Potrebbero piacerti anche
- Confirmation of Satanding PDFDocumento3 pagineConfirmation of Satanding PDFDavidForloyoNessuna valutazione finora
- Appeal and Pending Review FormsDocumento5 pagineAppeal and Pending Review FormsAnbaraj ArunNessuna valutazione finora
- Medication Plan and Discharge SummaryDocumento9 pagineMedication Plan and Discharge SummaryZaharia AlexandrNessuna valutazione finora
- Hotel ManagementDocumento34 pagineHotel ManagementGurlagan Sher GillNessuna valutazione finora
- PEMEDocumento3 paginePEMEEvangeline Antonio-TorresNessuna valutazione finora
- Dangerous Drugs Act 1952 (Consolidated To No 23 of 1990) PDFDocumento11 pagineDangerous Drugs Act 1952 (Consolidated To No 23 of 1990) PDFdesmond100% (1)
- List of Medical Tests For Saudi Visa - Life in Saudi ArabiaDocumento9 pagineList of Medical Tests For Saudi Visa - Life in Saudi Arabiakillerhigh100% (2)
- Medical Claim Form (Reimbursement Only)Documento2 pagineMedical Claim Form (Reimbursement Only)Muhammad Rizwan Tariq100% (1)
- SSS Form CLD-9NDocumento2 pagineSSS Form CLD-9NCat LedesmaNessuna valutazione finora
- MediHub Request For Letter of Guarantee Form 2021 v2 2 1 - 1Documento2 pagineMediHub Request For Letter of Guarantee Form 2021 v2 2 1 - 1Lhogeswaran RaviNessuna valutazione finora
- Records ReleaseDocumento1 paginaRecords ReleasechelseaNessuna valutazione finora
- Application Form For Reimbursement of Mdedical Charges in Respect of Pips EmployeesDocumento2 pagineApplication Form For Reimbursement of Mdedical Charges in Respect of Pips EmployeesNaveed Aman SafiNessuna valutazione finora
- Format For Medical Reimbursement-1Documento5 pagineFormat For Medical Reimbursement-1hemantaduttaghy1Nessuna valutazione finora
- Bajaj AllianzDocumento2 pagineBajaj AllianzKashish BangaloreNessuna valutazione finora
- MAP Application Form (Rev20230719)Documento3 pagineMAP Application Form (Rev20230719)Jen EugenioNessuna valutazione finora
- Clinical Volunteer ApplicationDocumento3 pagineClinical Volunteer ApplicationAnonymous tS0WWCCNessuna valutazione finora
- Data Privacy Consent:: General Evaluation FormDocumento2 pagineData Privacy Consent:: General Evaluation FormIreish Mae RutaNessuna valutazione finora
- Observer Application: General Personal InformationDocumento3 pagineObserver Application: General Personal InformationDragomir IsabellaNessuna valutazione finora
- Senior Residents & Senior Demonstrators - Annexure 1 & IIDocumento3 pagineSenior Residents & Senior Demonstrators - Annexure 1 & IIsarath6872Nessuna valutazione finora
- Instructions To The Assignee: Please Follow The Steps Outlined Below Immediately To Avoid Unnecessary DelaysDocumento12 pagineInstructions To The Assignee: Please Follow The Steps Outlined Below Immediately To Avoid Unnecessary DelaysLoganBohannonNessuna valutazione finora
- Pre AuthorizationForPertrochantericFractureDocumento2 paginePre AuthorizationForPertrochantericFracturepatrickarilloNessuna valutazione finora
- Application Med. Re-ImbDocumento2 pagineApplication Med. Re-Imbzahid hussainNessuna valutazione finora
- Acfrogbo ZR Yavmao RZ No1aftdazyjfq 7lqb Pnhtkqb6m5dp1xcygg2b38 Ifk8cvklo40xcq2j5uqxtb5jwzvgrwzssliqzlyuxdwzplaglu597wcdop8igqqDocumento3 pagineAcfrogbo ZR Yavmao RZ No1aftdazyjfq 7lqb Pnhtkqb6m5dp1xcygg2b38 Ifk8cvklo40xcq2j5uqxtb5jwzvgrwzssliqzlyuxdwzplaglu597wcdop8igqqKhay Gillesania MasulaNessuna valutazione finora
- In-Patient Claim FormDocumento2 pagineIn-Patient Claim Formfaisal_1241Nessuna valutazione finora
- Sss 02Documento2 pagineSss 02June CruzNessuna valutazione finora
- Adamjee Insurance Company Limited: Health Insurance - In-Patient Claim FormDocumento2 pagineAdamjee Insurance Company Limited: Health Insurance - In-Patient Claim FormubaidNessuna valutazione finora
- Medical CertificateDocumento2 pagineMedical CertificateBhem Fernandez RomeroNessuna valutazione finora
- Annex A, B, and CDocumento6 pagineAnnex A, B, and CJOHN GABRIEL CABIAANNessuna valutazione finora
- Medical Reimbursement FormDocumento2 pagineMedical Reimbursement FormMEMOONA ASHARNessuna valutazione finora
- MedicalVerification PDFDocumento3 pagineMedicalVerification PDFOptical RecoveryNessuna valutazione finora
- Credential IngDocumento13 pagineCredential Ingdr_rajatjainNessuna valutazione finora
- 'NEXtCARE UAE - ASOAP FormDocumento1 pagina'NEXtCARE UAE - ASOAP FormMohyee Eldin RagebNessuna valutazione finora
- Toddler QuestionaireDocumento3 pagineToddler Questionaireanarki85Nessuna valutazione finora
- HMRM RECORD DoccDocumento13 pagineHMRM RECORD DoccBharath BeeNessuna valutazione finora
- Observership ApplicationDocumento3 pagineObservership ApplicationMatheus AzevedoNessuna valutazione finora
- Medical Fitness Form PDFDocumento4 pagineMedical Fitness Form PDFKartikeya BagraNessuna valutazione finora
- QR-RCP-009 Authorization For Disclosure of Health InformationRecords - Rev07Documento1 paginaQR-RCP-009 Authorization For Disclosure of Health InformationRecords - Rev07Yel BNessuna valutazione finora
- 3 VSR Updated Form (6-3-2021) 2Documento5 pagine3 VSR Updated Form (6-3-2021) 2Zeeshan KhanNessuna valutazione finora
- 2020-Observership ApplicationDocumento10 pagine2020-Observership ApplicationShirley RamirezNessuna valutazione finora
- TUE - WADA Version 2016-EnDocumento4 pagineTUE - WADA Version 2016-EnYannick MOSSUSNessuna valutazione finora
- CLAIMS RE FORM Reimb - Claim Form PDFDocumento1 paginaCLAIMS RE FORM Reimb - Claim Form PDFMichael Ortega LigaligNessuna valutazione finora
- MED-F-018 OPD-Dentist Assessment PEADSDocumento3 pagineMED-F-018 OPD-Dentist Assessment PEADSdrakmalik71Nessuna valutazione finora
- UIICHdfc ClaimformDocumento2 pagineUIICHdfc ClaimformdomyomglolNessuna valutazione finora
- Idoc - Pub Medical Check Up FormDocumento4 pagineIdoc - Pub Medical Check Up FormBobly SweaggerNessuna valutazione finora
- Med Informed ConsentDocumento2 pagineMed Informed ConsentprabhaNessuna valutazione finora
- Indian Provisional Permanent RegistrationDocumento8 pagineIndian Provisional Permanent Registrationrameshshah765Nessuna valutazione finora
- CLAIMS REIMBURSEMENT FORM EditedDocumento1 paginaCLAIMS REIMBURSEMENT FORM EditedOliver SyNessuna valutazione finora
- CA Request Form GraduateDocumento4 pagineCA Request Form GraduateAltaf PNessuna valutazione finora
- Bajaj Allianz General Insurance Company Limited: Claim Form - Domiciliary and OpdDocumento2 pagineBajaj Allianz General Insurance Company Limited: Claim Form - Domiciliary and OpdvkbasavaNessuna valutazione finora
- Format For Medical FitnessDocumento4 pagineFormat For Medical FitnessParas JaniNessuna valutazione finora
- Indian Provisional Permanent RegistrationDocumento8 pagineIndian Provisional Permanent RegistrationUdhayashankar DhayalanNessuna valutazione finora
- Inbound 2401892485776729288Documento3 pagineInbound 2401892485776729288Elrym BanuaNessuna valutazione finora
- Claims Reimbursement Form: Member General InformationDocumento1 paginaClaims Reimbursement Form: Member General InformationHarold TanNessuna valutazione finora
- Last First Middle InitialDocumento3 pagineLast First Middle InitialAsjsjsjsNessuna valutazione finora
- Template of TUE Application FormDocumento4 pagineTemplate of TUE Application FormWilsfunNessuna valutazione finora
- Maxicare Application FormDocumento6 pagineMaxicare Application Formmeniemartin03Nessuna valutazione finora
- NAIC Claim Form PDFDocumento3 pagineNAIC Claim Form PDFMohit BaggaNessuna valutazione finora
- Department of State Academic Exchanges Participant Medical History and Examination FormDocumento8 pagineDepartment of State Academic Exchanges Participant Medical History and Examination FormNurman HidayatNessuna valutazione finora
- Complaint Registration Form Feb26-2016 tcm21-36522Documento8 pagineComplaint Registration Form Feb26-2016 tcm21-36522Sonof GoddNessuna valutazione finora
- Application and Consent For Release of Medical Information PDFDocumento3 pagineApplication and Consent For Release of Medical Information PDFben_coopermanNessuna valutazione finora
- Cross-Training: The Medical Assistant WorkbookDa EverandCross-Training: The Medical Assistant WorkbookNessuna valutazione finora
- How To Control A DC Motor With An ArduinoDocumento7 pagineHow To Control A DC Motor With An Arduinothatchaphan norkhamNessuna valutazione finora
- Convention On The Rights of Persons With Disabilities: United NationsDocumento13 pagineConvention On The Rights of Persons With Disabilities: United NationssofiabloemNessuna valutazione finora
- Properties of Moist AirDocumento11 pagineProperties of Moist AirKarthik HarithNessuna valutazione finora
- Escario Vs NLRCDocumento10 pagineEscario Vs NLRCnat_wmsu2010Nessuna valutazione finora
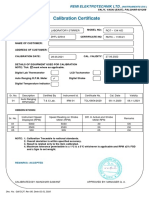
- Calibration CertificateDocumento1 paginaCalibration CertificateSales GoldClassNessuna valutazione finora
- TSB 120Documento7 pagineTSB 120patelpiyushbNessuna valutazione finora
- Hager Pricelist May 2014Documento64 pagineHager Pricelist May 2014rajinipre-1Nessuna valutazione finora
- RENCANA KERJA Serious Inspeksi#3 Maret-April 2019Documento2 pagineRENCANA KERJA Serious Inspeksi#3 Maret-April 2019Nur Ali SaidNessuna valutazione finora
- CoDocumento80 pagineCogdayanand4uNessuna valutazione finora
- Dissertation On Indian Constitutional LawDocumento6 pagineDissertation On Indian Constitutional LawCustomPaperWritingAnnArbor100% (1)
- Office Storage GuideDocumento7 pagineOffice Storage Guidebob bobNessuna valutazione finora
- TEVTA Fin Pay 1 107Documento3 pagineTEVTA Fin Pay 1 107Abdul BasitNessuna valutazione finora
- 3412C EMCP II For PEEC Engines Electrical System: Ac Panel DC PanelDocumento4 pagine3412C EMCP II For PEEC Engines Electrical System: Ac Panel DC PanelFrancisco Wilson Bezerra FranciscoNessuna valutazione finora
- Brochure Ref 670Documento4 pagineBrochure Ref 670veerabossNessuna valutazione finora
- Discover Mecosta 2011Documento40 pagineDiscover Mecosta 2011Pioneer GroupNessuna valutazione finora
- Cryo EnginesDocumento6 pagineCryo EnginesgdoninaNessuna valutazione finora
- Sample Opposition To Motion To Strike Portions of Complaint in United States District CourtDocumento2 pagineSample Opposition To Motion To Strike Portions of Complaint in United States District CourtStan Burman100% (1)
- 1934 PARIS AIRSHOW REPORT - Part1 PDFDocumento11 pagine1934 PARIS AIRSHOW REPORT - Part1 PDFstarsalingsoul8000Nessuna valutazione finora
- Maths PDFDocumento3 pagineMaths PDFChristina HemsworthNessuna valutazione finora
- The Electricity Act - 2003Documento84 pagineThe Electricity Act - 2003Anshul PandeyNessuna valutazione finora
- JAZEL Resume-2-1-2-1-3-1Documento2 pagineJAZEL Resume-2-1-2-1-3-1GirlieJoyGayoNessuna valutazione finora
- PeopleSoft Application Engine Program PDFDocumento17 paginePeopleSoft Application Engine Program PDFSaurabh MehtaNessuna valutazione finora
- Channel Tables1Documento17 pagineChannel Tables1erajayagrawalNessuna valutazione finora
- My CoursesDocumento108 pagineMy Coursesgyaniprasad49Nessuna valutazione finora
- IEC Blank ProformaDocumento10 pagineIEC Blank ProformaVanshika JainNessuna valutazione finora
- MSDS - Tuff-Krete HD - Part DDocumento6 pagineMSDS - Tuff-Krete HD - Part DAl GuinitaranNessuna valutazione finora
- IdM11gR2 Sizing WP LatestDocumento31 pagineIdM11gR2 Sizing WP Latesttranhieu5959Nessuna valutazione finora
- Expense Tracking - How Do I Spend My MoneyDocumento2 pagineExpense Tracking - How Do I Spend My MoneyRenata SánchezNessuna valutazione finora
- Separation PayDocumento3 pagineSeparation PayMalen Roque Saludes100% (1)