Potrebbero piacerti anche
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (73)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- Certificado V34aDocumento1 paginaCertificado V34aElizabeth Durán SánchezNessuna valutazione finora
- .Cancer DiseaseDocumento10 pagine.Cancer DiseasejanakrajchauhanNessuna valutazione finora
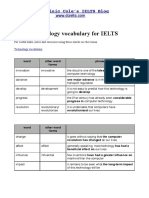
- Technology VocabularyDocumento3 pagineTechnology VocabularyChixo GalaxyNessuna valutazione finora
- Biology: Higher Tier Paper 1HDocumento28 pagineBiology: Higher Tier Paper 1HkaruneshnNessuna valutazione finora
- Sabas fOR THE FRCR 2aDocumento9 pagineSabas fOR THE FRCR 2aMohammad Shafiq0% (1)
- 06 Brakes PDFDocumento6 pagine06 Brakes PDFAKILI PSINessuna valutazione finora
- MIXDECK - FAQ and Troubleshooting 01Documento8 pagineMIXDECK - FAQ and Troubleshooting 01F>F>Nessuna valutazione finora
- Laura Gentile Letter On Hampden County CourthouseDocumento6 pagineLaura Gentile Letter On Hampden County CourthouseMassLiveNessuna valutazione finora
- The Rheological Properties of Ketchup As A Function of Different Hydrocolloids and TemperatureDocumento8 pagineThe Rheological Properties of Ketchup As A Function of Different Hydrocolloids and TemperatureVicente WiethNessuna valutazione finora
- System Substation Commissioning TestsDocumento8 pagineSystem Substation Commissioning TestsCvijayakumar100% (1)
- Quiz13 130630200754 Phpapp02Documento10 pagineQuiz13 130630200754 Phpapp02anukrititiwaNessuna valutazione finora
- L 7 Thermal Death Time DataDocumento21 pagineL 7 Thermal Death Time DataVaibhav GuptaNessuna valutazione finora
- Book of Bible Answers (Volume 1) - by Doug-BatchelorDocumento138 pagineBook of Bible Answers (Volume 1) - by Doug-BatchelorAdventist_Truth100% (3)
- Method Statement For Boom Barrier Installation (Rev00) ELV2Documento38 pagineMethod Statement For Boom Barrier Installation (Rev00) ELV2balajiNessuna valutazione finora
- Role of BisoprololDocumento43 pagineRole of BisoprololFidel Martua Marpaung67% (3)
- Ficha Tecnica p501Documento4 pagineFicha Tecnica p501LizbethNessuna valutazione finora
- The Determinants of Service Quality and Customer Satisfaction in Malaysian e Hailing ServicesDocumento8 pagineThe Determinants of Service Quality and Customer Satisfaction in Malaysian e Hailing ServicesYoannisa AtinaNessuna valutazione finora
- Fuel Tank Truck Afd-091005-058Documento40 pagineFuel Tank Truck Afd-091005-058cascade1100% (1)
- Spining Mill in IndiaDocumento74 pagineSpining Mill in IndiaMahendra Shah100% (4)
- Gujarat-Ports Sector ReportDocumento17 pagineGujarat-Ports Sector ReportK. Ashok Vardhan ShettyNessuna valutazione finora
- Poem Summary - Keeping QuietDocumento3 paginePoem Summary - Keeping QuietVignesh Mohan100% (2)
- Coronary Stents: Current StatusDocumento42 pagineCoronary Stents: Current StatusMANSI SALUNKENessuna valutazione finora
- RAJPUT - Gokul IndustryDocumento76 pagineRAJPUT - Gokul IndustryrajputvjNessuna valutazione finora
- Ao+ WDM12 R40DDocumento8 pagineAo+ WDM12 R40DPedro Igor Oliveira CarvalhoNessuna valutazione finora
- Internship ReportDocumento50 pagineInternship ReportSachinNessuna valutazione finora
- A Report On External Analysis of Construction in NepalDocumento13 pagineA Report On External Analysis of Construction in Nepalsubash upretiNessuna valutazione finora
- Documentation ExamplesDocumento5 pagineDocumentation ExamplesErika HarveryNessuna valutazione finora
- 10 Powerful Mudras and How To Use Them: 1. GyanDocumento4 pagine10 Powerful Mudras and How To Use Them: 1. GyanAkrithi Akrithi100% (1)
- Euroncap 2017 Audi q5 DatasheetDocumento13 pagineEuroncap 2017 Audi q5 DatasheetCosmin AnculiaNessuna valutazione finora
- Commissioning Valve Product BrochureDocumento14 pagineCommissioning Valve Product BrochureblindjaxxNessuna valutazione finora