Potrebbero piacerti anche
- Drug Nomenclature Suffixes and PrefixesDocumento6 pagineDrug Nomenclature Suffixes and PrefixesMariaNessuna valutazione finora
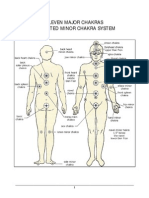
- Eleven Major ChakrasDocumento6 pagineEleven Major Chakrasaynodecam100% (2)
- Renal Physiology Lab ReportDocumento5 pagineRenal Physiology Lab Reportpatricia ankarNessuna valutazione finora
- The Hypothesis and Assumptions of The StudyDocumento12 pagineThe Hypothesis and Assumptions of The StudyMaria Arlene67% (3)
- ACP PocketbookDocumento91 pagineACP PocketbookjamesbeaudoinNessuna valutazione finora
- Nervous System Diseases and DisordersDocumento88 pagineNervous System Diseases and DisordersJape GarridoNessuna valutazione finora
- Circulatory SystemDocumento2 pagineCirculatory SystemcatchivanNessuna valutazione finora
- Resuscitation Pharmacology: Dr. Beny Hartono, SPJP, FihaDocumento44 pagineResuscitation Pharmacology: Dr. Beny Hartono, SPJP, FihaAna AgustinaNessuna valutazione finora
- Sign and SymptomsDocumento8 pagineSign and SymptomsCaral Grace Gatdula-PenalbaNessuna valutazione finora
- HypertensionDocumento19 pagineHypertensionmr_coolz282344Nessuna valutazione finora
- Seminar 4Documento49 pagineSeminar 4Yamuna SubramaniamNessuna valutazione finora
- Acute Leukemias: Clinical Pharmacy Iv Bachelor of PharmacyDocumento43 pagineAcute Leukemias: Clinical Pharmacy Iv Bachelor of PharmacyMuhammad Reza100% (2)
- Medical Terminology 4Documento26 pagineMedical Terminology 4ea4184386100% (1)
- Analyzing and Defining Medical TermsDocumento7 pagineAnalyzing and Defining Medical Termsmarcus colgroveNessuna valutazione finora
- Interpret Liver TestsDocumento4 pagineInterpret Liver TestsKaram Ali ShahNessuna valutazione finora
- Section 3: Nomenclature of TumorDocumento71 pagineSection 3: Nomenclature of TumorIsuri GanNessuna valutazione finora
- Commotio Cordis: R Eview A RticleDocumento24 pagineCommotio Cordis: R Eview A RticleYuji AdityaNessuna valutazione finora
- Heart Anatomy: LocationDocumento45 pagineHeart Anatomy: LocationZaira100% (1)
- Physio Coursepack 2016Documento282 paginePhysio Coursepack 2016Amanda KimNessuna valutazione finora
- AnaemiaDocumento27 pagineAnaemiaSamahir F HusseinNessuna valutazione finora
- Endocrine Notes - All in One FileDocumento182 pagineEndocrine Notes - All in One FilekjNessuna valutazione finora
- Leukemia - Pathophysiology of White Cells DisordersDocumento10 pagineLeukemia - Pathophysiology of White Cells DisordersJacecosmozNessuna valutazione finora
- 2 Cardiovascular System: Describe The Systemic Circulation in The Body and Give Its ImportanceDocumento28 pagine2 Cardiovascular System: Describe The Systemic Circulation in The Body and Give Its ImportanceBhavin ChangelaNessuna valutazione finora
- Summary ImmunologyDocumento1 paginaSummary ImmunologyNoor AlsheikhNessuna valutazione finora
- Efm CH 3Documento12 pagineEfm CH 3Hajar Aldhanhani0% (1)
- A Summary of The Chemical Mediators Involve in The Acute Inflammatory Response Is Shown in The Table BelowDocumento30 pagineA Summary of The Chemical Mediators Involve in The Acute Inflammatory Response Is Shown in The Table Belowinny100% (1)
- Top 100 Secrets About Critical CareDocumento8 pagineTop 100 Secrets About Critical CareMariaUlfaNessuna valutazione finora
- Kimberly F. v. Mary Hitchcock, 1st Cir. (1993)Documento34 pagineKimberly F. v. Mary Hitchcock, 1st Cir. (1993)Scribd Government DocsNessuna valutazione finora
- Chronic Inflammation Causes, Features and EffectsDocumento24 pagineChronic Inflammation Causes, Features and EffectsTommys100% (1)
- Advanced Cardiac Life SupportDocumento37 pagineAdvanced Cardiac Life SupportRoy Acosta GumbanNessuna valutazione finora
- Anaerobic Infections in HumansDa EverandAnaerobic Infections in HumansSydney FinegoldValutazione: 5 su 5 stelle5/5 (1)
- Free Physiology Books PDFDocumento2 pagineFree Physiology Books PDFTonya0% (2)
- KROK2 2010 Paper (200Qs)Documento62 pagineKROK2 2010 Paper (200Qs)Ali Zeeshan100% (1)
- Best Physiology TextbookDocumento3 pagineBest Physiology TextbookPeterNessuna valutazione finora
- Pre Assessment Diabetes Nursing CareDocumento4 paginePre Assessment Diabetes Nursing CareHabib UllahNessuna valutazione finora
- Pulmonary Patho PDFDocumento623 paginePulmonary Patho PDFNabeel Shahzad100% (1)
- Beta BlockersDocumento70 pagineBeta BlockersIrina Cabac-PogoreviciNessuna valutazione finora
- Basic Immunology: Ratna Windyaningrum Supervisor: Dr. Arif Dermawan, M.Kes., Sp. T.H.T.K.L (K)Documento42 pagineBasic Immunology: Ratna Windyaningrum Supervisor: Dr. Arif Dermawan, M.Kes., Sp. T.H.T.K.L (K)Ratna Windyaningrum100% (1)
- 3-Major Veins of The BodyDocumento26 pagine3-Major Veins of The BodyTJPlayz100% (1)
- Abdul Rahim Bin Mohamad Nor C 111 10 871: Prof - Dr.Peter Kabo, PHD, SPFK, SPJP (K), Fiha, FasccDocumento38 pagineAbdul Rahim Bin Mohamad Nor C 111 10 871: Prof - Dr.Peter Kabo, PHD, SPFK, SPJP (K), Fiha, FasccAis KonorasNessuna valutazione finora
- Coughing, A Simple Guide to The Condition, Treatment and Related ConditionsDa EverandCoughing, A Simple Guide to The Condition, Treatment and Related ConditionsNessuna valutazione finora
- Emergency Room Medicine - 4th EdDocumento32 pagineEmergency Room Medicine - 4th EdRaees ParmarNessuna valutazione finora
- PEDI PEARLS: Dr. Cortes Guide to Common Pediatric Respiratory IssuesDocumento46 paginePEDI PEARLS: Dr. Cortes Guide to Common Pediatric Respiratory Issuesthomasfx10100% (1)
- Cardiovascular Physiology: Cardiac Output, Blood Flow ControlsDocumento33 pagineCardiovascular Physiology: Cardiac Output, Blood Flow ControlsLuiz Jorge MendonçaNessuna valutazione finora
- 201103-Fkg-Drugs Act On Cardiovascular SystemDocumento19 pagine201103-Fkg-Drugs Act On Cardiovascular SystemEidelen Lovani Sembiring100% (1)
- GERIATRIC MEDICINE (Basic)Documento41 pagineGERIATRIC MEDICINE (Basic)Medical AdvicesNessuna valutazione finora
- Surgery NeurologyDocumento9 pagineSurgery Neurologyaam_tabishNessuna valutazione finora
- Acid-Base Disorders NotesDocumento10 pagineAcid-Base Disorders NotesLovely100% (1)
- Cardiovascular SystemDocumento40 pagineCardiovascular SystemDouglas Jacques100% (1)
- Introduction To HaematologyDocumento8 pagineIntroduction To HaematologyKasey ChaseNessuna valutazione finora
- Interview Pa Tool.Documento5 pagineInterview Pa Tool.Raisah Bint AbdullahNessuna valutazione finora
- SARP (Skin Anesthesia Radiology Psychiatry) Review 2010Documento4 pagineSARP (Skin Anesthesia Radiology Psychiatry) Review 2010QworldNessuna valutazione finora
- MEDICINE - Allergies and AnaphylaxisDocumento7 pagineMEDICINE - Allergies and AnaphylaxisZelle PeredasNessuna valutazione finora
- Chapter 020Documento8 pagineChapter 020api-281340024100% (1)
- Neurotransmitters in Schizophrenia: Dr. Adel El SheshaiDocumento47 pagineNeurotransmitters in Schizophrenia: Dr. Adel El SheshaielvinegunawanNessuna valutazione finora
- 1.rationale of Use of Antibiotic in Surgical Patients CDocumento22 pagine1.rationale of Use of Antibiotic in Surgical Patients CPanna SahaNessuna valutazione finora
- Vascular Responses to PathogensDa EverandVascular Responses to PathogensFelicity N.E. GavinsNessuna valutazione finora
- Chapter Two Tissue InjuryDocumento38 pagineChapter Two Tissue Injuryapi-19916399Nessuna valutazione finora
- Blood Test RangesDocumento18 pagineBlood Test Rangeskltran80Nessuna valutazione finora
- Medical Terminology 2 Cardiovascular System Lesson 1Documento3 pagineMedical Terminology 2 Cardiovascular System Lesson 1sotman58Nessuna valutazione finora
- Patient Case Presentation StructureDocumento30 paginePatient Case Presentation StructureAmira HelayelNessuna valutazione finora
- Introduction To ImmunologyDocumento21 pagineIntroduction To Immunologysaeed5220020% (1)
- In Mathematics: MultiplicationDocumento1 paginaIn Mathematics: Multiplicationsai calderNessuna valutazione finora
- Indian Culture: MultiplicationDocumento1 paginaIndian Culture: Multiplicationsai calderNessuna valutazione finora
- Evolution of The Glyph: Basic CalculationsDocumento1 paginaEvolution of The Glyph: Basic Calculationssai calderNessuna valutazione finora
- Anthropology: Usage and TermsDocumento1 paginaAnthropology: Usage and Termssai calderNessuna valutazione finora
- Arts and Entertainment: AlbumsDocumento1 paginaArts and Entertainment: Albumssai calderNessuna valutazione finora
- Green: Etymology and Linguistic DefinitionsDocumento1 paginaGreen: Etymology and Linguistic Definitionssai calderNessuna valutazione finora
- Music: Left May Refer ToDocumento1 paginaMusic: Left May Refer Tosai calderNessuna valutazione finora
- Places: Northern Ireland, UKDocumento1 paginaPlaces: Northern Ireland, UKsai calderNessuna valutazione finora
- Shades and Variations: Indigofera TinctoriaDocumento1 paginaShades and Variations: Indigofera Tinctoriasai calderNessuna valutazione finora
- In Mathematics: List of Basic CalculationsDocumento1 paginaIn Mathematics: List of Basic Calculationssai calderNessuna valutazione finora
- ForwardDocumento1 paginaForwardsai calderNessuna valutazione finora
- RightsDocumento1 paginaRightssai calderNessuna valutazione finora
- Shades and Variations: This Article Is About The Color. For Other Uses, SeeDocumento1 paginaShades and Variations: This Article Is About The Color. For Other Uses, Seesai calderNessuna valutazione finora
- FootDocumento1 paginaFootsai calderNessuna valutazione finora
- BrownDocumento1 paginaBrownsai calderNessuna valutazione finora
- HandDocumento1 paginaHandsai calderNessuna valutazione finora
- Acetylcholine ReceptorDocumento1 paginaAcetylcholine Receptorsai calderNessuna valutazione finora
- Orange: Arts, Entertainment, and MediaDocumento1 paginaOrange: Arts, Entertainment, and Mediasai calderNessuna valutazione finora
- Astral: Concepts of The Non-PhysicalDocumento1 paginaAstral: Concepts of The Non-Physicalsai calderNessuna valutazione finora
- FootDocumento1 paginaFootsai calderNessuna valutazione finora
- Non-Compound EyesDocumento1 paginaNon-Compound Eyessai calderNessuna valutazione finora
- Subtle: Subtle May Refer ToDocumento1 paginaSubtle: Subtle May Refer Tosai calderNessuna valutazione finora
- Thought PDFDocumento1 paginaThought PDFsai calderNessuna valutazione finora
- MentalDocumento1 paginaMentalsai calderNessuna valutazione finora
- CausalityDocumento1 paginaCausalitysai calderNessuna valutazione finora
- PhysicalDocumento1 paginaPhysicalsai calderNessuna valutazione finora
- BehaviorDocumento1 paginaBehaviorsai calderNessuna valutazione finora
- Anesthetic PDFDocumento1 paginaAnesthetic PDFsai calderNessuna valutazione finora
- Anesthetic PDFDocumento1 paginaAnesthetic PDFsai calderNessuna valutazione finora
- How to prepare your Asil for fightingDocumento16 pagineHow to prepare your Asil for fightingcinna01Nessuna valutazione finora
- 2017 Functional Anatomy Test QuestionsDocumento10 pagine2017 Functional Anatomy Test QuestionsmarcusNessuna valutazione finora
- Bapat Et Al. - 2006 - Quantification of Metabolically Active Biomass Using Methylene Blue Dye Reduction Test (MBRT) Measurement of CFU IDocumento10 pagineBapat Et Al. - 2006 - Quantification of Metabolically Active Biomass Using Methylene Blue Dye Reduction Test (MBRT) Measurement of CFU IJosé Matías ZapiolaNessuna valutazione finora
- Chronic Low Back Pain Good Clinical Practice GCPDocumento341 pagineChronic Low Back Pain Good Clinical Practice GCPTru ManNessuna valutazione finora
- AdenoidsDocumento8 pagineAdenoidsUjjawalShriwastavNessuna valutazione finora
- CommonGround 8 26 BrierleyDocumento84 pagineCommonGround 8 26 Brierleytuinbroek_94397869Nessuna valutazione finora
- 13497-Texto Del Artículo-48998-1-10-20150925Documento7 pagine13497-Texto Del Artículo-48998-1-10-20150925Pipe Contecha BernatteNessuna valutazione finora
- Types of Casts and Their IndicationsDocumento3 pagineTypes of Casts and Their IndicationsPhylum ChordataNessuna valutazione finora
- Zingiber Officinale MonographDocumento5 pagineZingiber Officinale Monographc_j_bhattNessuna valutazione finora
- Aos 94 10Documento11 pagineAos 94 10Andi Tiara S. AdamNessuna valutazione finora
- Masters in Medical Science - MMSCDocumento12 pagineMasters in Medical Science - MMSCtexilaamericanNessuna valutazione finora
- Mink Dissection InstructionsDocumento15 pagineMink Dissection InstructionsMark PenticuffNessuna valutazione finora
- Materials Compatibility List: Chemicals For Processing Endoscopes and Endoscopic InstrumentsDocumento24 pagineMaterials Compatibility List: Chemicals For Processing Endoscopes and Endoscopic InstrumentsarimudaNessuna valutazione finora
- Psychological Assessment ReviewerDocumento9 paginePsychological Assessment Reviewerpatquianzon100% (1)
- Klinefelter SyndromeDocumento6 pagineKlinefelter Syndromemeeeenon100% (1)
- Thulium e Alopecia AndrogenéticaDocumento9 pagineThulium e Alopecia AndrogenéticacristianneNessuna valutazione finora
- Not Eligible As No Experience of Teaching and ResearchDocumento5 pagineNot Eligible As No Experience of Teaching and ResearchVasanth Kumar AllaNessuna valutazione finora
- A Brief History of Evidence-Based Medicine in Four PeriodsDocumento31 pagineA Brief History of Evidence-Based Medicine in Four PeriodsSaad MotawéaNessuna valutazione finora
- AcetaminophenDocumento2 pagineAcetaminophenKimskiusNessuna valutazione finora
- Phagocytosis Assay Kit (Igg Fitc) : Item No. 500290Documento9 paginePhagocytosis Assay Kit (Igg Fitc) : Item No. 500290drfiatNessuna valutazione finora
- 20 Uses of Vicks VaporubDocumento3 pagine20 Uses of Vicks VaporubDrBertram ForerNessuna valutazione finora
- Negative Feedback Thyroxine and Adrenelin WsDocumento2 pagineNegative Feedback Thyroxine and Adrenelin WsEllie AbelNessuna valutazione finora
- Disturbing Art Exposes Modern Culture AbsurditiesDocumento15 pagineDisturbing Art Exposes Modern Culture Absurdities2aethicusNessuna valutazione finora
- Tza STG Neml 2007 PDFDocumento220 pagineTza STG Neml 2007 PDFJohnny EmperorNessuna valutazione finora
- Dressing and BandagingDocumento5 pagineDressing and BandagingMaricar Gallamora Dela CruzNessuna valutazione finora
- Anemia: Differential DiagnosisDocumento7 pagineAnemia: Differential DiagnosisZaman MigozaradNessuna valutazione finora
- Uttar Pradesh Empanelment List for Minilap 2018-19Documento19 pagineUttar Pradesh Empanelment List for Minilap 2018-19Vijay KumarNessuna valutazione finora
- Ten Days in A Mad-House by Nellie BlyDocumento122 pagineTen Days in A Mad-House by Nellie BlyCharmaineTanti100% (1)