Potrebbero piacerti anche
- Advanced Techniques For Solution Focused CounselingDocumento23 pagineAdvanced Techniques For Solution Focused CounselingFrank Smith100% (3)
- Final Program PlanDocumento20 pagineFinal Program Planapi-547392304100% (1)
- Antepartum Record Labor WatchDocumento4 pagineAntepartum Record Labor WatchMaryJoy rosalesNessuna valutazione finora
- CerebrolysinDocumento3 pagineCerebrolysinMelissa Fatima Laurente Dosdos100% (2)
- Agricultural Engeeniring Thesis KSUDocumento80 pagineAgricultural Engeeniring Thesis KSUjingky SallicopNessuna valutazione finora
- Capstone Paper - FinalDocumento13 pagineCapstone Paper - Finalapi-29112217450% (2)
- Proposed NFPA 1851 Decision TreeDocumento2 pagineProposed NFPA 1851 Decision Treeepraetorian100% (1)
- Childhood Obesity Apa PaperDocumento13 pagineChildhood Obesity Apa Paperapi-3018616020% (1)
- Literature Review FinalDocumento11 pagineLiterature Review Finalapi-253949835Nessuna valutazione finora
- Sample Research Paper On Childhood ObesityDocumento8 pagineSample Research Paper On Childhood Obesitygw13qds8100% (1)
- Techmemo9 4aDocumento3 pagineTechmemo9 4aapi-283086678Nessuna valutazione finora
- Research Paper On Childhood Obesity PDFDocumento4 pagineResearch Paper On Childhood Obesity PDFzhzafmhkf100% (1)
- Research Paper On Childhood Obesity and Fast FoodDocumento6 pagineResearch Paper On Childhood Obesity and Fast Foodugmhvdulg100% (1)
- Childhood Obesity Research Paper MlaDocumento6 pagineChildhood Obesity Research Paper Mladyf0g0h0fap3100% (1)
- Thesis Statement Examples On Childhood ObesityDocumento8 pagineThesis Statement Examples On Childhood Obesityjaclyncreedonannarbor100% (2)
- International Childhood Obesity Prevention StrategiesDocumento12 pagineInternational Childhood Obesity Prevention StrategiesMarkNessuna valutazione finora
- Literature Review Brief Interventions and Childhood ObesityDocumento7 pagineLiterature Review Brief Interventions and Childhood ObesityozbvtcvkgNessuna valutazione finora
- 16 01 ExecsummaryDocumento2 pagine16 01 Execsummaryapi-255677957Nessuna valutazione finora
- Reversing The Trend of Childhood ObesityDocumento6 pagineReversing The Trend of Childhood ObesitySharon V.Nessuna valutazione finora
- Good Thesis Statement For Child ObesityDocumento7 pagineGood Thesis Statement For Child Obesityamandahengelfargo100% (2)
- Childhood Obesityfinal 2Documento12 pagineChildhood Obesityfinal 2api-260974225Nessuna valutazione finora
- Research Paper On Obesity in The WorkplaceDocumento8 pagineResearch Paper On Obesity in The Workplacevvomvqwgf100% (1)
- Thesis Statement For Child ObesityDocumento4 pagineThesis Statement For Child ObesityWriteMyCustomPaperSingapore100% (1)
- Introduction For A Research Paper On ObesityDocumento7 pagineIntroduction For A Research Paper On Obesityqosryjvnd100% (1)
- 10 Page Research Paper On ObesityDocumento5 pagine10 Page Research Paper On Obesityyvunfevgf100% (1)
- Literature Review Article On Childhood ObesityDocumento8 pagineLiterature Review Article On Childhood Obesityc5qvf1q1100% (1)
- Childhood Obesity Research Paper QuestionsDocumento7 pagineChildhood Obesity Research Paper Questionsafnhicafcspyjh100% (1)
- Apa Research Paper On Child ObesityDocumento6 pagineApa Research Paper On Child Obesitylqinlccnd100% (1)
- Childhood Obesity Research Paper ExampleDocumento5 pagineChildhood Obesity Research Paper Examplecakvaw0q100% (1)
- Obesity in America Term PaperDocumento4 pagineObesity in America Term Paperafdtfhtut100% (1)
- Selbrede Anna Synthesispaper 5 31Documento13 pagineSelbrede Anna Synthesispaper 5 31api-320307298Nessuna valutazione finora
- Obesity Term PaperDocumento4 pagineObesity Term Paperafmzndvyddcoio100% (1)
- Childhood Obesity Research Paper SampleDocumento4 pagineChildhood Obesity Research Paper Samplepxihigrif100% (1)
- Research Paper On Preventing Childhood ObesityDocumento7 pagineResearch Paper On Preventing Childhood Obesityphjaehhkf100% (1)
- Childhood Obesity in America Research PaperDocumento7 pagineChildhood Obesity in America Research Paperyvunfevgf100% (1)
- Example Thesis Statement For Childhood ObesityDocumento5 pagineExample Thesis Statement For Childhood Obesityfjda52j0100% (2)
- Example of Research Paper On Adolescent ObesityDocumento5 pagineExample of Research Paper On Adolescent Obesitygvzph2vh100% (1)
- Argumentative Research Paper On Child ObesityDocumento7 pagineArgumentative Research Paper On Child Obesityk0wyn0tykob3100% (1)
- Free Research Paper On Childhood ObesityDocumento4 pagineFree Research Paper On Childhood Obesityd0f1lowufam3100% (1)
- Term Paper ObesityDocumento8 pagineTerm Paper Obesityafmzahfnjwhaat100% (1)
- Thesis Statement Regarding Childhood ObesityDocumento7 pagineThesis Statement Regarding Childhood Obesityufagmcgld100% (1)
- Childhood Obesity Research Paper UkDocumento5 pagineChildhood Obesity Research Paper Ukxilllqwhf100% (1)
- Research Paper About ObesityDocumento6 pagineResearch Paper About Obesityxcjfderif100% (1)
- Preventing Childhood Obesity Through Family EducationDocumento15 paginePreventing Childhood Obesity Through Family EducationKiana TehraniNessuna valutazione finora
- Child Obesity Research Paper TopicsDocumento7 pagineChild Obesity Research Paper Topicsfzpabew4100% (1)
- Example Literature Review On Childhood ObesityDocumento6 pagineExample Literature Review On Childhood Obesityc5praq5p100% (1)
- Dissertation Obesity IdeasDocumento8 pagineDissertation Obesity IdeasCollegePaperWriterLittleRock100% (1)
- Childhood Obesity Dissertation UkDocumento4 pagineChildhood Obesity Dissertation UkBuyingPapersFrisco100% (1)
- Research Paper Over ObesityDocumento5 pagineResearch Paper Over Obesityyelbsyvkg100% (1)
- Obesity Thesis PDFDocumento8 pagineObesity Thesis PDFmariaparkslasvegas100% (2)
- What Would Be A Good Thesis Statement For Childhood ObesityDocumento7 pagineWhat Would Be A Good Thesis Statement For Childhood Obesityafcnhvyoc100% (2)
- ESSINGTON. Legislating Weight Loss. Are Antiobesity Public Health Policies Making An ImpactDocumento9 pagineESSINGTON. Legislating Weight Loss. Are Antiobesity Public Health Policies Making An ImpactNina NavajasNessuna valutazione finora
- Child Obesity Essay ThesisDocumento8 pagineChild Obesity Essay Thesisdwsjyt34100% (2)
- Research Paper On Childhood Obesity TopicsDocumento8 pagineResearch Paper On Childhood Obesity Topicsikofdvbnd100% (1)
- Thesis Statement For Childhood ObesityDocumento4 pagineThesis Statement For Childhood Obesitycourtneypetersonspringfield100% (2)
- Rhiannon Worker Possible Solutions of Childhood Obesity Arizona State University English 102Documento5 pagineRhiannon Worker Possible Solutions of Childhood Obesity Arizona State University English 102api-403496064Nessuna valutazione finora
- Thesis ObesityDocumento8 pagineThesis ObesityProfessionalPaperWritingServiceManchester100% (2)
- Research Paper Child ObesityDocumento4 pagineResearch Paper Child Obesitycar93zdy100% (1)
- Proposal Research Paper On Childhood ObesityDocumento4 pagineProposal Research Paper On Childhood Obesityegyey4bp100% (1)
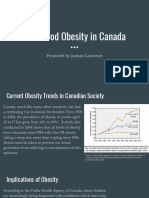
- Childhood Obesity in Canada: Presented by Jaiman LawrenceDocumento11 pagineChildhood Obesity in Canada: Presented by Jaiman LawrenceJaiman LawrenceNessuna valutazione finora
- Final Research Paper On Childhood ObesityDocumento4 pagineFinal Research Paper On Childhood Obesityafmcpdbnr100% (1)
- FinalinternshipproposalDocumento16 pagineFinalinternshipproposalapi-298341996Nessuna valutazione finora
- Good Thesis Statement About Childhood ObesityDocumento4 pagineGood Thesis Statement About Childhood Obesitydnqkxm09100% (2)
- What Is A Good Thesis Statement For Childhood ObesityDocumento8 pagineWhat Is A Good Thesis Statement For Childhood ObesityBuyCustomPapersOnlineChicago100% (1)
- Childhood Obesity: Causes, Consequences and Prevention ApproachesDa EverandChildhood Obesity: Causes, Consequences and Prevention ApproachesNessuna valutazione finora
- Yield Performance of TomatoDocumento71 pagineYield Performance of Tomatojingky SallicopNessuna valutazione finora
- English: Quarter 1 - Module 1: Unity Within!Documento35 pagineEnglish: Quarter 1 - Module 1: Unity Within!Helen Lanzuela-ManalotoNessuna valutazione finora
- VolleyballDocumento1 paginaVolleyballjingky SallicopNessuna valutazione finora
- Ilocos Norte Tourist SpotDocumento8 pagineIlocos Norte Tourist Spotjingky SallicopNessuna valutazione finora
- Mga Kulturang Pilipino Sa Panahon NG KatutuboDocumento12 pagineMga Kulturang Pilipino Sa Panahon NG Katutubojingky SallicopNessuna valutazione finora
- Eng4 q1 Mod2 Get To Know It Final08032020Documento35 pagineEng4 q1 Mod2 Get To Know It Final08032020jingky SallicopNessuna valutazione finora
- ACFrOgAzVG78oBgEdkRlo77Ir8wqUvVpLAjgxOTLYAewh660EF42CwmPdvZUqpf2pPsJ9itcl0gF2J0D6vzoSjiWKkQ6JrO479laUUTibLn6xJ 0cUBAkwwHNxJ0Cwawq FDN4NyU-B5T4qRfGbWDocumento12 pagineACFrOgAzVG78oBgEdkRlo77Ir8wqUvVpLAjgxOTLYAewh660EF42CwmPdvZUqpf2pPsJ9itcl0gF2J0D6vzoSjiWKkQ6JrO479laUUTibLn6xJ 0cUBAkwwHNxJ0Cwawq FDN4NyU-B5T4qRfGbWjingky SallicopNessuna valutazione finora
- Advance Biology SpupDocumento2 pagineAdvance Biology Spupjingky SallicopNessuna valutazione finora
- ASSIGNMENT in PharmacueticalDocumento3 pagineASSIGNMENT in Pharmacueticaljingky SallicopNessuna valutazione finora
- Weekly OTSIC Report from Balbalan Municipal Police StationDocumento3 pagineWeekly OTSIC Report from Balbalan Municipal Police Stationjingky SallicopNessuna valutazione finora
- Methods of Processing Fruits and VegetablesDocumento11 pagineMethods of Processing Fruits and Vegetablesjingky SallicopNessuna valutazione finora
- BatoyDocumento12 pagineBatoyjingky SallicopNessuna valutazione finora
- Artist and ArtisanDocumento3 pagineArtist and Artisanjingky SallicopNessuna valutazione finora
- Broken Dream by ChristyDocumento7 pagineBroken Dream by Christyjingky SallicopNessuna valutazione finora
- Allubaggan Application LetterDocumento1 paginaAllubaggan Application Letterjingky SallicopNessuna valutazione finora
- Basketball Simple RulesDocumento14 pagineBasketball Simple Rulesjingky SallicopNessuna valutazione finora
- Weekly OTSIC Report from Balbalan Municipal Police StationDocumento3 pagineWeekly OTSIC Report from Balbalan Municipal Police Stationjingky SallicopNessuna valutazione finora
- AffidavitDocumento1 paginaAffidavitjingky SallicopNessuna valutazione finora
- Certification Vinalyn04172019Documento1 paginaCertification Vinalyn04172019jingky SallicopNessuna valutazione finora
- ACIDS and BasesDocumento3 pagineACIDS and Basesjingky SallicopNessuna valutazione finora
- ,furnitureDocumento121 pagine,furniturejingky SallicopNessuna valutazione finora
- Adrience GacayanDocumento26 pagineAdrience Gacayanjingky SallicopNessuna valutazione finora
- ACKNOWLEDGEMETNDocumento1 paginaACKNOWLEDGEMETNjingky SallicopNessuna valutazione finora
- Weekly OTSIC Report from Balbalan Municipal Police StationDocumento3 pagineWeekly OTSIC Report from Balbalan Municipal Police Stationjingky SallicopNessuna valutazione finora
- Ang Pasko Ay SumapitDocumento8 pagineAng Pasko Ay Sumapitjingky SallicopNessuna valutazione finora
- Weekly OTSIC Report from Balbalan Municipal Police StationDocumento3 pagineWeekly OTSIC Report from Balbalan Municipal Police Stationjingky SallicopNessuna valutazione finora
- TorrusDocumento1 paginaTorrusjingky SallicopNessuna valutazione finora
- Absolute Deed of Sale GLORIA REGINO150KDocumento1 paginaAbsolute Deed of Sale GLORIA REGINO150Kjingky SallicopNessuna valutazione finora
- Kalinga State University: College of Public Administration and Indigenous GovernanceDocumento10 pagineKalinga State University: College of Public Administration and Indigenous Governancejingky SallicopNessuna valutazione finora
- Experience: Operations ManagerDocumento3 pagineExperience: Operations ManagerBimo Adlian SNessuna valutazione finora
- Essay 3 Final DraftDocumento8 pagineEssay 3 Final Draftapi-270571146Nessuna valutazione finora
- Journal Pre-Proof: American Journal of Kidney DiseasesDocumento27 pagineJournal Pre-Proof: American Journal of Kidney DiseasesGabriel Felipe CGNessuna valutazione finora
- Uganda Universities and Courses For Student Loan SupportDocumento5 pagineUganda Universities and Courses For Student Loan SupportThe Campus TimesNessuna valutazione finora
- Causes and Effects of Teacher BurnoutDocumento3 pagineCauses and Effects of Teacher BurnoutArif AkmalNessuna valutazione finora
- Janani Suraksha Yojana (JSY) (J) : State Institute of Health & Family Welfare, JaipurDocumento39 pagineJanani Suraksha Yojana (JSY) (J) : State Institute of Health & Family Welfare, JaipurvipinyadavkumarNessuna valutazione finora
- Spider AngiomaDocumento5 pagineSpider AngiomaVishal SharmaNessuna valutazione finora
- Concept of Stress and Psychological Adaptation To StressDocumento12 pagineConcept of Stress and Psychological Adaptation To Stressvaideeswari kumarNessuna valutazione finora
- 10 WinterDocumento48 pagine10 WintercontinentdriftNessuna valutazione finora
- Professional Adjustment in NursingDocumento47 pagineProfessional Adjustment in NursingAnning HagarNessuna valutazione finora
- Preventive Medicine Reports: Michael E. Rezaee, Charlotte E. Ward, Einar F. Sverrisson, Lawrence M. DagrosaDocumento4 paginePreventive Medicine Reports: Michael E. Rezaee, Charlotte E. Ward, Einar F. Sverrisson, Lawrence M. DagrosaJoko MardiyonoNessuna valutazione finora
- NZREX Bridging Programme OverviewDocumento12 pagineNZREX Bridging Programme OverviewGus LionsNessuna valutazione finora
- "Physiological Monitoring and Device Interface": Report by Jawia Mustapha BSN2-ADocumento21 pagine"Physiological Monitoring and Device Interface": Report by Jawia Mustapha BSN2-ADimple AnticamaraNessuna valutazione finora
- Coronavirus Infographics (NSTP)Documento1 paginaCoronavirus Infographics (NSTP)Sedric VillanuevaNessuna valutazione finora
- Comparative Study Between Swiss Ball and Theraband Exercises On Overweight IndividualsDocumento42 pagineComparative Study Between Swiss Ball and Theraband Exercises On Overweight Individualssundar_kumar0Nessuna valutazione finora
- Pengetahuan Ergonomi Dan Postur Kerja Perawat Pada Perawatan Luka Dengan Gangguan Muskuloskeletal Di Dr. H. Koesnadi BondowosoDocumento5 paginePengetahuan Ergonomi Dan Postur Kerja Perawat Pada Perawatan Luka Dengan Gangguan Muskuloskeletal Di Dr. H. Koesnadi BondowosoImanuel SihotangNessuna valutazione finora
- Sample Paper 2 Iatf Protocol1Documento103 pagineSample Paper 2 Iatf Protocol1Tiny Grace PalgueNessuna valutazione finora
- NCP Acute PainDocumento3 pagineNCP Acute PainSian Grace AsadaNessuna valutazione finora
- Case Report on Extravasation Injury from IV ClindamycinDocumento3 pagineCase Report on Extravasation Injury from IV ClindamycinmdthNessuna valutazione finora
- WHO MBHSS 2010 Section2 Web PDFDocumento20 pagineWHO MBHSS 2010 Section2 Web PDFDnrxsNessuna valutazione finora
- EDocumento375 pagineEANA MARIA CRISTIANANessuna valutazione finora
- Rare Sigmoid Abdominal Wall Fistula After Appendectomy: A Case ReportDocumento6 pagineRare Sigmoid Abdominal Wall Fistula After Appendectomy: A Case Reportjlcano1210Nessuna valutazione finora
- Eastern Connecticut State University Informed Consent Form: Participant's Printed NameDocumento4 pagineEastern Connecticut State University Informed Consent Form: Participant's Printed NameKisu Hive GamesNessuna valutazione finora
- Aorn Laser SafetyDocumento16 pagineAorn Laser SafetyAmanda RapaNessuna valutazione finora
- Bentonite MSDSDocumento3 pagineBentonite MSDSMohammed Ahmed NasherNessuna valutazione finora
- Sir Iqbal First PageDocumento7 pagineSir Iqbal First PageMozzam Ali ShahNessuna valutazione finora