Potrebbero piacerti anche
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- 2021 SAISD Mask Mandate-LetterheadDocumento2 pagine2021 SAISD Mask Mandate-LetterheadDavid IbanezNessuna valutazione finora
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Cardiff PacesDocumento26 pagineCardiff PacesIvyljn100% (2)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- Hancock County Needs Assessment 1Documento20 pagineHancock County Needs Assessment 1api-622005669Nessuna valutazione finora
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- Slowther and Kleinman - ConfidentialityDocumento4 pagineSlowther and Kleinman - ConfidentialitysugarmelodiesNessuna valutazione finora
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- NSTP Act2 Suan, Allyna ChantalDocumento8 pagineNSTP Act2 Suan, Allyna ChantalChan TalNessuna valutazione finora
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- Identification of Exudates in InflammationDocumento5 pagineIdentification of Exudates in InflammationAnna AzukiNessuna valutazione finora
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- Total Abdominal Hysterectomy Bilateral Salpingo Oophorectomy (Tahbso) Nursing Responsibilities Rationale Pre-OperativeDocumento4 pagineTotal Abdominal Hysterectomy Bilateral Salpingo Oophorectomy (Tahbso) Nursing Responsibilities Rationale Pre-OperativeMiar QuestNessuna valutazione finora
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- Delayed Growth and Development Assessment N.Diagnosis Inference Planning Intervention Rationale EvaluationDocumento2 pagineDelayed Growth and Development Assessment N.Diagnosis Inference Planning Intervention Rationale Evaluationkreny10Nessuna valutazione finora
- WHO TRS 961 EngDocumento440 pagineWHO TRS 961 Engkorde1100% (3)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Burns and InjuryDocumento27 pagineBurns and InjuryJane Ann Alolod100% (1)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- MS GuldaneDocumento22 pagineMS GuldaneKhyy SafitryNessuna valutazione finora
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- TuberculosisDocumento4 pagineTuberculosisdreamxtreme16100% (2)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- Transoral Laser MicrosurgeryDocumento4 pagineTransoral Laser MicrosurgeryanniebuhrNessuna valutazione finora
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (74)
- American Indian: Health DisparitiesDocumento13 pagineAmerican Indian: Health DisparitiesDarwinso AlvarezNessuna valutazione finora
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- President Ramon Magsaysay State University: Sagutin Mo Ko! PANUTO: Sagutin Ang Mga Sumusunod Na KatanunganDocumento4 paginePresident Ramon Magsaysay State University: Sagutin Mo Ko! PANUTO: Sagutin Ang Mga Sumusunod Na KatanunganAndrea AngelicaNessuna valutazione finora
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- Antibiotic Resistance Among Uropathogenic Escherichia ColiDocumento13 pagineAntibiotic Resistance Among Uropathogenic Escherichia ColiSyed AmanNessuna valutazione finora
- Celiac Disease: DR Ajeet Kumar Lohana Senior Registrar Gastroenterology AtmcDocumento59 pagineCeliac Disease: DR Ajeet Kumar Lohana Senior Registrar Gastroenterology AtmcAjeet LohanaNessuna valutazione finora
- The Prevention and Management of Pressure UlcerDocumento5 pagineThe Prevention and Management of Pressure UlcerrantiNessuna valutazione finora
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- Physical Exam For PneumoniaDocumento3 paginePhysical Exam For PneumoniaAnna SłońskaNessuna valutazione finora
- Migraine Diaries PDFDocumento4 pagineMigraine Diaries PDFDr.Gopinath SaravananNessuna valutazione finora
- Probiotics Downloadable PDFDocumento2 pagineProbiotics Downloadable PDFGreg WrightNessuna valutazione finora
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- SDMS ID: P2010/0482-001 2.7-07WACS Title: Oxytocin (Syntocinon) InfusionDocumento5 pagineSDMS ID: P2010/0482-001 2.7-07WACS Title: Oxytocin (Syntocinon) InfusionYwagar YwagarNessuna valutazione finora
- Cleft Lip and PalateDocumento25 pagineCleft Lip and PalateRahul Dhaker100% (1)
- How To Kill Ticks On DogsDocumento3 pagineHow To Kill Ticks On DogsPhelan LoweNessuna valutazione finora
- Community Health Nursing Services in The Philippines PDFDocumento2 pagineCommunity Health Nursing Services in The Philippines PDFEdgar0% (3)
- Lecture-25 Cesarean SectionDocumento21 pagineLecture-25 Cesarean SectionMadhu Sudhan PandeyaNessuna valutazione finora
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- Personal Accident BrochureDocumento2 paginePersonal Accident BrochureAmar DixitNessuna valutazione finora
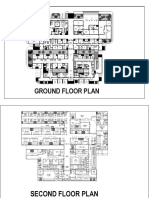
- Sample Plan HospitalDocumento3 pagineSample Plan HospitalMarkNova100% (1)
- A SphygmomanometerDocumento3 pagineA Sphygmomanometerdeepesh288Nessuna valutazione finora
- Antenatal Assessment - Case No-1Documento4 pagineAntenatal Assessment - Case No-1Prity DeviNessuna valutazione finora
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)