payments and Balances Capital OutlayDocumento1 paginaRegistry of Budget, Commitments, Payments and Balances Capital OutlaySK GACAO PALO, LEYTENessuna valutazione finora
- Sample of Budget PreparationDocumento14 pagineSample of Budget PreparationCasey Del Gallego EnrileNessuna valutazione finora
- BIR FORM 2307 SampleDocumento6 pagineBIR FORM 2307 SampleEasyHear Philippines by NuGen Hearing Devices, Inc.Nessuna valutazione finora
- Purchase Request FormDocumento2 paginePurchase Request Formiramaries30Nessuna valutazione finora
- Appendix 26 - RCD FormDocumento1 paginaAppendix 26 - RCD FormRogie Apolo0% (1)
- Annex E - Certification For Damaged Documents Due To Typhoon OdetteDocumento1 paginaAnnex E - Certification For Damaged Documents Due To Typhoon OdetteDijey Reymundo50% (2)
- Appendix 35 - LR Liquidation ReportDocumento1 paginaAppendix 35 - LR Liquidation ReportEtchel Osiam AvilaNessuna valutazione finora
- SAOR 2015 Additional AOM DO ZDNDocumento9 pagineSAOR 2015 Additional AOM DO ZDNrussel1435Nessuna valutazione finora
- 2021 IGHRS-HRMO-Certificate-of-ComplianceDocumento2 pagine2021 IGHRS-HRMO-Certificate-of-ComplianceRegion PersonnelNessuna valutazione finora
- Payroll 4Documento2 paginePayroll 4Dave LabianoNessuna valutazione finora
- COA - R2016-024 - Deferment of Implementation of COA Circular No. 2015-011 Dated December 1, 2015 - Prescribing The Use of The Manual On Financial Management For BarangaysDocumento1 paginaCOA - R2016-024 - Deferment of Implementation of COA Circular No. 2015-011 Dated December 1, 2015 - Prescribing The Use of The Manual On Financial Management For BarangaysJoseph Paguio100% (1)
- Appendix 34 - CHECKS AND ADVICES TO DEBIT ACCOUNT DISBURSEMENTS RECORDDocumento1 paginaAppendix 34 - CHECKS AND ADVICES TO DEBIT ACCOUNT DISBURSEMENTS RECORDPau PerezNessuna valutazione finora
- Annex 11-Logbook of Checks Issued and CancelledDocumento3 pagineAnnex 11-Logbook of Checks Issued and CancelledVermon JayNessuna valutazione finora
- PAYROLLDocumento1 paginaPAYROLLArchemedes Molina100% (1)
- Appendix 32 - PayrollDocumento2 pagineAppendix 32 - Payrollhehehedontmind meNessuna valutazione finora
- Liquidation ReportDocumento17 pagineLiquidation ReportApril Joy Sumagit HidalgoNessuna valutazione finora
- Sangguniang Kabataan Financial Training and Governance Exemplars For Meaningful Service OrientationDocumento4 pagineSangguniang Kabataan Financial Training and Governance Exemplars For Meaningful Service OrientationOrjen BangonNessuna valutazione finora
- Logbook of Checks Issued and CancelledDocumento2 pagineLogbook of Checks Issued and Cancelledmichael john chavezNessuna valutazione finora
- DV SportswearDocumento1 paginaDV SportswearRenge TañaNessuna valutazione finora
- Property Transfer Report: Entity Name: Fund ClusterDocumento2 pagineProperty Transfer Report: Entity Name: Fund ClusterCatherine BenbanNessuna valutazione finora
- 08 AnnexesDocumento109 pagine08 AnnexesCassieNessuna valutazione finora
- Invitation To Apply and To Bid (SK Office Equipment)Documento3 pagineInvitation To Apply and To Bid (SK Office Equipment)Rene FabriaNessuna valutazione finora
- Report of Check Issued RCIDocumento2 pagineReport of Check Issued RCIArnie Jean AbianNessuna valutazione finora
- Turnover of Money and Property AccountabilitiesDocumento1 paginaTurnover of Money and Property AccountabilitiesDianne Zyra Dela RosaNessuna valutazione finora
- List of Accountable Public Officers For New ApplicantsDocumento1 paginaList of Accountable Public Officers For New ApplicantsRonel Bordios100% (1)
- Travel Expense ReportDocumento2 pagineTravel Expense Reportcamille samsonNessuna valutazione finora
- Preliminary Review of Barangay BudgetDocumento2 paginePreliminary Review of Barangay BudgetRey CorderoNessuna valutazione finora
- Accomplishment Report CbmsDocumento2 pagineAccomplishment Report CbmsMary Grace BlancadNessuna valutazione finora
- Transmittal Letter Blank 2022Documento3 pagineTransmittal Letter Blank 2022Likey PromiseNessuna valutazione finora
- Annex 7 - DV - Clean and GreenDocumento1 paginaAnnex 7 - DV - Clean and GreenWalter IcariNessuna valutazione finora
- SK FormsDocumento49 pagineSK Formsjanila garnicaNessuna valutazione finora
- Disbursement Voucher For BarangayDocumento2 pagineDisbursement Voucher For BarangayJonathan ZusaNessuna valutazione finora
- CertificateDocumento1 paginaCertificateJomar Reuben A. RuecoNessuna valutazione finora
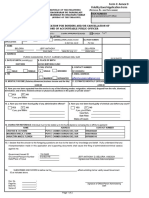
- SK Application Form For FidelityDocumento2 pagineSK Application Form For FidelityJanelkris PlazaNessuna valutazione finora
- Updates For MOOEDocumento245 pagineUpdates For MOOEKristalyn MiguelNessuna valutazione finora
- MC 2018-034 - Updated Guidelines On RATADocumento7 pagineMC 2018-034 - Updated Guidelines On RATAKarla KatigbakNessuna valutazione finora
- Inventory and Inspection Report of Unserviceable PropertyDocumento1 paginaInventory and Inspection Report of Unserviceable PropertyPacita ImpongNessuna valutazione finora
- Apr Form No. 02Documento4 pagineApr Form No. 02Francis Gavin Delos ReyesNessuna valutazione finora
- Disbursement Voucher: LBP AlabelDocumento14 pagineDisbursement Voucher: LBP AlabelJames Hydoe ElanNessuna valutazione finora
- Form ACCEPTANCE & INSPECTION REPORTDocumento2 pagineForm ACCEPTANCE & INSPECTION REPORTLiga ng mga Barangay Catubig Chapter100% (1)
- Travel OrderDocumento1 paginaTravel OrderMarie Antonette Aco Barba100% (1)
- 1.4 BSKE 2023 - Annexes D E and F SANGGUNIANG KABATAAN Inventory and Turnover of SK PFRDs and Money - October 30 RA No. 11935 - February 27 1Documento7 pagine1.4 BSKE 2023 - Annexes D E and F SANGGUNIANG KABATAAN Inventory and Turnover of SK PFRDs and Money - October 30 RA No. 11935 - February 27 1jellyn ayosNessuna valutazione finora
- Obligation Request and Status: Appendix 11Documento2 pagineObligation Request and Status: Appendix 11Rogie ApoloNessuna valutazione finora
- Obligation Request and Status: Dilg Car Entity Name Dilg Car Cos Personnel-Contact TracersDocumento3 pagineObligation Request and Status: Dilg Car Entity Name Dilg Car Cos Personnel-Contact TracersClaudine PuyaoNessuna valutazione finora
- Jagmeet Singh StatementDocumento6 pagineJagmeet Singh StatementBALKAR SINGHNessuna valutazione finora
- Important Reports in SAP FIDocumento42 pagineImportant Reports in SAP FIPallavi100% (1)
- Account Management FormDocumento1 paginaAccount Management FormPaul Mc Ellorey UtterNessuna valutazione finora
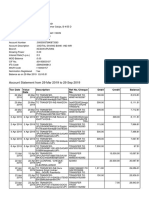
- Lista Tranzactii: Dra Telehoi Andreea RO17BRDE140SV43532111400 RON Andreea TelehoiDocumento6 pagineLista Tranzactii: Dra Telehoi Andreea RO17BRDE140SV43532111400 RON Andreea TelehoiAndreeaNessuna valutazione finora
- BillDocumento1 paginaBillVikas BhosleNessuna valutazione finora
- GST Tax InvoiceDocumento1 paginaGST Tax InvoiceSunnyNessuna valutazione finora
- IciciDocumento8 pagineIcicidhanushNessuna valutazione finora
- MCQs Exam Review Sheet Variant 2Documento8 pagineMCQs Exam Review Sheet Variant 2Majid 1 MubarakNessuna valutazione finora
- e-StatementBRImo 014801118771501 May2023 20230822 020618Documento5 paginee-StatementBRImo 014801118771501 May2023 20230822 020618Puskesmas CamplongNessuna valutazione finora
- State of Market Feb 2008Documento42 pagineState of Market Feb 2008azharaqNessuna valutazione finora
- Ekb OZVi JDKQ 37 Ho GDocumento7 pagineEkb OZVi JDKQ 37 Ho GSahil SalujaNessuna valutazione finora
- SOP ClaimsDocumento9 pagineSOP ClaimsSudalaimuthu KumarNessuna valutazione finora
- Answer Key Fa RemDocumento4 pagineAnswer Key Fa RemMac b IBANEZNessuna valutazione finora
- Hero Housing - Sanction - 09.09.2022 - MCDocumento12 pagineHero Housing - Sanction - 09.09.2022 - MCvishwesheswaran1Nessuna valutazione finora
- Questions Chapter 8Documento19 pagineQuestions Chapter 8SA 10Nessuna valutazione finora
- Chapter 9 Introduction To Data Link LayerDocumento35 pagineChapter 9 Introduction To Data Link LayerFarhan TamzidNessuna valutazione finora
- Trolley Bags - Bags & Luggage - Luggage & Apparel - BestpriceDocumento9 pagineTrolley Bags - Bags & Luggage - Luggage & Apparel - BestpricePrakriti SinghNessuna valutazione finora
- Specialized Fields and Branches of AccountingDocumento2 pagineSpecialized Fields and Branches of AccountingElla Simone100% (2)
- ThesisDocumento6 pagineThesisKell LynoNessuna valutazione finora
- Usaservicestore Com Product Buy Verified Cash App AccountDocumento5 pagineUsaservicestore Com Product Buy Verified Cash App AccountBuy Verified PayPal AccountsNessuna valutazione finora
- MT 103+ Format Specifications: MT 103+ Single Customer Credit TransferDocumento2 pagineMT 103+ Format Specifications: MT 103+ Single Customer Credit Transferme Nader100% (1)
- Application Form 2023Documento8 pagineApplication Form 2023Lovely. RailynnNessuna valutazione finora
- العملات الافتراضية حقيقتها وتكييفها وحكمها الشرعيDocumento24 pagineالعملات الافتراضية حقيقتها وتكييفها وحكمها الشرعيLARBI BENAMARNessuna valutazione finora
- International Premium Outlets - Cuponera 2022Documento7 pagineInternational Premium Outlets - Cuponera 2022Juan P. TestaNessuna valutazione finora
- W.W. Grainger and Mcmaster-Carr: Mro Suppliers: Alejandro Casanueva Hurtado 23611Documento5 pagineW.W. Grainger and Mcmaster-Carr: Mro Suppliers: Alejandro Casanueva Hurtado 23611Hitisha agrawal100% (1)
- PDFDocumento4 paginePDFJunel King VillarNessuna valutazione finora
- Account StatementDocumento22 pagineAccount Statement18 Shivam SharmaNessuna valutazione finora
- Measuring Foreign Exchange Risk and ExposureDocumento9 pagineMeasuring Foreign Exchange Risk and Exposurevenkatesh.s venkatesh.sNessuna valutazione finora
- Investment BankingDocumento62 pagineInvestment Bankingकपिल देव यादवNessuna valutazione finora
- Basic Freeway Segments - F11 PDFDocumento20 pagineBasic Freeway Segments - F11 PDFMichael RantungNessuna valutazione finora