Potrebbero piacerti anche
- Schema Therapy Conceptualization of Personality Functioning and Traits in ICD 11 and DSM 5Documento12 pagineSchema Therapy Conceptualization of Personality Functioning and Traits in ICD 11 and DSM 5María González MartínNessuna valutazione finora
- PDM Manual Provides Comprehensive Psychodynamic DiagnosisDocumento6 paginePDM Manual Provides Comprehensive Psychodynamic Diagnosisas9as9as9as9Nessuna valutazione finora
- The Psychodynamic Diagnostic ManualDocumento6 pagineThe Psychodynamic Diagnostic ManuallukasNessuna valutazione finora
- P02 - An Integrative Approach To PsychopathologyDocumento30 pagineP02 - An Integrative Approach To PsychopathologyTEOFILO PALSIMON JR.Nessuna valutazione finora
- Gangguan BipolarDocumento9 pagineGangguan BipolarNaomiNessuna valutazione finora
- Recommendations for CHC FactorsDocumento5 pagineRecommendations for CHC FactorsJanie Ruth Green100% (1)
- Psychoanalysis AlexythimiaDocumento36 paginePsychoanalysis AlexythimiaJimy Moskuna100% (1)
- MCMI-III Victor LalhmangaihkimaDocumento12 pagineMCMI-III Victor LalhmangaihkimaVictor YanafNessuna valutazione finora
- Psychopharmacology Drugs The Brain and Be - 59efdf1c1723dd1190c6bd52Documento5 paginePsychopharmacology Drugs The Brain and Be - 59efdf1c1723dd1190c6bd52Sukanya SubramaniyanNessuna valutazione finora
- Prodromal SchizophreniaDocumento13 pagineProdromal SchizophreniadizhalfaNessuna valutazione finora
- Clinical Rating Scales in Suicide AssessmentDocumento8 pagineClinical Rating Scales in Suicide AssessmentCarol Artigas GómezNessuna valutazione finora
- Steiner, J. (1994) - Patient-Centered and Analyst-Centered Interpretations. Some Implications of Containment and CountertransferenceDocumento9 pagineSteiner, J. (1994) - Patient-Centered and Analyst-Centered Interpretations. Some Implications of Containment and CountertransferenceJulián Alberto Muñoz FigueroaNessuna valutazione finora
- Rorschach Interpretation Susan Himelstein, Ph.D. - Meet The Faculty ...Documento40 pagineRorschach Interpretation Susan Himelstein, Ph.D. - Meet The Faculty ...michoxNessuna valutazione finora
- Assessment of Personality DisorderDocumento19 pagineAssessment of Personality DisorderTanyu Mbuli TidolineNessuna valutazione finora
- A Filled-In Example: Schema Therapy Case Conceptualization FormDocumento10 pagineA Filled-In Example: Schema Therapy Case Conceptualization FormKarinaNessuna valutazione finora
- Personality Assessment in Treatment Planning PDFDocumento259 paginePersonality Assessment in Treatment Planning PDFrezasattariNessuna valutazione finora
- Mental StatusDocumento6 pagineMental StatusIgor Oliveira100% (1)
- Psychoeducation: 19 July 2018 Unit VI Topic DiscussionDocumento26 paginePsychoeducation: 19 July 2018 Unit VI Topic DiscussionDana Franklin100% (1)
- Attachment, Mentalization, and the Development of the SelfDocumento33 pagineAttachment, Mentalization, and the Development of the SelfSantiago Osorio MoralesNessuna valutazione finora
- MMPI-3 GuidelinesDocumento82 pagineMMPI-3 Guidelinesclaudia carrera100% (4)
- Otto Kernberg's Object Relations TheoryDocumento25 pagineOtto Kernberg's Object Relations TheoryHannah HolandaNessuna valutazione finora
- 2016 - Psychiatric SymptomsDocumento164 pagine2016 - Psychiatric SymptomsCristina100% (1)
- Psychotherapeutic Strategies in The Latency YearsDocumento590 paginePsychotherapeutic Strategies in The Latency YearsCarmen SpirescuNessuna valutazione finora
- Introduction To The Special Section On Attachment Theory and PsychotherapyDocumento5 pagineIntroduction To The Special Section On Attachment Theory and PsychotherapyMichaeilaNessuna valutazione finora
- Mmpi-3 Sample Interpretive ReportDocumento20 pagineMmpi-3 Sample Interpretive ReportMohammad Hassan Haji Hosseini100% (1)
- K-GSADS-A - Package Posible Prueba para Medir SOCIAL PHOBIADocumento16 pagineK-GSADS-A - Package Posible Prueba para Medir SOCIAL PHOBIABetsyNessuna valutazione finora
- Overcome Anxiety with Adlerian TherapyDocumento14 pagineOvercome Anxiety with Adlerian TherapyEarl EhimplarNessuna valutazione finora
- 2 MMPI-2 Validity-Scales Final PDFDocumento9 pagine2 MMPI-2 Validity-Scales Final PDFHanifa Bi BaritoNessuna valutazione finora
- Psychodynamic Diagnostic Manual, Second Edition: PDM-2Documento5 paginePsychodynamic Diagnostic Manual, Second Edition: PDM-2gysedyte0% (6)
- Winnicot Hate and Transitional ObjectsDocumento28 pagineWinnicot Hate and Transitional ObjectsAmbrose66Nessuna valutazione finora
- Markowitz PPD IptDocumento4 pagineMarkowitz PPD IptIoana BocaNessuna valutazione finora
- Types of PsychotherapiesDocumento2 pagineTypes of PsychotherapiesJulie VictorianoNessuna valutazione finora
- Zuchowski Assessment ReportDocumento7 pagineZuchowski Assessment Reportapi-532093342Nessuna valutazione finora
- Y Bocs Information SampleDocumento2 pagineY Bocs Information SampledevNessuna valutazione finora
- DASI EnglishDocumento96 pagineDASI Englishfionachappell79100% (1)
- Psychotherapy of Depression in Children and AdolescentsDocumento58 paginePsychotherapy of Depression in Children and AdolescentsYamila Borges Rivera100% (1)
- Linking Assessment and TreatmentDocumento37 pagineLinking Assessment and Treatmentaimee2oo8Nessuna valutazione finora
- BPRS Manual: Guide to Administering the Brief Psychiatric Rating ScaleDocumento29 pagineBPRS Manual: Guide to Administering the Brief Psychiatric Rating ScaleNungki TriandariNessuna valutazione finora
- Validity R:: All Descriptive Statistics Presented in This Handout Are For An Adult Nonpatient Population (Table 1)Documento40 pagineValidity R:: All Descriptive Statistics Presented in This Handout Are For An Adult Nonpatient Population (Table 1)Marina SwansonNessuna valutazione finora
- Neuropsychological AssessmentDocumento6 pagineNeuropsychological AssessmentAkhwand Saulat100% (1)
- Borderline Personality Disorder, Kernberg & MichelsDocumento4 pagineBorderline Personality Disorder, Kernberg & MichelsMarietta_Monari100% (1)
- Women in Psychology - Margaret MahlerDocumento7 pagineWomen in Psychology - Margaret MahlerNadia ShinkewiczNessuna valutazione finora
- Cognitive Model of Postnatal DepressionDocumento1 paginaCognitive Model of Postnatal Depressionchrispalmer21Nessuna valutazione finora
- The Broad Scope of Ego Function Assessment (Leopold Bellak, Lisa Goldsmith) PDFDocumento605 pagineThe Broad Scope of Ego Function Assessment (Leopold Bellak, Lisa Goldsmith) PDFAmbrose66100% (1)
- Case Vignette 1Documento3 pagineCase Vignette 1api-312964081Nessuna valutazione finora
- Childhood Emotional DevelopmentDocumento27 pagineChildhood Emotional DevelopmentAbegail RuizNessuna valutazione finora
- The Unstructured Clinical InterviewDocumento8 pagineThe Unstructured Clinical Interviewkasmiantoabadi100% (1)
- Suneeta Monga, Diane Benoit - Assessing and Treating Anxiety Disorders in Young Children - The Taming Sneaky Fears Program-Springer International Publishing (2018)Documento228 pagineSuneeta Monga, Diane Benoit - Assessing and Treating Anxiety Disorders in Young Children - The Taming Sneaky Fears Program-Springer International Publishing (2018)OlharapoNessuna valutazione finora
- MoCA 7.2 ScoringDocumento5 pagineMoCA 7.2 Scoringszhou52100% (2)
- Thepsychodynamic Treatmentofborderline Personalitydisorder: An Introduction To Transference-Focused PsychotherapyDocumento17 pagineThepsychodynamic Treatmentofborderline Personalitydisorder: An Introduction To Transference-Focused PsychotherapyDonald Cabrera AstudilloNessuna valutazione finora
- Delgado, S. V., Strawn, J. R., & Pedapati, E. V. (2015) - Contemporary Psychodynamic Psychotherapy For Children and Adolescents PDFDocumento398 pagineDelgado, S. V., Strawn, J. R., & Pedapati, E. V. (2015) - Contemporary Psychodynamic Psychotherapy For Children and Adolescents PDFMarcoBalzariniNessuna valutazione finora
- CLIENT VARIABLES and Psychotherapy OutcomesDocumento20 pagineCLIENT VARIABLES and Psychotherapy OutcomespsicandreiaNessuna valutazione finora
- Panss ScoreDocumento8 paginePanss ScoretriaclaresiaNessuna valutazione finora
- WINNICOTT, Donald W. - 1974.-Fear-of-Breakdown.-International-Review-of-Psychoanalysis.-1-103-7 PDFDocumento5 pagineWINNICOTT, Donald W. - 1974.-Fear-of-Breakdown.-International-Review-of-Psychoanalysis.-1-103-7 PDFFelipe Garzon SutNessuna valutazione finora
- Lesson 2 The Skills Activities of A Clinical PsychologistDocumento6 pagineLesson 2 The Skills Activities of A Clinical PsychologistReg RoseteNessuna valutazione finora
- A Comparison of The Emotional Indicators On The House-Tree-Person PDFDocumento214 pagineA Comparison of The Emotional Indicators On The House-Tree-Person PDFKrisdaryadiHadisubroto100% (1)
- 433 Psychiatry Team Child PsychiatryDocumento10 pagine433 Psychiatry Team Child PsychiatrySherlina Rintik Tirta AyuNessuna valutazione finora
- The Structural Approach in Psychological Testing: Pergamon General Psychology SeriesDa EverandThe Structural Approach in Psychological Testing: Pergamon General Psychology SeriesNessuna valutazione finora
- Principles of Psychotherapy: Promoting Evidence-Based Psychodynamic PracticeDa EverandPrinciples of Psychotherapy: Promoting Evidence-Based Psychodynamic PracticeNessuna valutazione finora
- Integrating Clinical and Empirical Perspectives On Personality: The Shedler-Westen Assessment Procedure (Swap)Documento28 pagineIntegrating Clinical and Empirical Perspectives On Personality: The Shedler-Westen Assessment Procedure (Swap)gustiNessuna valutazione finora
- WhodasDocumento152 pagineWhodasChristopher Oneil100% (2)
- Hierarchical Personality Assessment CostaMcCrae1995Documento30 pagineHierarchical Personality Assessment CostaMcCrae1995vath23Nessuna valutazione finora
- The Barnum Effect in Personality Assessment A Review of The LiteratureDocumento16 pagineThe Barnum Effect in Personality Assessment A Review of The LiteraturegustiNessuna valutazione finora
- Talking As Dreaming. OgdenDocumento16 pagineTalking As Dreaming. OgdenMariane NotoNessuna valutazione finora
- Pathological Narcissism and Narcissistic Personality DisorderDocumento26 paginePathological Narcissism and Narcissistic Personality DisorderLyd Pensado100% (2)
- Play Therapy and Behavior Modification in ChildrenDocumento4 paginePlay Therapy and Behavior Modification in ChildrenMonina JonesNessuna valutazione finora
- New Freedom Ops LLC Iop P&PDocumento51 pagineNew Freedom Ops LLC Iop P&Pmike iovinoNessuna valutazione finora
- Managing Psychological ProblemsDocumento2 pagineManaging Psychological ProblemsAdrian LagascaNessuna valutazione finora
- NCMH Perfomance Eval Tool (1) .Xls PERF. CHECKLIST (PI)Documento4 pagineNCMH Perfomance Eval Tool (1) .Xls PERF. CHECKLIST (PI)JAN MARIELLE GALLARDENessuna valutazione finora
- The Civil War Inside My BrainDocumento5 pagineThe Civil War Inside My BrainTony BlairNessuna valutazione finora
- 4 Middle School Tips - Social and Emotional DevelopmentDocumento4 pagine4 Middle School Tips - Social and Emotional DevelopmentOrne PuricelliNessuna valutazione finora
- Posha S Comparisons 2011Documento6 paginePosha S Comparisons 2011Andreia TavaresNessuna valutazione finora
- (고1 3월) 2022+3월+고1+변형문제+abridgedDocumento23 pagine(고1 3월) 2022+3월+고1+변형문제+abridgedo6oeeoNessuna valutazione finora
- An Interactional Description of SchizophreniaDocumento13 pagineAn Interactional Description of SchizophreniaPatricio Batana100% (1)
- Pop Quiz CharacterizationDocumento5 paginePop Quiz CharacterizationRoanne MendozaNessuna valutazione finora
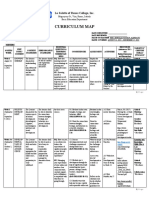
- Curriculum Map: La Salette of Roxas College, IncDocumento7 pagineCurriculum Map: La Salette of Roxas College, IncCzarina Ciara AndresNessuna valutazione finora
- Licerio Antiporda Sr. National High School - Dalaya Annex: Review of Related LiteratureDocumento4 pagineLicerio Antiporda Sr. National High School - Dalaya Annex: Review of Related Literatureadrianpaul villenaNessuna valutazione finora
- International Classification of Diseases - 10 Edition: Presentation By-Saloni Punya Akanksha FarheenDocumento16 pagineInternational Classification of Diseases - 10 Edition: Presentation By-Saloni Punya Akanksha FarheenAakanksha VermaNessuna valutazione finora
- Many Musicians and Performers Make A Distinction BDocumento3 pagineMany Musicians and Performers Make A Distinction BHassan MaqsoodNessuna valutazione finora
- Please Return The Completed Referral Form byDocumento5 paginePlease Return The Completed Referral Form byA AkbNessuna valutazione finora
- A Presentation On Student Discipline at New Hanover County Schools To Be Given On May 2, 2023Documento23 pagineA Presentation On Student Discipline at New Hanover County Schools To Be Given On May 2, 2023Jamie BouletNessuna valutazione finora
- Peer Support For PeopleDocumento120 paginePeer Support For Peoplebraulio rojasNessuna valutazione finora
- Q ERI - Psychometric-SiegristDocumento14 pagineQ ERI - Psychometric-Siegristshashank shuklaNessuna valutazione finora
- Statement of Purpose (MHA) Gannon UniversityDocumento3 pagineStatement of Purpose (MHA) Gannon UniversitySheikh Shafiq SiamNessuna valutazione finora
- Guide For Integration of Perinatal Mental Health in Maternal and Child Health ServicesDocumento66 pagineGuide For Integration of Perinatal Mental Health in Maternal and Child Health ServicesJudit Cos BusquetsNessuna valutazione finora
- Vsim David Carter Part 2 PDFDocumento5 pagineVsim David Carter Part 2 PDFJennifer Adviento100% (1)
- Integrating Behavioral Health Into The Medical Home A Rapid Implementation Guide 1st Edition Ebook PDFDocumento53 pagineIntegrating Behavioral Health Into The Medical Home A Rapid Implementation Guide 1st Edition Ebook PDFteresa.vanhorn907100% (42)
- g12 - Mock Test 38Documento4 pagineg12 - Mock Test 38Hải YếnNessuna valutazione finora
- Evidence Based Practice - CookingDocumento4 pagineEvidence Based Practice - Cookingapi-578165683Nessuna valutazione finora
- Dr. Bob DeMaria, The Drugless Doctor, Releases His Eleventh Book, "Dr. Bob's Drugless Guide To Mental Health," For Mental Health Awareness MonthDocumento3 pagineDr. Bob DeMaria, The Drugless Doctor, Releases His Eleventh Book, "Dr. Bob's Drugless Guide To Mental Health," For Mental Health Awareness MonthPR.comNessuna valutazione finora
- Review of Related LiteratureDocumento5 pagineReview of Related LiteratureCake ManNessuna valutazione finora
- Understanding the Self and Red Flags of Unhealthy RelationshipsDocumento3 pagineUnderstanding the Self and Red Flags of Unhealthy RelationshipsMica Krizel Javero MercadoNessuna valutazione finora
- Factors Leading to Mental Illness in High School StudentsDocumento13 pagineFactors Leading to Mental Illness in High School StudentsBea MalagambaNessuna valutazione finora