Potrebbero piacerti anche
- Vascular Access For Hemodialysis Patients: New Data Should Guide Decision MakingDocumento8 pagineVascular Access For Hemodialysis Patients: New Data Should Guide Decision MakingHeri IrawanNessuna valutazione finora
- Tumor Kanker TiroidDocumento9 pagineTumor Kanker TiroidyuliantoNessuna valutazione finora
- Comparison of Surgical Versus Percutaneously Created Arteriovenous Hemodialysis FistulasDocumento9 pagineComparison of Surgical Versus Percutaneously Created Arteriovenous Hemodialysis Fistulasmananlamba863Nessuna valutazione finora
- Jorgensen 2019Documento8 pagineJorgensen 2019Emeray EssenceNessuna valutazione finora
- Benali Et Al 2023 Procedure Related Complications of Catheter Ablation For Atrial FibrillationDocumento11 pagineBenali Et Al 2023 Procedure Related Complications of Catheter Ablation For Atrial FibrillationjlmoralesartNessuna valutazione finora
- Temporary Inferior Vena Cava Filters: How Do We Move Forward?Documento3 pagineTemporary Inferior Vena Cava Filters: How Do We Move Forward?MostafaNessuna valutazione finora
- European Guidelines On Perioperative Venous.6Documento4 pagineEuropean Guidelines On Perioperative Venous.6ionut.andruscaNessuna valutazione finora
- Readings in "Prevention of Peripheral Venous CatheterDocumento3 pagineReadings in "Prevention of Peripheral Venous CatheterJoanne Kathleen SantolicesNessuna valutazione finora
- Diagnosis and Treatment of Vascular Air EmbolismDocumento14 pagineDiagnosis and Treatment of Vascular Air EmbolismAdsoni IndoNessuna valutazione finora
- Rahman 2016Documento3 pagineRahman 2016Rabin SitumorangNessuna valutazione finora
- VATS Versus Open Surgery For Lung Cancer Resection: Moving Toward A Minimally Invasive ApproachDocumento3 pagineVATS Versus Open Surgery For Lung Cancer Resection: Moving Toward A Minimally Invasive ApproachAlin Ionut BurlacuNessuna valutazione finora
- Indications For Percutaneous Left Atrial Appendage.5Documento7 pagineIndications For Percutaneous Left Atrial Appendage.5吳醫師Nessuna valutazione finora
- Arteriovenous FistulasDocumento21 pagineArteriovenous FistulasDragos GarofilNessuna valutazione finora
- Tracking Arteriovenous Fistula Maturation: A Novel Approach: Research Article - Advances in CKD 2019Documento6 pagineTracking Arteriovenous Fistula Maturation: A Novel Approach: Research Article - Advances in CKD 2019Anonymous ATdLPZNessuna valutazione finora
- Overview of Hemodialysis Access and Assessment - PMCDocumento17 pagineOverview of Hemodialysis Access and Assessment - PMCvwyldrNessuna valutazione finora
- Deep Venous Thrombosis After Percutaneous Insertion of Vena Caval FiltersDocumento9 pagineDeep Venous Thrombosis After Percutaneous Insertion of Vena Caval Filtersari kurniawanNessuna valutazione finora
- IMP Shock Etiol 5y Outcome VA-ECMO Edit 2023Documento3 pagineIMP Shock Etiol 5y Outcome VA-ECMO Edit 2023vladbvs16Nessuna valutazione finora
- Role of Endoscopy in The Management of Variceal HemorrhageDocumento7 pagineRole of Endoscopy in The Management of Variceal HemorrhageAmelia Fitria DewiNessuna valutazione finora
- VP Shunt and ComplicationDocumento5 pagineVP Shunt and ComplicationFabiola VaniaNessuna valutazione finora
- Surgical Treatment of BAV JTCVS 2014Documento10 pagineSurgical Treatment of BAV JTCVS 2014juajimenez55Nessuna valutazione finora
- Open Surgical Repair of Abdominal Aortic Aneurysms Maintains A Pivotal Role in The Endovascular EraDocumento10 pagineOpen Surgical Repair of Abdominal Aortic Aneurysms Maintains A Pivotal Role in The Endovascular EraAnna Sofía ParedesNessuna valutazione finora
- A Comparative Study Between Radiocephalic and Brachiocephalic Arteriovenous Fistula in End Stage Renal DiseaseDocumento6 pagineA Comparative Study Between Radiocephalic and Brachiocephalic Arteriovenous Fistula in End Stage Renal Diseasearinda calvine santosoNessuna valutazione finora
- Trachtenberg 2015Documento7 pagineTrachtenberg 2015Sufyan HadiNessuna valutazione finora
- Atrioventricular Septal Defects: EditorialDocumento3 pagineAtrioventricular Septal Defects: EditorialFinaARNessuna valutazione finora
- Prosthetic Valve Endocarditis: State of The Heart: Review: Clinical Trial OutcomesDocumento15 pagineProsthetic Valve Endocarditis: State of The Heart: Review: Clinical Trial OutcomesUshnish ChakrabartyNessuna valutazione finora
- 2020 Article 2138Documento10 pagine2020 Article 2138Andi Tiara S. AdamNessuna valutazione finora
- Outcomes of Patients Referred For Arteriovenous Fistula Construction: A Systematic ReviewDocumento9 pagineOutcomes of Patients Referred For Arteriovenous Fistula Construction: A Systematic ReviewAnonymous ATdLPZNessuna valutazione finora
- Julliard Worse Outcomes EVH 2011Documento7 pagineJulliard Worse Outcomes EVH 2011Mary MoraNessuna valutazione finora
- 1 s2.0 S0093775422000525 MainDocumento4 pagine1 s2.0 S0093775422000525 MainAchmad Dodi MeidiantoNessuna valutazione finora
- Critical Care Management of The Lung Transplant RecipientDocumento15 pagineCritical Care Management of The Lung Transplant RecipienttaniaNessuna valutazione finora
- Liver Transplantation - 2009 - Lim - Endoscopic Variceal Ligation For Primary Prophylaxis of Esophageal Variceal HemorrhageDocumento6 pagineLiver Transplantation - 2009 - Lim - Endoscopic Variceal Ligation For Primary Prophylaxis of Esophageal Variceal Hemorrhagedarlington D. y ayimNessuna valutazione finora
- Increased Minimum Vein Diameter On PreoperativeDocumento40 pagineIncreased Minimum Vein Diameter On PreoperativeMikael AngelooNessuna valutazione finora
- The Management of Abdominal Aortic AneurysmDocumento7 pagineThe Management of Abdominal Aortic AneurysmShaastieNessuna valutazione finora
- The Rise of Prevalence and The Fall of Mortality of Patients With Acute Renal Failure: What The Analysis of Two Databases Does and Does Not Tell UsDocumento3 pagineThe Rise of Prevalence and The Fall of Mortality of Patients With Acute Renal Failure: What The Analysis of Two Databases Does and Does Not Tell UsLivia Meidy UbayidNessuna valutazione finora
- AvenewDocumento12 pagineAvenewNachchakorn DellNessuna valutazione finora
- 5 Sagban2015Documento7 pagine5 Sagban2015mihaelamocanNessuna valutazione finora
- WJN 4 148Documento13 pagineWJN 4 148Rafela Agatha ChristyNessuna valutazione finora
- Inferior Vena Cava Ultrasonography For Volume Status EvaluationDocumento13 pagineInferior Vena Cava Ultrasonography For Volume Status Evaluationtavo570Nessuna valutazione finora
- Prospective Evaluation of Factors Associated With Early Failure of Arteriovenous Fistulae in Hemodialysis PatientsDocumento5 pagineProspective Evaluation of Factors Associated With Early Failure of Arteriovenous Fistulae in Hemodialysis PatientsIvor WilopoNessuna valutazione finora
- Abdominal Aortic AneurysmsDocumento60 pagineAbdominal Aortic Aneurysmsroata cristianNessuna valutazione finora
- Risk Assessment As A Guide To Thrombosis Prophylaxis in Bariatric Surgical PatientsDocumento4 pagineRisk Assessment As A Guide To Thrombosis Prophylaxis in Bariatric Surgical PatientssaludortizNessuna valutazione finora
- Jco 2005 06 084Documento6 pagineJco 2005 06 084Nurul SafitriNessuna valutazione finora
- Arteriovenous Fistulae For Haemodialysis: A Systematic Review and Meta-Analysis of Ef Ficacy and Safety OutcomesDocumento10 pagineArteriovenous Fistulae For Haemodialysis: A Systematic Review and Meta-Analysis of Ef Ficacy and Safety OutcomesMarco Antonio Galvan RuizNessuna valutazione finora
- Factors That Influence Venous Leg Ulcer Healing and Recurrence Rate After Endovenous Radiofrequency Ablation of Incompetent Saphenous VeinDocumento6 pagineFactors That Influence Venous Leg Ulcer Healing and Recurrence Rate After Endovenous Radiofrequency Ablation of Incompetent Saphenous VeinHan's OfficialNessuna valutazione finora
- Last BreathDocumento2 pagineLast BreathAnnie Elizabeth TorresNessuna valutazione finora
- Varicose Veins Diagnosis and TreatmentDocumento7 pagineVaricose Veins Diagnosis and Treatmenthossein kasiriNessuna valutazione finora
- Management of Epistaxis in Patients With Ventricular Assist Device: A Retrospective ReviewDocumento6 pagineManagement of Epistaxis in Patients With Ventricular Assist Device: A Retrospective ReviewDenta HaritsaNessuna valutazione finora
- Aortic Stenosis and Transcatheter Aortic Valve Implantation: Current Status and Future Directions in KoreaDocumento15 pagineAortic Stenosis and Transcatheter Aortic Valve Implantation: Current Status and Future Directions in Koreaخديجة عمرNessuna valutazione finora
- Validacion CPISDocumento5 pagineValidacion CPISXavier AbrilNessuna valutazione finora
- The Eschar Trial: Should It Change Practice?: David D. I. Wright, MB, BSC, FrcsDocumento5 pagineThe Eschar Trial: Should It Change Practice?: David D. I. Wright, MB, BSC, FrcsNthie UnguNessuna valutazione finora
- 1047 FullDocumento7 pagine1047 Fullnaxo128Nessuna valutazione finora
- Neumonia Asosiada A VentiladorDocumento11 pagineNeumonia Asosiada A VentiladorYnomata RusamellNessuna valutazione finora
- Pi Is 0741521421004754Documento12 paginePi Is 0741521421004754Essam KhalafNessuna valutazione finora
- ACO Peripro 2016Documento10 pagineACO Peripro 2016Philippe Bocanegra FernándezNessuna valutazione finora
- Contemporary Management of Sigmoid VolvulusDocumento8 pagineContemporary Management of Sigmoid VolvulusWILLIAM RICARDO EFFIO GALVEZNessuna valutazione finora
- In Ammation of The Pleural CavityDocumento24 pagineIn Ammation of The Pleural CavityMáximo Saldaña TorresNessuna valutazione finora
- Ijbt0012 0121Documento6 pagineIjbt0012 0121Serque777Nessuna valutazione finora
- VTE Profilaxis in CancerDocumento27 pagineVTE Profilaxis in CancerPedro AzevedoNessuna valutazione finora
- Dialysis Access ManagementDa EverandDialysis Access ManagementSteven WuNessuna valutazione finora
- Bronchiolitis Obliterans Syndrome in Lung TransplantationDa EverandBronchiolitis Obliterans Syndrome in Lung TransplantationNessuna valutazione finora
- DR - Dikshit ResumeDocumento4 pagineDR - Dikshit ResumeRajiveDikshitNessuna valutazione finora
- Diabetes in Pregnancy: Supervisor: DR Rathimalar By: DR Ashwini Arumugam & DR Laily MokhtarDocumento21 pagineDiabetes in Pregnancy: Supervisor: DR Rathimalar By: DR Ashwini Arumugam & DR Laily MokhtarHarleyquinn96 DrNessuna valutazione finora
- Medical Catastrophe PDFDocumento221 pagineMedical Catastrophe PDFghuoiNessuna valutazione finora
- Emerging Endoscopic Treatments For Nonvariceal Upper Gastrointestinal HemorrhageDocumento14 pagineEmerging Endoscopic Treatments For Nonvariceal Upper Gastrointestinal HemorrhageIsais NNessuna valutazione finora
- ACR White Paper Ovarian IncidentalomaDocumento7 pagineACR White Paper Ovarian IncidentalomaMaxNessuna valutazione finora
- Dwarfism: Navigation Search Dwarf (Germanic Mythology) DwarfDocumento15 pagineDwarfism: Navigation Search Dwarf (Germanic Mythology) DwarfManzano JenecaNessuna valutazione finora
- Assessment of Fetal Lung MaturityDocumento12 pagineAssessment of Fetal Lung MaturityAnton Supono Wong TekAnNessuna valutazione finora
- Solo Protect Case Study - Healthcare at HomeDocumento2 pagineSolo Protect Case Study - Healthcare at HomentapianNessuna valutazione finora
- Participant DrillDocumento2 pagineParticipant DrillponekNessuna valutazione finora
- Health Centre FinalDocumento22 pagineHealth Centre FinalEmmanuel CarltonNessuna valutazione finora
- CME Miscarriages Combined 1Documento76 pagineCME Miscarriages Combined 1syawal zulfitriNessuna valutazione finora
- Jurnal Bedah 11Documento20 pagineJurnal Bedah 11Andhyka Brillian KharismaNessuna valutazione finora
- Nursing Role of Cardiac and Respiratory Arrest Checklist 2022 ApproveDocumento3 pagineNursing Role of Cardiac and Respiratory Arrest Checklist 2022 ApproveDo0odi AlharbiNessuna valutazione finora
- Editorial Board 2013 Journal of The American Academy of DermatologyDocumento1 paginaEditorial Board 2013 Journal of The American Academy of DermatologyYusmiatiNessuna valutazione finora
- Principles of Casting and SplintingDocumento8 paginePrinciples of Casting and Splintingbobtaguba100% (1)
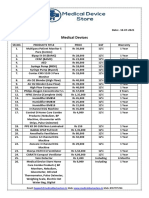
- Medical Device Store Products CatalogueDocumento3 pagineMedical Device Store Products CatalogueWasim KhatibNessuna valutazione finora
- Microsoft Power Point - Tidal Therapy Approved 11-11-09Documento39 pagineMicrosoft Power Point - Tidal Therapy Approved 11-11-09kamsechlerNessuna valutazione finora
- Hpeb 300 Final ReportDocumento21 pagineHpeb 300 Final Reportapi-336103510Nessuna valutazione finora
- 4, FHSIS Indicators, Formula & TargetDocumento6 pagine4, FHSIS Indicators, Formula & Targetkkabness101 YUL100% (3)
- Obturation Techniques and DevicesDocumento29 pagineObturation Techniques and DevicesArivinthaan Tanigajalam100% (1)
- Infertility Social ImpactDocumento3 pagineInfertility Social ImpactAlisha SyiemliehNessuna valutazione finora
- Name: Ra Tuty Kuswardhani Md. PHD, Mha, Finasim, Geriatrician Pembina Utama Madya / Iv D/ Head LectorDocumento27 pagineName: Ra Tuty Kuswardhani Md. PHD, Mha, Finasim, Geriatrician Pembina Utama Madya / Iv D/ Head LectorMardikaNessuna valutazione finora
- Eacvi Recommendations Valvular Regurgitation Summary PDFDocumento34 pagineEacvi Recommendations Valvular Regurgitation Summary PDFstoicea_katalinNessuna valutazione finora
- ANA Nursing Sensitive Indicator PDFDocumento29 pagineANA Nursing Sensitive Indicator PDFAchmad Hidayatullah HafidNessuna valutazione finora
- 04 CIN and Cervical Cancer UNEDITEDDocumento120 pagine04 CIN and Cervical Cancer UNEDITEDRalph JuicoNessuna valutazione finora
- What Is An Intravenous Pyelogram (IVP) ? How Should I Prepare?Documento4 pagineWhat Is An Intravenous Pyelogram (IVP) ? How Should I Prepare?vindictive666Nessuna valutazione finora
- Log Book BedahDocumento51 pagineLog Book BedahaghniaNessuna valutazione finora
- 7 Point SGA JPEN Apr 15 Online FirstDocumento9 pagine7 Point SGA JPEN Apr 15 Online FirstNoviana ZaraNessuna valutazione finora
- Enigma 1 Trial 2007Documento11 pagineEnigma 1 Trial 2007Jason TiongNessuna valutazione finora
- Or JournalDocumento2 pagineOr JournalNathaniel PulidoNessuna valutazione finora