Potrebbero piacerti anche
- Clinical Signs in Humans and Animals Associated with Minerals, Trace Elements and Rare Earth ElementsDa EverandClinical Signs in Humans and Animals Associated with Minerals, Trace Elements and Rare Earth ElementsNessuna valutazione finora
- The Regulatory Genome in Adaptation, Evolution, Development, and DiseaseDa EverandThe Regulatory Genome in Adaptation, Evolution, Development, and DiseaseNessuna valutazione finora
- Bio Inorganic 1 PPT ChemistryDocumento57 pagineBio Inorganic 1 PPT ChemistryShantanu MawaskarNessuna valutazione finora
- Inborn Errors or MetabolismDocumento25 pagineInborn Errors or MetabolismSamdiSutantoNessuna valutazione finora
- Food-Drug Interaction: Presented By: Deepika Baranwal PHD ScholarDocumento29 pagineFood-Drug Interaction: Presented By: Deepika Baranwal PHD ScholarUncu LiviaNessuna valutazione finora
- Inborn Errors of Metabolism LectureDocumento32 pagineInborn Errors of Metabolism LectureEMMANUEL ABEL IMAH100% (1)
- Fluids & Electrolytes 5Documento14 pagineFluids & Electrolytes 5Justin Angelo SildoraNessuna valutazione finora
- Eating DisordersDocumento9 pagineEating DisordersFatin Nurina Mohd NazemiNessuna valutazione finora
- Lecture Notes CALCIUM HOMEOSTASISDocumento8 pagineLecture Notes CALCIUM HOMEOSTASISREMAN ALINGASANessuna valutazione finora
- OSTEOMALACIADocumento2 pagineOSTEOMALACIARosda BalimbinganNessuna valutazione finora
- Osteomalacia: Risk Factors Diagnosis Disease Clinical Manifestation Diagnostic FindingDocumento2 pagineOsteomalacia: Risk Factors Diagnosis Disease Clinical Manifestation Diagnostic FindingRosda BalimbinganNessuna valutazione finora
- Inborn Errors of MetabolismDocumento61 pagineInborn Errors of MetabolismVinay PatilNessuna valutazione finora
- Comprehensive Management SarcopeniaDocumento25 pagineComprehensive Management SarcopeniaMardikaNessuna valutazione finora
- Vitamins TableDocumento1 paginaVitamins TableMicah Lou CalambaNessuna valutazione finora
- Introduction To MineralsDocumento22 pagineIntroduction To MineralsJaveria MerajNessuna valutazione finora
- Zellweger Syndrome: Polytechnic College of Davao Del SurDocumento8 pagineZellweger Syndrome: Polytechnic College of Davao Del SurChristian Paul R. LasalaNessuna valutazione finora
- 23 Triyani - Asuhan Gizi Ginjal KronisDocumento30 pagine23 Triyani - Asuhan Gizi Ginjal KronisFanda RubakNessuna valutazione finora
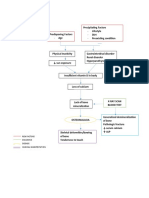
- Phatway CKD: Penurunan Fungsi NefronDocumento3 paginePhatway CKD: Penurunan Fungsi NefronAnggita AgustinaNessuna valutazione finora
- Kelainan Metabolik Dan Endokrin Oleh Dr. RonaldDocumento48 pagineKelainan Metabolik Dan Endokrin Oleh Dr. RonaldOdilia Maria RahalusNessuna valutazione finora
- An Def Fe Tk4Documento17 pagineAn Def Fe Tk4putridwierlindaNessuna valutazione finora
- 2 NCM114Documento24 pagine2 NCM114Adrian SantiagoNessuna valutazione finora
- Vitamins and Minerals GuideDocumento3 pagineVitamins and Minerals GuideJustin AncogNessuna valutazione finora
- Secondary Osteoporosis AssessmentDocumento12 pagineSecondary Osteoporosis AssessmentBibiana Prada de Camargo ColenciNessuna valutazione finora
- Naturopathic Nutrition Trace Elements GuideDocumento38 pagineNaturopathic Nutrition Trace Elements Guideglenn johnstonNessuna valutazione finora
- 1st Year FND21, BIOCHEMICAL COMPOSITION OF CELL-II - 24022021Documento26 pagine1st Year FND21, BIOCHEMICAL COMPOSITION OF CELL-II - 24022021Egg TorNessuna valutazione finora
- MBR 2019 - Pathology HandoutsDocumento98 pagineMBR 2019 - Pathology HandoutsRgm UyNessuna valutazione finora
- OSTEOPOROSIS, OSTEOMALACIA & PAGET DISEASEDocumento108 pagineOSTEOPOROSIS, OSTEOMALACIA & PAGET DISEASEYauffa Hanna Elt MisykahNessuna valutazione finora
- FarmaDocumento1 paginaFarmaefewtrNessuna valutazione finora
- Mitochondrial DiseasesDocumento34 pagineMitochondrial DiseasesAli MansorNessuna valutazione finora
- In The Name of GodDocumento46 pagineIn The Name of GodGalaxyNessuna valutazione finora
- SBRC General PrinciplesDocumento51 pagineSBRC General Principlesdalia khamoNessuna valutazione finora
- Anemia Defisiensi FeDocumento17 pagineAnemia Defisiensi FeSony WirasaktiNessuna valutazione finora
- Bone, Joint and Soft TissueDocumento10 pagineBone, Joint and Soft Tissuesarguss14100% (2)
- Bolile Genetice de MetabolismDocumento7 pagineBolile Genetice de MetabolismIoana Gal100% (1)
- Care for Patients with Fluid and Electrolyte ImbalancesDocumento10 pagineCare for Patients with Fluid and Electrolyte ImbalancesAbigail LonoganNessuna valutazione finora
- Fluid & ElectrolyteDocumento69 pagineFluid & ElectrolytePaul Ebenezer100% (1)
- Lab Normal Value S&Sof S&Sof : Loma Linda University School of Nursing Accepted Lab Values Adapted From KaplanDocumento3 pagineLab Normal Value S&Sof S&Sof : Loma Linda University School of Nursing Accepted Lab Values Adapted From KaplanGiacen100% (3)
- Human Hygiene and DiseasesDocumento10 pagineHuman Hygiene and Diseasesashokbhat19559402100% (2)
- Clinical Chemistry 2 Lecture Notes in Trace ElementsDocumento6 pagineClinical Chemistry 2 Lecture Notes in Trace ElementsMoira Pauline LibroraniaNessuna valutazione finora
- Bch417 Ln1 Biochemical Basis of DiseasesDocumento11 pagineBch417 Ln1 Biochemical Basis of DiseasesidriscognitoleadsNessuna valutazione finora
- Chemotherapeutic AgentsDocumento2 pagineChemotherapeutic AgentsmajNessuna valutazione finora
- Curs 7 Ca, MG, PDocumento31 pagineCurs 7 Ca, MG, PAndreea AronNessuna valutazione finora
- Vitamin Functions Characteristics Deficiency RDA Food SourcesDocumento9 pagineVitamin Functions Characteristics Deficiency RDA Food SourcesJoren Angela GalangNessuna valutazione finora
- Lesson 7.1 Inborn Errors of MetabolismDocumento119 pagineLesson 7.1 Inborn Errors of Metabolismmisaki06100% (2)
- Hematology SummaryDocumento9 pagineHematology SummaryJovielle Hayden100% (1)
- 1 - PATHOLOGY - Cellular Injury, Cellular Adaptation, and Cell Death LectureDocumento25 pagine1 - PATHOLOGY - Cellular Injury, Cellular Adaptation, and Cell Death Lectureregeti bhargavNessuna valutazione finora
- ATAXIAS PTDocumento13 pagineATAXIAS PTKarunya VkNessuna valutazione finora
- Chemotherapeutic Agents - StudentDocumento32 pagineChemotherapeutic Agents - Studentcaitie miracleNessuna valutazione finora
- Approach To in Born Errors of MetabolismDocumento112 pagineApproach To in Born Errors of MetabolismGurpreet Singh100% (3)
- Vitamin DeficienciesDocumento8 pagineVitamin DeficienciesCheskaLevineNessuna valutazione finora
- Nutritional Management On Kidney Disease: Prof DR DR Haerani Rasyid, Mkes, SPPD, KGH, SPGK 2018Documento108 pagineNutritional Management On Kidney Disease: Prof DR DR Haerani Rasyid, Mkes, SPPD, KGH, SPGK 2018Rahmawati HamudiNessuna valutazione finora
- AsKep - GGK Meri Punya Terbaru BGTDocumento24 pagineAsKep - GGK Meri Punya Terbaru BGTAnonymous nhZCowNessuna valutazione finora
- Vitamin and Micro Nutrients ChartDocumento2 pagineVitamin and Micro Nutrients ChartsublunderNessuna valutazione finora
- Detect Metabolic Disorders Early with Laboratory TestsDocumento21 pagineDetect Metabolic Disorders Early with Laboratory Testssaleema11Nessuna valutazione finora
- Ammonia Manganese: AstrocytesDocumento2 pagineAmmonia Manganese: AstrocytesJULIUS ART VINCENT A. PADINITNessuna valutazione finora
- Metabolic Disorder2 and Degenerative Disorderindonesia1Documento23 pagineMetabolic Disorder2 and Degenerative Disorderindonesia1Ardena Maulidia HamdaniNessuna valutazione finora
- Biochem Quick Review by Haji MuhammadDocumento7 pagineBiochem Quick Review by Haji Muhammadimran dilawarNessuna valutazione finora
- Anemia Table283Documento2 pagineAnemia Table283Bridget ParkerNessuna valutazione finora
- Managing Chronic Kidney Disease in Patients with DiabetesDocumento47 pagineManaging Chronic Kidney Disease in Patients with DiabetesTamzid Rabby TanmoyNessuna valutazione finora
- OTM 101 Nursing MnemonicsDocumento2 pagineOTM 101 Nursing MnemonicsMarlena Nicole100% (6)
- Cognitive Development of Infants and ToddlersDocumento1 paginaCognitive Development of Infants and ToddlersCyrell Rondina100% (2)
- SBR2018 - AbstractsDocumento115 pagineSBR2018 - AbstractsGustavo ResendeNessuna valutazione finora
- Respiratory Medicine 1 50Documento33 pagineRespiratory Medicine 1 50Ahmed Kh. Abu WardaNessuna valutazione finora
- Shavuot 5774Documento4 pagineShavuot 5774Andrea KingNessuna valutazione finora
- Cloudsoc For Amazon Web Services Solution Overview enDocumento6 pagineCloudsoc For Amazon Web Services Solution Overview enmanishNessuna valutazione finora
- Cottonhill - Red Collection PDFDocumento33 pagineCottonhill - Red Collection PDFVioricaNessuna valutazione finora
- Causes & Prevention of Coronary Artery DiseaseDocumento41 pagineCauses & Prevention of Coronary Artery DiseaseeenagpurcongNessuna valutazione finora
- Soil Loss EstimationDocumento77 pagineSoil Loss Estimationmys85Nessuna valutazione finora
- AHG-003 Guideline On GHG Accounting and Reporting 1junDocumento16 pagineAHG-003 Guideline On GHG Accounting and Reporting 1junbagjabuktiNessuna valutazione finora
- AP000100 EngDocumento9 pagineAP000100 EngLucas WrightNessuna valutazione finora
- The Baking and Frozen Dough MarketDocumento4 pagineThe Baking and Frozen Dough MarketMilling and Grain magazineNessuna valutazione finora
- 1.4 Market FailureDocumento42 pagine1.4 Market FailureRuban PaulNessuna valutazione finora
- Surface BOP Kill SheetDocumento12 pagineSurface BOP Kill Sheetzouke2002Nessuna valutazione finora
- PRECOMMISSIONING and COMMISSIONING PROCEDURE FOR CARD ACCESS CONTROL SYSTEMDocumento3 paginePRECOMMISSIONING and COMMISSIONING PROCEDURE FOR CARD ACCESS CONTROL SYSTEMHumaid ShaikhNessuna valutazione finora
- HPAD 201 Sat Days 2 and 3Documento11 pagineHPAD 201 Sat Days 2 and 3Arianne A ZamoraNessuna valutazione finora
- Humiseal Thinner 73 MSDSDocumento3 pagineHumiseal Thinner 73 MSDSibnu Groho Herry sampurnoNessuna valutazione finora
- Chem For Engineering Material by Pup BuddiesDocumento46 pagineChem For Engineering Material by Pup BuddiesJedidiah MondaresNessuna valutazione finora
- Spez KR QUANTEC Prime enDocumento155 pagineSpez KR QUANTEC Prime enDave FansolatoNessuna valutazione finora
- Forensic Science Project Group B5518Documento5 pagineForensic Science Project Group B5518Anchit JassalNessuna valutazione finora
- Grade 3 Science: PlantsDocumento5 pagineGrade 3 Science: PlantsMauie Flores100% (3)
- The Evolution of FungiDocumento15 pagineThe Evolution of Fungi2010eon2010Nessuna valutazione finora
- Courses at NeevDocumento10 pagineCourses at NeevDr Mohan SavadeNessuna valutazione finora
- Gretton, Hare, Catchpole - Psychopathy and Offending From Adolescence To Adulthood - A 10-Year Follow-UpDocumento10 pagineGretton, Hare, Catchpole - Psychopathy and Offending From Adolescence To Adulthood - A 10-Year Follow-UpMaria Isabel Trujillo MayaNessuna valutazione finora
- Respiratory Epithelium: Human Histology Lecture Chapter 17 Ï The Respiratory SystemDocumento16 pagineRespiratory Epithelium: Human Histology Lecture Chapter 17 Ï The Respiratory SystemEvandie OngNessuna valutazione finora
- Cooking - Sauces and Marinade RecipesDocumento96 pagineCooking - Sauces and Marinade Recipesagape_1st7100% (3)
- Cyclopropane, Ethynyl - (Cas 6746-94-7) MSDS: CyclopropylacetyleneDocumento5 pagineCyclopropane, Ethynyl - (Cas 6746-94-7) MSDS: CyclopropylacetyleneMiMi JoyNessuna valutazione finora
- Sugar Crisis in Pakistan Research PaperDocumento10 pagineSugar Crisis in Pakistan Research Paperrehan9891Nessuna valutazione finora
- Boge Screw UsaDocumento40 pagineBoge Screw UsaAir Repair, LLC100% (1)
- Reglas para Añadir Al Verbo Principal: Am Is Are ReadDocumento8 pagineReglas para Añadir Al Verbo Principal: Am Is Are ReadBrandon Sneider Garcia AriasNessuna valutazione finora
- Developmental Psychology - Socioemotional Development in Middle & Late ChildhoodDocumento56 pagineDevelopmental Psychology - Socioemotional Development in Middle & Late ChildhoodAlyNessuna valutazione finora