Potrebbero piacerti anche
- Mode of Presentation TBDocumento7 pagineMode of Presentation TBSohaib Abbas MalikNessuna valutazione finora
- Cryptococcal Infection in Plhiv: Series of 12 Cases at The Laboratory of Mohammed Vi University Hospital of MarrakechDocumento6 pagineCryptococcal Infection in Plhiv: Series of 12 Cases at The Laboratory of Mohammed Vi University Hospital of MarrakechIJAR JOURNALNessuna valutazione finora
- Desprendimiento de RetinaDocumento8 pagineDesprendimiento de RetinaDiana Carolina RodríguezNessuna valutazione finora
- 2016 Article 310Documento6 pagine2016 Article 310Gracie ShemaNessuna valutazione finora
- Journal Homepage: - : Manuscript HistoryDocumento8 pagineJournal Homepage: - : Manuscript HistoryIJAR JOURNALNessuna valutazione finora
- Aids and EyeDocumento8 pagineAids and EyeAndreas OctavianoNessuna valutazione finora
- Uveitis-A Rare Disease Often Associated With Systemic Diseases and Infections - A Systematic Review of 2619 PatientsDocumento7 pagineUveitis-A Rare Disease Often Associated With Systemic Diseases and Infections - A Systematic Review of 2619 PatientsnovywardanaNessuna valutazione finora
- Case Report: Tuberculous Scleritis A Challenging DiagnosticDocumento10 pagineCase Report: Tuberculous Scleritis A Challenging DiagnosticIJAR JOURNALNessuna valutazione finora
- Ni Hms 820468Documento41 pagineNi Hms 820468Sohaib Abbas MalikNessuna valutazione finora
- Vasculitis Vih VegaDocumento7 pagineVasculitis Vih VegaOrfa Esther Barrios PazosNessuna valutazione finora
- Sicca Syndrome in Patients HIVDocumento6 pagineSicca Syndrome in Patients HIVkagone walidNessuna valutazione finora
- Jurding Mata EndophthalamitisDocumento24 pagineJurding Mata EndophthalamitisBenk Setsuna F. SeieiNessuna valutazione finora
- 1 s2.0 S003962571630090X MainDocumento14 pagine1 s2.0 S003962571630090X MainBenjamin NgNessuna valutazione finora
- Indian J OphthalmolDocumento16 pagineIndian J OphthalmolfathiaRNessuna valutazione finora
- The Egyptian Journal of Critical Care Medicine: Ahmed Abdelrazik Othman, Mohsen Salah AbdelazimDocumento3 pagineThe Egyptian Journal of Critical Care Medicine: Ahmed Abdelrazik Othman, Mohsen Salah AbdelazimAquardoleo ValentinoNessuna valutazione finora
- 2021 Amaylia Oehadian - Putri - Uun - Bahti - Evan - Jeffery (U) - Erythropoiesis Differences in Various ClinicalDocumento6 pagine2021 Amaylia Oehadian - Putri - Uun - Bahti - Evan - Jeffery (U) - Erythropoiesis Differences in Various ClinicalEvan SusandiNessuna valutazione finora
- RequestedDocumento9 pagineRequestedGaurav MauryaNessuna valutazione finora
- Uveitis and Systemic DiseasesDocumento50 pagineUveitis and Systemic DiseasesAnumeha JindalNessuna valutazione finora
- SMW 09797 PDFDocumento9 pagineSMW 09797 PDFEJ AguilarNessuna valutazione finora
- AygunDocumento5 pagineAygunotheasNessuna valutazione finora
- Pneumocystis in Patients Living With Hiv: Experience of The Infectious Diseases Department of Chu Mohamed Vi-MarrakechDocumento10 paginePneumocystis in Patients Living With Hiv: Experience of The Infectious Diseases Department of Chu Mohamed Vi-MarrakechIJAR JOURNALNessuna valutazione finora
- Clinical Profile of Tubercular Uveitis in A Tertiary Care Ophthalmic CentreDocumento3 pagineClinical Profile of Tubercular Uveitis in A Tertiary Care Ophthalmic CentreArif BudimanNessuna valutazione finora
- A Case Series of Ocular Manifestations in TuberculosisDocumento4 pagineA Case Series of Ocular Manifestations in TuberculosisInternational Journal of Innovative Science and Research TechnologyNessuna valutazione finora
- Internal Medicine Journal - 2021 - Chang - Consensus Guidelines For The Diagnosis and Management of Cryptococcosis and RareDocumento25 pagineInternal Medicine Journal - 2021 - Chang - Consensus Guidelines For The Diagnosis and Management of Cryptococcosis and RareumayamajidNessuna valutazione finora
- Neurological Manifestations of HIV Infection: Mohammed MZ, Venugopal KDocumento6 pagineNeurological Manifestations of HIV Infection: Mohammed MZ, Venugopal KSadam Yondaime AriesNessuna valutazione finora
- Tugas Akademik 12-Journal Reading 3-Infeksi Dan Imunologi-Usamah HaidarDocumento6 pagineTugas Akademik 12-Journal Reading 3-Infeksi Dan Imunologi-Usamah HaidarUsamah HaidarNessuna valutazione finora
- Pyogenic Brain Abscess A 15 Year SurveryDocumento10 paginePyogenic Brain Abscess A 15 Year SurverySilvia RoseNessuna valutazione finora
- Our Experience With Bicytopenia in Patients Treated at The Ankara Hospital Pediatric ClinicDocumento5 pagineOur Experience With Bicytopenia in Patients Treated at The Ankara Hospital Pediatric ClinicRonny DoankNessuna valutazione finora
- 1 s2.0 S1876034120304603 MainDocumento6 pagine1 s2.0 S1876034120304603 MainNeysaAzaliaEfrimaisaNessuna valutazione finora
- Pathomorphological Peculiarities of Tuberculous Meningoencephalitis Associated With HIV InfectionDocumento6 paginePathomorphological Peculiarities of Tuberculous Meningoencephalitis Associated With HIV InfectionBesseMarwah AgusHusainNessuna valutazione finora
- TID 9999 E13413Documento5 pagineTID 9999 E13413saraabolghasemi1Nessuna valutazione finora
- 4Documento16 pagine4Ihsanul Ma'arifNessuna valutazione finora
- Ocular Involvement and Visual Outcome of Herpes Zoster Ophthalmicus: Review of 45 Patients From Tunisia, North AfricaDocumento6 pagineOcular Involvement and Visual Outcome of Herpes Zoster Ophthalmicus: Review of 45 Patients From Tunisia, North AfricaGiorgos MousterisNessuna valutazione finora
- Intracranial MucormycosisDocumento3 pagineIntracranial Mucormycosisdrabrar waniNessuna valutazione finora
- Nebulized Colistin in The Treatment of Pneumonia Due To Multidrug-Resistant Acinetobacter Baumannii and Pseudomonas AeruginosaDocumento4 pagineNebulized Colistin in The Treatment of Pneumonia Due To Multidrug-Resistant Acinetobacter Baumannii and Pseudomonas AeruginosaPhan Tấn TàiNessuna valutazione finora
- Ijccm 25 S150Documento5 pagineIjccm 25 S150Carlos MejiaNessuna valutazione finora
- Neuro-Ophthalmological Biomarkers of Visual Outcome in Newly Diagnosed Idiopathic Intracranial HypertensionDocumento8 pagineNeuro-Ophthalmological Biomarkers of Visual Outcome in Newly Diagnosed Idiopathic Intracranial HypertensionMira TamilaNessuna valutazione finora
- JCDR 11 TC06 PDFDocumento4 pagineJCDR 11 TC06 PDFPutra PratamaNessuna valutazione finora
- Guillain Barre Syndrome: A Clinical Observational Study in Indian Paediatric PatientsDocumento5 pagineGuillain Barre Syndrome: A Clinical Observational Study in Indian Paediatric PatientsLeonardo Antonio Castillo ZegarraNessuna valutazione finora
- RMV 2107Documento6 pagineRMV 2107Ahmed AllamNessuna valutazione finora
- A Clinical Study of Anterior Uveitis in A Rural Hospital: DR - Anitha.S.Maiya, DR - Sundip ShenoyDocumento5 pagineA Clinical Study of Anterior Uveitis in A Rural Hospital: DR - Anitha.S.Maiya, DR - Sundip ShenoyTri BasukiNessuna valutazione finora
- Herpes Zoster & KatarakDocumento6 pagineHerpes Zoster & KatarakSteve aokiNessuna valutazione finora
- Sepsis in The Newborn - Latest NewsDocumento13 pagineSepsis in The Newborn - Latest NewsBrunaNessuna valutazione finora
- Viral Acute Anterior Uveitis: Clinical Signs Useful For Differential DiagnosisDocumento9 pagineViral Acute Anterior Uveitis: Clinical Signs Useful For Differential DiagnosisDiah Rindayani HasbiNessuna valutazione finora
- Jurnal 16Documento9 pagineJurnal 16Putri Intan SolehahNessuna valutazione finora
- Diagnostic Challenge of Tuberculosis in Systemic Lupus ErythematosusDocumento9 pagineDiagnostic Challenge of Tuberculosis in Systemic Lupus ErythematosusBelinda Putri agustiaNessuna valutazione finora
- Tuberculomas of The Brain With and Without Associated Meningitis: A Cohort of 28 Cases Treated With Anti-Tuberculosis Drugs at A Tertiary Care CentreDocumento4 pagineTuberculomas of The Brain With and Without Associated Meningitis: A Cohort of 28 Cases Treated With Anti-Tuberculosis Drugs at A Tertiary Care CentreDestyNessuna valutazione finora
- Sun 2012Documento6 pagineSun 2012ntnquynhproNessuna valutazione finora
- International Journal of Infectious Diseases: A.G. Vos, M.W.M. Wassenberg, J. de Hoog, J.J. OosterheertDocumento7 pagineInternational Journal of Infectious Diseases: A.G. Vos, M.W.M. Wassenberg, J. de Hoog, J.J. OosterheertSohaib Abbas MalikNessuna valutazione finora
- Research Article: Neutropenic Sepsis in The ICU: Outcome Predictors in A Two-Phase Model and Microbiology FindingsDocumento9 pagineResearch Article: Neutropenic Sepsis in The ICU: Outcome Predictors in A Two-Phase Model and Microbiology Findings28121998Nessuna valutazione finora
- mc7 Impact of HIV and AIDS On Surgical PracticeDocumento5 paginemc7 Impact of HIV and AIDS On Surgical PracticeRichard EscalonaNessuna valutazione finora
- Aspergilosis InvasivoDocumento13 pagineAspergilosis InvasivoVeronica ZendejasNessuna valutazione finora
- Lucas 2014Documento8 pagineLucas 2014Prima YosiNessuna valutazione finora
- JCM 12 03447 v2Documento11 pagineJCM 12 03447 v2Marcellia AngelinaNessuna valutazione finora
- Candidiasis in PICUDocumento6 pagineCandidiasis in PICUMeirinda HidayantiNessuna valutazione finora
- Envenimations ViperinesDocumento6 pagineEnvenimations ViperinesIJAR JOURNALNessuna valutazione finora
- Acta Med Iran 2013 51 2 113 118 PDFDocumento6 pagineActa Med Iran 2013 51 2 113 118 PDFbreNessuna valutazione finora
- Jurnal MataDocumento7 pagineJurnal MataKurnia22Nessuna valutazione finora
- SJAMS 66 2563 2566 C PDFDocumento4 pagineSJAMS 66 2563 2566 C PDFVitta Kusma WijayaNessuna valutazione finora
- Detailed Lesson Plan in Science 7: Ii. Subject MatterDocumento6 pagineDetailed Lesson Plan in Science 7: Ii. Subject Matterpinky señaNessuna valutazione finora
- Paper Pet ProjectDocumento27 paginePaper Pet Projectapi-406104878Nessuna valutazione finora
- Introduction To Biochemistry: by Zaheer Uddin (Pharm-D, M Phil (Pharmacy Practice) MBA (MARKETING)Documento63 pagineIntroduction To Biochemistry: by Zaheer Uddin (Pharm-D, M Phil (Pharmacy Practice) MBA (MARKETING)Izat KhanNessuna valutazione finora
- 1 s2.0 S1550413116306519 MainDocumento20 pagine1 s2.0 S1550413116306519 MainMaharani Sari NastitiNessuna valutazione finora
- What Are The Biological Agents That Can Be Utilized For Bioterrorism?Documento30 pagineWhat Are The Biological Agents That Can Be Utilized For Bioterrorism?anukriti shrivastavaNessuna valutazione finora
- The DermatopyteDocumento20 pagineThe Dermatopyteaufa QooNessuna valutazione finora
- NeoplasiaDocumento9 pagineNeoplasiaRinaldo GintingNessuna valutazione finora
- RIBOZYMESDocumento17 pagineRIBOZYMESSharan GayathrinathanNessuna valutazione finora
- Lac OperonDocumento14 pagineLac Operonsony_arora10% (1)
- Marek's Disease: Navigation SearchDocumento18 pagineMarek's Disease: Navigation SearchSUTHANNessuna valutazione finora
- BTR Offline Day 3Documento176 pagineBTR Offline Day 3vivekanurag97Nessuna valutazione finora
- ML 101 Reviewer - 1st ExamDocumento7 pagineML 101 Reviewer - 1st ExamJane EbascoNessuna valutazione finora
- Antigen and Antibody ReactionDocumento27 pagineAntigen and Antibody ReactionHusnain AliNessuna valutazione finora
- Immunoassay TestsDocumento21 pagineImmunoassay TestsDewi PradnyaNessuna valutazione finora
- Innate and Adaptive Immunity: - Innate Is FIRST LINE OF DEFENCE: No Prior Exposure Needed - Comprised OfDocumento31 pagineInnate and Adaptive Immunity: - Innate Is FIRST LINE OF DEFENCE: No Prior Exposure Needed - Comprised OfBegumHazinNessuna valutazione finora
- 1st Lecture History of Molecular BiologyDocumento52 pagine1st Lecture History of Molecular BiologyShanza SyedNessuna valutazione finora
- Hardy Weinberg Law WorksheetDocumento4 pagineHardy Weinberg Law WorksheetThanos GamingNessuna valutazione finora
- Seminar On Breast Feeding, Types, Advantages, Disadvantages, Signs of Good Attachment, Hormones InvolvedDocumento43 pagineSeminar On Breast Feeding, Types, Advantages, Disadvantages, Signs of Good Attachment, Hormones InvolvedTHONDYNALU100% (3)
- BordetellaDocumento54 pagineBordetellatummalapalli venkateswara rao100% (2)
- Fournier GangreneDocumento16 pagineFournier GangreneAmirah Dahalan100% (1)
- CHN TransesDocumento82 pagineCHN Transeskint manlangitNessuna valutazione finora
- PlasmodiumDocumento46 paginePlasmodiumMuna MaranNessuna valutazione finora
- Pharmacology and Venipuncture Nosocomial InfectionDocumento55 paginePharmacology and Venipuncture Nosocomial InfectionArvic Pascua MaltizoNessuna valutazione finora
- Knowledge, Attitude and Practices On Vaccination During Time of Pandemic Among Pediatrician of Olongapo City, Zambales, PhilippinesDocumento15 pagineKnowledge, Attitude and Practices On Vaccination During Time of Pandemic Among Pediatrician of Olongapo City, Zambales, PhilippinesNiran ThapaNessuna valutazione finora
- Flow Cytometry Application Note 13 Color Panel T Cell Subsets Whole BloodDocumento17 pagineFlow Cytometry Application Note 13 Color Panel T Cell Subsets Whole BloodTksAchaNessuna valutazione finora
- Progressive Myoclonic - Genetic Therapeutic - Lancet 2005 (Shahwan)Documento10 pagineProgressive Myoclonic - Genetic Therapeutic - Lancet 2005 (Shahwan)chintanNessuna valutazione finora
- Tocilizumab For Treatment Patients With COVID-19 - Recommended Medication For Novel Disease.Documento8 pagineTocilizumab For Treatment Patients With COVID-19 - Recommended Medication For Novel Disease.Ginna Paola SaavedraNessuna valutazione finora
- Infectious Diseases in Pediatric Otolaryngology - Infections of The External EarDocumento14 pagineInfectious Diseases in Pediatric Otolaryngology - Infections of The External EarGading AuroraNessuna valutazione finora
- K - 1 Perspective and The Future of OncologyDocumento36 pagineK - 1 Perspective and The Future of OncologyPRAGAATHYRAJANNessuna valutazione finora
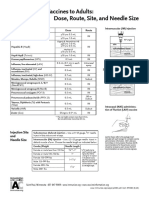
- Administering Vaccines To Adults: Dose, Route, Site, and Needle SizeDocumento1 paginaAdministering Vaccines To Adults: Dose, Route, Site, and Needle SizeAkashNessuna valutazione finora
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionDa EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionValutazione: 4 su 5 stelle4/5 (404)
- The Age of Magical Overthinking: Notes on Modern IrrationalityDa EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityValutazione: 4 su 5 stelle4/5 (34)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDDa EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDValutazione: 5 su 5 stelle5/5 (4)
- Love Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)Da EverandLove Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)Valutazione: 3 su 5 stelle3/5 (1)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsDa EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsValutazione: 4 su 5 stelle4/5 (4)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedDa EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedValutazione: 4.5 su 5 stelle4.5/5 (82)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeDa EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeValutazione: 4.5 su 5 stelle4.5/5 (254)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsDa EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsValutazione: 4.5 su 5 stelle4.5/5 (170)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsDa EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNessuna valutazione finora
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeDa EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeValutazione: 2 su 5 stelle2/5 (1)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisDa EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisValutazione: 4.5 su 5 stelle4.5/5 (44)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsDa EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsValutazione: 5 su 5 stelle5/5 (1)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaDa EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaValutazione: 4.5 su 5 stelle4.5/5 (266)
- Manipulation: The Ultimate Guide To Influence People with Persuasion, Mind Control and NLP With Highly Effective Manipulation TechniquesDa EverandManipulation: The Ultimate Guide To Influence People with Persuasion, Mind Control and NLP With Highly Effective Manipulation TechniquesValutazione: 4.5 su 5 stelle4.5/5 (1412)
- The Twentysomething Treatment: A Revolutionary Remedy for an Uncertain AgeDa EverandThe Twentysomething Treatment: A Revolutionary Remedy for an Uncertain AgeValutazione: 4.5 su 5 stelle4.5/5 (2)
- The Obesity Code: Unlocking the Secrets of Weight LossDa EverandThe Obesity Code: Unlocking the Secrets of Weight LossValutazione: 4 su 5 stelle4/5 (6)
- To Explain the World: The Discovery of Modern ScienceDa EverandTo Explain the World: The Discovery of Modern ScienceValutazione: 3.5 su 5 stelle3.5/5 (51)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Da EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Valutazione: 4.5 su 5 stelle4.5/5 (110)
- When the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisDa EverandWhen the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisValutazione: 3.5 su 5 stelle3.5/5 (2)
- The Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsDa EverandThe Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsNessuna valutazione finora
- Hearts of Darkness: Serial Killers, The Behavioral Science Unit, and My Life as a Woman in the FBIDa EverandHearts of Darkness: Serial Killers, The Behavioral Science Unit, and My Life as a Woman in the FBIValutazione: 4 su 5 stelle4/5 (20)
- Why We Die: The New Science of Aging and the Quest for ImmortalityDa EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityValutazione: 4.5 su 5 stelle4.5/5 (6)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryDa EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryValutazione: 4 su 5 stelle4/5 (46)