Potrebbero piacerti anche
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- Family Therapy For Autism Spectrum Disorders (Cto)Documento21 pagineFamily Therapy For Autism Spectrum Disorders (Cto)Julie Rose AlboresNessuna valutazione finora
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (73)
- Lavender Lavender Lavender Lavender Lavender Lavender: UrineDocumento3 pagineLavender Lavender Lavender Lavender Lavender Lavender: UrineJonathan A. Sarmiento67% (6)
- Leukemia EssayDocumento4 pagineLeukemia EssaydanarajNessuna valutazione finora
- Hazardous Materials Management Plan SMDocumento26 pagineHazardous Materials Management Plan SMdarmayunitaNessuna valutazione finora
- Prepared by Muhammad Salman: This Brand Plan Has Been Designed For The ProductDocumento90 paginePrepared by Muhammad Salman: This Brand Plan Has Been Designed For The ProductMuhammad SalmanNessuna valutazione finora
- Paediatric Clerking SheetDocumento5 paginePaediatric Clerking SheetIamTinesh100% (2)
- MBLEx Practice ExamsDocumento268 pagineMBLEx Practice ExamsTrace Thuma100% (9)
- Masterfile Let ReviewerDocumento644 pagineMasterfile Let ReviewerApril Claire Pineda Manlangit50% (4)
- Tai Chi LiteratureDocumento2 pagineTai Chi LiteratureMichael Fong100% (1)
- An Industrial Training Report at Biogenetic Drugs PVT - Ltd. Baddi (H.P.)Documento26 pagineAn Industrial Training Report at Biogenetic Drugs PVT - Ltd. Baddi (H.P.)pankajsinghal27010% (2)
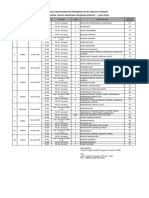
- Jadwal UAS PSSF Semester Ganjil 2019 2020 - Update 5 Des 2019Documento1 paginaJadwal UAS PSSF Semester Ganjil 2019 2020 - Update 5 Des 2019Rizky TriantoroNessuna valutazione finora
- I Was WrongDocumento5 pagineI Was WrongRizky TriantoroNessuna valutazione finora
- Use of Human Embryonic Stem Cells in The Treatment of Diabetes Mellitus: A Case SeriesDocumento6 pagineUse of Human Embryonic Stem Cells in The Treatment of Diabetes Mellitus: A Case SeriesAnonymous 7l69XWy12UNessuna valutazione finora
- ScoliosisDocumento1 paginaScoliosisRizky TriantoroNessuna valutazione finora
- Img20190901 07125078Documento1 paginaImg20190901 07125078Rizky TriantoroNessuna valutazione finora
- UVA QuestionsDocumento61 pagineUVA QuestionsjhhjjhNessuna valutazione finora
- Ethical Dilemmas in The Practice of NursingDocumento15 pagineEthical Dilemmas in The Practice of Nursingestudiant9Nessuna valutazione finora
- Corrected Ortho QsDocumento48 pagineCorrected Ortho QsMuhamad Danial Kholili Al-JaloriNessuna valutazione finora
- Pharma NotesDocumento69 paginePharma NotesJawad Ahmad100% (1)
- Anexo 3 Consenso de La Eskka en OsteoartritisDocumento58 pagineAnexo 3 Consenso de La Eskka en OsteoartritisgrimmNessuna valutazione finora
- Mpfwhitfieldsointment5 5Documento1 paginaMpfwhitfieldsointment5 5Dr.Ramkaran SainiNessuna valutazione finora
- PD 03-2020 PDFDocumento2 paginePD 03-2020 PDFtimvrghs123Nessuna valutazione finora
- BibliopocDocumento4 pagineBibliopocKarlo ReyesNessuna valutazione finora
- Oral 5Documento236 pagineOral 5Iodeh1985 OdehNessuna valutazione finora
- Red Biotechnology ProjectDocumento5 pagineRed Biotechnology ProjectMahendrakumar ManiNessuna valutazione finora
- Carrubba Botanical Guide RDocumento247 pagineCarrubba Botanical Guide Rafridikhanjan100% (3)
- Tinnitus EpidemiologyDocumento149 pagineTinnitus EpidemiologyTheodoros Kontogiannis100% (1)
- Prob PDFDocumento12 pagineProb PDFwallace120Nessuna valutazione finora
- GUY Et Al 1994 - Regulation of Colostrum Formation in Beef and Dairy CowsDocumento6 pagineGUY Et Al 1994 - Regulation of Colostrum Formation in Beef and Dairy CowsMonique IndNessuna valutazione finora
- History of SensorDocumento37 pagineHistory of SensornsdewNessuna valutazione finora
- Moretsu Shain (Fanatical Workers) and Yoi Kigyo Senshi (Good Corporate Soldiers)Documento7 pagineMoretsu Shain (Fanatical Workers) and Yoi Kigyo Senshi (Good Corporate Soldiers)Erwin Alvih Taufik HidayatNessuna valutazione finora
- MBB 1 Handout 1 and What About BiotechnologyDocumento4 pagineMBB 1 Handout 1 and What About BiotechnologyMariah Shanice BasaNessuna valutazione finora
- Lidocaine Spray On An Endoscope Immediately Before Gi-5-067Documento5 pagineLidocaine Spray On An Endoscope Immediately Before Gi-5-067Byung ChaNessuna valutazione finora
- Wellness Check PrintableDocumento2 pagineWellness Check PrintablethubtendrolmaNessuna valutazione finora
- Ceohns Disease ECCO Guideline SumarizedDocumento19 pagineCeohns Disease ECCO Guideline Sumarizednishad nilangaNessuna valutazione finora